 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
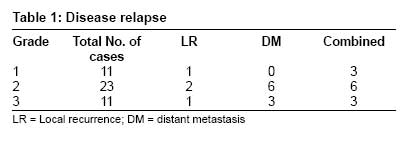
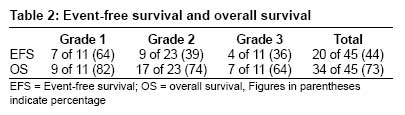
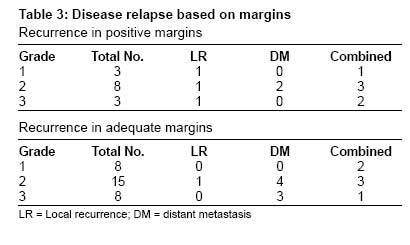
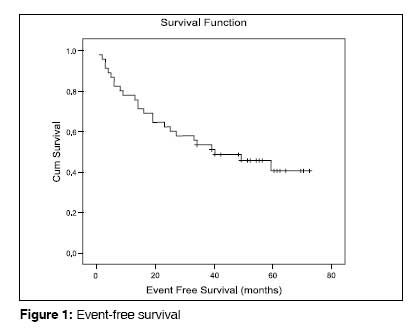
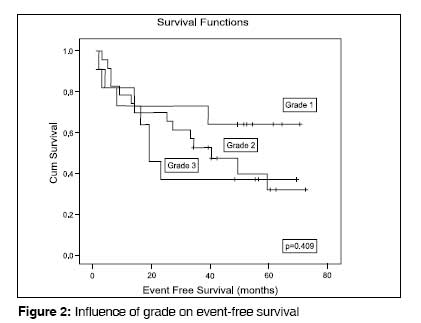
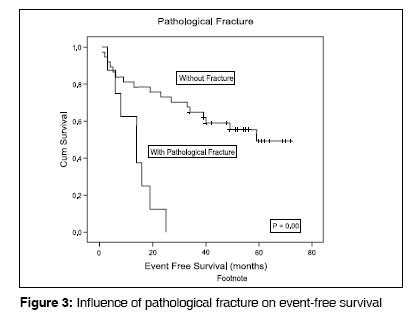
Journal of Cancer Research and Therapeutics, Vol. 5, No. 1, January-March, 2009, pp. 14-19 Original Article Chondrosarcoma of bone: Does the size of the tumor, the presence of a pathologic fracture, or prior intervention have an impact on local control and survival? Puri, Ajay; Shah, Mandip; Agarwal, ManishG; Jambhekar, NirmalaA & Basappa, Prabhudev Department of Orthopaedic Oncology, and Pathology, Tata Memorial Hospital, Room No: 26, E Borges Road, Parel, Mumbai - 400 071, India. Code Number: cr09004 Abstract Aims and Objectives: We studied 45 patients with chondrosarcoma, without metastasis at diagnosis, who were surgically treated between January 2000 and December 2004 to evaluate the risk factors associated with local recurrence and metastasis.Materials and Methods: Fourteen (31%) patients had had some major prior intervention, either in the form of an open biopsy or a curettage / unplanned excision, before presenting to us. Eight patients had pathologic fractures at presentation. None of the patients received adjuvant chemotherapy or radiotherapy. The follow-up duration ranged from 8-75 months. All survivors had a minimum follow-up of 36 months (range 36-75 months). Results: There were 11 grade 1 (24.5%), 23 grade 2 (51%), and 11 grade 3 (24.5%) chondrosarcomas. Thirty-two (71%) patients had tumors that were larger than 8 cm in the greatest dimension. Margins were adequate in 31 patients. Twenty-five patients had disease relapse; there were four local failures, nine distant failures, and 12 combined failures. At the time of the last review, 12 patients had died, 11 were alive with disease, and 22 were free of disease. The cumulative event-free survival was 44% and the overall survival was 73%. Conclusion: Grade of tumor, size of tumor, and adequacy of resection might be important predictors of outcome. Local recurrence is a prelude to distant metastasis and portends poor ultimate survival. The presence of a pathological fracture could indicate biologically aggressive disease, and limb salvage in these cases should be advised with caution. Even in cases where there has been a prior unplanned intervention, local control can be achieved by subsequent adequate resection. Keywords: Chondrosarcoma, local recurrence, metastasis, pathological fracture, prior intervention Introduction Chondrosarcoma is the second most common primary malignant bone tumor after osteosarcoma and the commonest one in patients aged more than 20 years. [1],[2] Surgical resection remains the mainstay of treatment as these tumors do not respond to chemotherapy or radiotherapy. [3] Chondrosarcomas can vary in behavior from being extremely low-grade slowly growing lesions with negligible metastatic potential to highly aggressive, invasive, and metastasizing tumors. Though there is consensus that the histological grade is one of the major factors determining the outcome, certain issues are still debatable. For example: Do larger tumors have a worse prognosis? Is limb salvage safe in pathological fractures in chondrosarcomas, in the absence of effective adjuvant therapy? Does prior unplanned intervention compromise local control in chondrosarcomas? These are some of the questions that we sought to address in this study. Most of the orthopedic oncology data presented in this article is from the western world. There is a paucity of literature from developing countries, where socioeconomic conditions and availability of quality medical care vary from place to place; large tumors, late presentation, and prior unplanned interventions are commoner in these areas. Our study evaluates the outcome of Indian patients with chondrosarcoma, who do not have metastasis at diagnosis; these were all patients treated at a specialist oncology center over a 5-year period. We examined the risk factors associated with local recurrence and systemic metastasis and compared our results with those published in literature.Materials and Methods Between January 2000 and December 2004, 56 patients with chondrosarcoma were surgically treated at our institution, a referral center for oncology. Medical