 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
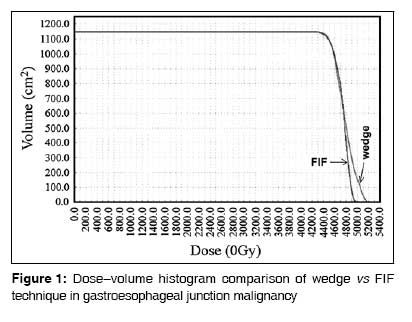
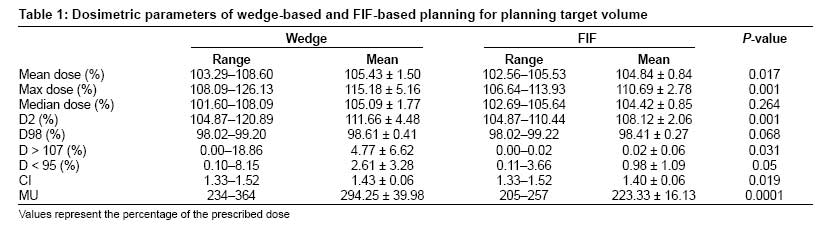
Journal of Cancer Research and Therapeutics, Vol. 5, No. 1, January-March, 2009, pp. 20-23 Original Article Field-in-field technique for upper abdominal malignancies in clinical radiotherapy Prabhakar R, Haresh KP, Kumar M, Sharma DN, Julka PK, Rath GK Department of Radiation Oncology, Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi - 110 029, India Code Number: cr09005 Abstract Background: In upper abdominal malignancies (UAM), due to the presence of multiple inhomogeneous tissues, a wedge-based conformal treatment planning results in high-dose regions inside the target volume.Aim: This study was designed to explore the feasibility of using a field-in-field (FIF) technique in different UAM and its efficacy in reducing the high-dose regions. Materials and Methods: Twelve patients of UAM (which included malignancies of the gastroesophageal junction, stomach, gall bladder, and pancreas) were selected for this study. Computed tomography (CT) scans were performed and three-dimensional conformal wedge plans were generated for all the cases. The same plan was copied with the wedges removed and a FIF plan was generated. The two plans were compared for mean, maximum, and median doses; dose received by 2% (D2) and 98% (D98) of the target volume; volume receiving >107% (V > 107%) and <95% (V < 95%) of the prescribed dose; conformality index (CI); and total monitor units. The doses to critical structures such as liver, kidneys, and spinal cord were also compared. Statistical Analysis: Statistical analysis was performed with SPSS, version 10.0. Results: For all the cases, the FIF technique was better than wedge-based planning in terms of maximum dose, D2, V > 107%, and CI; there was a statistically significant reduction in monitor units. With regard to doses to critical structures, there was marginal dose reduction for the kidneys and spinal cord with FIF as compared to wedge-based planning. Conclusion: The FIF technique can be employed for UAM in place of wedge-based conformal treatment plans. Keywords: Abdominal malignancies, field-in-field, treatment planning, wedge Introduction In upper abdominal malignancies (UAM), due to the presence of multiple inhomogeneous tissues, a wedge-based conformal treatment planning results in high-dose regions inside the target volume. In most centers, the usual method of treating UAM such as cancers of the gastroesophageal junction, stomach, gall bladder, and pancreas is by employing antero posterior/postero anterior fields (AP/PA) or by three fields. The three-field technique is believed to reduce toxicity in most patients. Leong et al. compared an antero posterior/postero anteror (AP/PA) with a 3D conformal technique using a monoisocentric split-field technique and concluded that the 3D conformal technique reduced the dose to the kidneys and spinal cord. [1] Forward planning has been routinely used in the treatment of breast cancer and has been shown to give better dosimetric results as compared to conventional wedge fields [2],[3] and equivalent dosimetric results as compared to inverse planning. [4] It has also been demonstrated that the field-in-field (FIF) technique reduces the dose to contralateral breast. [5] There is little literature available on the use of the FIF technique at other sites. This study was designed to evaluate the feasibility of the FIF technique for UAM.Materials and Methods Twelve patients of UAM were selected for this study. Among these, four had malignancies of the gastroesophageal junction, three of the stomach, three of the gall bladder, and two of the pancreas. All the patients underwent CT scanning with a Siemens Volume Zoom CT TM scanner for 2.5mm slice thicknesses and the CT datasets were transferred to an Eclipse TM treatment planning system through a DICOM network. Following the ICRU 62 recommendations, the planning target volume (PTV) was generated by expanding the clinical target volume by 1cm to compensate for