records, radiographs, histological sections, and pathology data were reviewed retrospectively. There were 44 males and 12 females; the mean age was 45 years (range 15-76 years). The pelvis was the commonest site of the lesion (18), followed by the femur (16), humerus (10), tibia (4), foot bones (2), scapula (3), clavicle (1), vertebral body, and fibula (1). Forty-five of these patients were analyzed; 11 patients (two patients with metastasis at presentation, one perioperative mortality, and eight patients who were unavailable for follow-up) were excluded from the analysis. Of the 45 patients analyzed, 14 (31%) patients had had a major prior intervention, either in the form of an open biopsy or a curettage / unplanned excision at a non-oncology center before presenting to us. Eight patients had a pathologic fracture at presentation. Four of 13 (31%) patients with lesions in the femur and three of nine (33%) with humeral lesions presented with pathologic fractures. A tissue diagnosis was obtained preoperatively in all patients. In case slides and blocks prepared at the time of the prior intervention were available, these were reviewed at our institute; if not, a biopsy was performed. In the large majority of cases we preferred a core needle biopsy to obtain tissue. [4],[5] The biopsy results were discussed at a multidisciplinary meeting, which included a radiologist and a pathologist specializing in bone tumors. In all these cases, the tumor matrix was entirely chondroid and no osseous matrix was produced by the tumor cells. Histologically, all tumors showed features of permeative growth into the host bone, both in the biopsy samples and in the resected specimens. This is an important histological feature and defines a cartilaginous tumor as a chondrosarcoma, since low-grade chondrosarcomas can often be confused with enchondromas because the two conditions have an overlapping cytomorphology. The tumors were histologically graded as grades 1, 2, or 3 on the bases on the cellularity, the characteristics of the tumor matrix, the nuclear features, and the mitotic rate. [6] The primary goal of surgery was complete excision of the tumor, with preservation of the limb and useful residual function wherever possible. Amputation was performed in those cases where adequate margins seemed unlikely or in those cases where salvage would result in resection of so much tissue as to render the limb functionless. Surgical margins were evaluated according to the method of Enneking. [7] We considered an adequate surgical margin for chondrosarcoma to be one that was uncontaminated, wide, or radical. Intralesional, marginal, or contaminated margins were regarded as inadequate. The pathology reports were reviewed for histopathologic grading and for assessing margins and the largest tumor dimension in any plane. As studies to assess tumor volume are not routinely done at our institute, the dimensions of the tumor were measured from the excised pathological specimens. Tumors were grouped as less than or larger than 8 cm for the purpose of analysis; we decided on a cutoff value of 8 cm based on the (AJCC) grading. [8] None of the patients received adjuvant chemotherapy or radiotherapy. The follow-up duration ranged from 8 months to 75 months, with a mean of 43 months. All survivors had a minimum follow-up of 36 months (range: 36-75 months; mean: 54 months). Statistical analysis For descriptive statistics we calculated frequencies and percentages. The cumulative rate of survival was calculated according to the Kaplan-Meier method using the log rank test. The event-free survival was calculated from the time of surgery to the first adverse event (i.e., clinically or radiologically detected local or distant recurrence) or to the last follow-up. Results Nine patients had amputation, while 36 patients underwent limb-sparing surgery initially. There were 11 grade 1 (24.5%), 23 grade 2 (51%), and 11 grade 3 (24.5%) chondrosarcomas. Thirty-two (71%) patients had tumors that were larger than 8 cm in the greatest dimension. Margins were adequate in 31 patients. Fourteen patients (31%) had contamination intraoperatively or involved margins; these were considered as inadequate / positive margins. Of these, only one occurred in an amputation. Thus, 13 of 36 patients (36%) with limb salvage and 1 of 9 patients (11%) with amputation had positive margins. Of the eight patients with pathological fractures, seven underwent limb salvage; four of these 7 patients had inadequate margins. At the time of last review 12 patients had died, 11 were alive with disease, and 22 were free of disease. Disease relapse [Table - 1] Twenty-five patients had a disease relapse. There were four local failures, nine distant failures, and 12 combined failures. Four of 11 (36%) patients with grade 1 chondrosarcomas, 14 of 23 (61%) patients with grade 2 chondrosarcomas, and seven of 11 (64%) patients with grade 3 chondrosarcomas had relapses. Of the 25 patients with disease relapse, only two (one local recurrence treated with an amputation and one combined relapse treated with local resection and pulmonary metastectomy) are currently disease free at 36 and 34 months, respectively. The others are either dead or being managed with supportive care. Two patients with only local recurrence refused amputation. Event-free survival and overall survival [Table - 2] At the time of evaluation, cumulative event-free survival (EFS) was 44% (20 of 45) and overall survival (OS) was 73% (33 of 45). Grade 1 tumors had the best EFS and OS and grade 3 tumors had the worst EFS and OS. Local recurrence and margins [Table - 3] Sixteen of 45 (36%) patients had local recurrence. The time taken for development of local recurrence ranged from 2-44 months, with a mean of 15 months. Two patients had local recurrences, one at 40 months and the other at 44 months. In the remaining 14 patients, the maximum time to local recurrence was 33 months. Nine of 14 (64%) patients with positive margins had local recurrence, whereas only seven of 31 (23%) patients with adequate margins had local recurrence. Between January 2000 and December 2002, 28 patients were operated upon, with a local recurrence rate of 43%. Between January 2003 and December 2004, 17 patients were operated, with a local recurrence rate of 24%. Limb salvage or amputation Patients who underwent limb salvage had a higher rate of local relapse but this was not associated with poorer EFS. One of the nine (11%) patients who underwent amputations had local recurrence and 15 of 36 (42%) patients who had limb salvage had local recurrence; however, the EFS was similar in both groups (44%). Local recurrence and distant metastasis [Table - 3] Twelve of 16 (75%) patients with local recurrence had distant metastasis, whereas only nine of 29 (31%) patients without local recurrence had distant metastasis. Two of these nine patients had positive margins, whereas the margins were adequate in the other seven. Site Location (pelvis vs extrapelvic) did not seem to result in a higher rate of local relapse or poorer EFS. Five of 14 (36%) patients with pelvic tumors had local recurrences and 11 of 31 (35%) patients with tumors in an extrapelvic location had local recurrences. The EFS was 43% in patients with pelvic tumors and 45% in patients with tumors in extrapelvic locations ( P = 0.601). Notably, seven of nine (78%) tumors occurring in the humerus had local recurrence. Tumor size Tumors larger than 8 cm had a higher rate of local relapse and tended to be associated with poorer EFS. Two of 13 (15%) patients with tumors less than 8 cm in size had local recurrences, whereas 14 of 32 (44%) patients with tumors larger than 8 cm had local recurrences. The EFS was 69% in patients with tumors less than 8 cm, while it was 34% in patients with tumors larger than 8 cm ( P = 0.105). Pathological fractures One of 11 (9%) grade 1, three of 23 (13%) grade 2, and four of 11 (36%) grade 3 chondrosarcomas presented with pathological fractures. Pathological fractures were associated with the poorest outcome. Seven of 8 (88%) cases had local recurrences. Six of these patients also had distant relapse. The one case that did not have local recurrence developed pulmonary metastasis. Thus all eight patients had recurrence of disease. Prior intervention Prior intervention did not seem to result in a higher rate of local relapse but tended to be associated with poorer EFS. Five of 14 (36%) patients with prior intervention had local recurrence and 11 of 31 (35%) patients without prior intervention had local recurrence. EFS was 36% in patients with prior intervention and 48% in patients without prior intervention ( P = 0.748). Discussion Our patient population could be said to be a homogenous group as they were treated by the same team of clinicians at a specialist oncology center over a relatively short period of time (5 years). Like Fiorenza et al . we have excluded borderline cartilaginous tumors of unknown malignant potential from our series and have elected to use the less subjective 'cutoff' feature of permeative growth of the tumor into adjacent host bone as the criterion for malignancy. [9],[10] Our figures for limb salvage (80%) and amputation (20%) do not necessarily accurately reflect the number of patients unsuitable for limb salvage. There may have been a selection bias as, occasionally, patients found unsuitable for limb salvage were referred back the referring hospital for an amputation due to various reasons. The proportion of patients with low-grade (grade 1) disease is 24.5% in our series, which is lower than that reported in other series. This may have had an impact on the EFS [Figure - 1] and OS seen in our study (44% and 73%, respectively), which is lower than that reported by others in literature. [2],[9],[10] Consistent with the earlier studies, however, an increase in the histological grade seemed to correlate with a poorer outcome [Figure - 2] ( P = 0.409). [1],[10] The definition of 'adequate' margins varies in different series. We have been guided by the criteria described by Enneking. Fiorenza et al . have been more rigid in their definition of 'adequate' margins for patients with chondrosarcoma and this could explain the fact that though our percentage (69%) of adequate margins was higher than theirs, our local control rates were poorer. [9] Our local recurrence rate (36%) is higher than that reported in recent publications. [1],[2],[3],[9],[10] Similar to other studies, there was a demonstrable improvement in our local control rate with increasing experience: [11] the local recurrence rate (24%) in the latter half of the series is similar to that reported in recent publications. All authors have documented poorer outcomes in patients who have had inadequate surgical margins. [1],[2],[3],[9] This is evident in our series too ( P = 0.067). Amputation and limb-preserving surgery have been reported as resulting in similar rates of local control if adequate margins of excision are achieved. [9] We are unable to validate this statement as in our series inadequate margins were three times commoner with limb salvage. Limb salvage was also associated with a higher rate of local relapse. Whether our selection of patients for limb salvage was appropriate is open to question in the light of our inability to achieve adequate margins in one-third of these patients. It is however debatable whether these patients would have benefited from an amputation. In spite of poorer local control, EFS was similar (44%) in both groups. Cases undergoing amputation suffer from a selection bias. These are generally patients with large tumors presenting late and possibly have an inherent poorer prognosis. Despite adequate local control they may still be susceptible to distant metastasis and therefore have poorer survival. Most literature on chondrosarcoma confirms that local failure is a prelude to distant disease and a risk factor for survival. [1],[10],[12] In our series, 75% of patients with local recurrence had distant metastasis, whereas only 31% of patients without local recurrence had distant metastasis. Fiorenza et al . made an interesting observation that the development of a local recurrence was only relevant to survival if the patient already had metastases when the diagnosis of local recurrence was made. In patients without metastases at the time of detection of local recurrence, further radical surgical treatment produced a good chance of long-term cure. In contrast, only 5% of those presenting with a local recurrence and metastases had long-term survival. [9] Because of the small number of patients in our series, we are unable to comment on this aspect. Of the 25 patients with disease relapse, including four who presented with isolated local recurrence, only two are currently disease free; the others are either dead or are being managed with supportive care. Size and pelvic location are two other factors that have been associated with the overall outcome. [1],[9] Though site did not seem to affect the overall outcome, as evidenced by similar local recurrence and EFS in patients with pelvic tumors and those with tumors in extrapelvic locations, size of the tumor did seem to play a role in our study. Tumors larger than 8 cm had a higher rate of local relapse and tended to be associated with poorer EFS. Tumors occurring in the humerus had a higher rate of local recurrence. Poorer local control in the humerus has been documented by other authors as well. [10] Also, pathological fractures are more common in the humerus. [13] Pathological fractures in chondrosarcomas may need to be looked at differently in view of the fact that there is no additional protection in the absence of effective adjuvant therapy in these tumors. Unlike the results reported by other authors, pathological fractures in our series were associated with a very poor outcome [Figure - 3]. [1],[13] The poor local control may be explained by the fact that we were unable to achieve adequate margins in half these patients. Four of eight patients with pathological fractures had inadequate margins. Another contributing factor may have been that in our socioeconomic scenario patients with pathological fractures are often transported over large distances without appropriate immobilization. This can result in wider dissemination of the fracture hematoma, resulting in a higher chance of local recurrence. Like us, others too have noted an increased occurrence of pathological fractures in high-grade chondrosarcomas. [1] A pathological fracture could thus be indirect evidence of biologically more aggressive disease. The number of cases of pathological fracture in our series is small (8) but based on our experience, as well as the fact that there is no additional protection in the absence of effective adjuvant therapy in these tumors, we would exercise caution while recommending limb salvage in chondrosarcomas. In our study, prior intervention did not result in a higher rate of local relapse but these patients did tend to have poorer EFS. The numbers are too small to comment but they do seem to suggest that similar rates of local control are achievable even in patients who have had prior intervention at a non-oncology center. Whether such intervention results in distant dissemination of disease, with an impact on survival, can only be answered by studies with larger numbers of patients. Our study has the inherent limitations of a retrospective evaluation. Additionally, unlike other authors, we have not staged our patients according to the Musculoskeletal Tumor Society staging system. This staging system requires classifying the lesions as intra- or extra-compartmental. One-third of our patients had major prior intervention before presenting to us. Very often, imaging of the index presentation was not available And, after an extensive open biopsy or curettage has been done, it is difficult to comment on whether the tumor was intra- or extra-compartmental at initial presentation. The small number of patients in our study prevents us from validating our observations statistically. The presence of a pathological facture was significantly associated with a poor outcome but none of the other variables that we examined achieved statistical significance, possibly due to the small sample size. Due to the relatively short duration of follow-up we have used EFS as a marker to indicate outcome. A longer follow-up would give a better indication of overall survival. In spite of these shortcomings, we believe that this study does add to the understanding of the behavior of chondrosarcomas. This study also provides an insight into the treatment and outcome of these tumors in the Indian scenario. It reinforces the fact that grade and size of the tumor, and adequacy of resection, might be important predictors of outcome. Local recurrence is a prelude to distant metastasis and portends poor ultimate survival. The presence of a pathological fracture could be an indicator of biologically aggressive disease and limb salvage in these cases should be advised with caution. In spite of prior unplanned intervention, local control can be achieved by subsequent adequate resection. Acknowledgement The authors wish to acknowledge Ms Rohini Hawaldar for her assistance in statistical evaluation of the data and Dr. CS Pramesh for his editorial assistance in preparing the manuscript.References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09004t2.jpg] [cr09004t3.jpg] [cr09004t1.jpg] [cr09004f2.jpg] [cr09004f1.jpg] [cr09004f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}