the organ motion and setup error. [6] Plans were generated for a dual-energy (6 and 15MV x-rays) linear accelerator (Clinac 2300C/D TM ) equipped with 40 pairs of multileaf collimators (MLC). A standard three fields, which included one anterior and two lateral fields, were generated for the comparative study. For all the cases, two plans were generated: a wedge- and an FIF-based treatment plan. Initially, wedge-based planning was performed to achieve the best possible dose distribution inside the target volume, with the MLCs ensuring that the surrounding critical structure such as the kidneys, liver, and spinal cord received less than their tolerance limits (plan 1). A copy of the same plan was generated with the wedge removed. The dose was computed with the same beam arrangement and MLC sets. High-dose regions, above 105% of the maximum dose, were shielded with MLCs in steps of 5% dose levels using beams eye view (plan 2). The weights of the MLC segments were adjusted manually to reduce the hotspots till an optimal dose distribution, with better dose homogeneity, was achieved inside the target volume. The two plans, plan 1 and plan 2, were evaluated and compared for the following: mean dose, maximum dose, and median dose; dose received by 2% of the target volume (D2); dose received by 98% of the target volume (D98); volume receiving greater than 107% of the prescribed dose (V > 107%); volume receiving less than 95% of the prescribed dose (V < 95%); and total monitor units required to deliver the plan. Similarly, for the kidneys, the mean dose and volume receiving greater than or equal to 20 Gy of the prescribed dose (V20) were used for comparing the two plans. Here, D2 (lowest dose to the 2% of the 'hottest' volume) and D98 (dose received by at least 98% of the target volume) are considered to be the near-maximum and near-minimum doses to the target volume, respectively. In case of the liver, the mean dose and the volume receiving greater than or equal to 30 Gy (V30) of the prescribed dose were used for comparing plan 1 and plan 2. For the spinal cord, the maximum dose and the maximum dose received by 2 cc volume (D2cc) were used for comparison. Statistical analysis was performed with SPSS version 10.0. Paired Student's t-test with a two-tailed P < 0.05 was used for assessing the statistical significance of the difference between plan 1 and plan 2.Results [Figure - 1] shows the dose-volume histogram comparison of wedge vs FIF technique in a typical case of gastroesophageal junction carcinoma. [Table - 1],[Table - 2],[Table - 3],[Table - 4] show the dosimetric parameters of wedge- and FIF-based planning for PTV, kidneys, liver, and spinal cord, respectively. [Table - 1] shows that there is statistically significant reduction in maximum dose, high-dose regions (D2), and monitor units for FIF as compared to wedge-based treatment planning. For critical structures, there is a marginal dose reduction with FIF as compared to wedge-based planning, especially for the kidneys and spinal cord.Discussion An important observation from our study is that FIF not only reduces the dose inhomogeneity inside the target volume but requires less monitor units for delivering a plan as compared to wedge-based treatment planning; this difference between FIF and wedge-based treatment planning was statistically highly significant. It is due to the fact that in the FIF technique, the monitor units are adjusted among the subfields and even an increase in the number of subfields will not bring about much change in the monitor units. This is the biggest advantage of using the FIF technique in radiotherapy. Intensity-modulated radiation therapy (IMRT) has the advantage of reducing the doses to surrounding critical structures [7] but, in most of the centers, UAM are routinely treated with 3D conformal radiation therapy. In those centers that follow 3D-conformal radiotherapy, the FIF technique can comfortably replace wedge-based planning. An important advantage of FIF over IMRT is that the monitor units can be reduced and, until more information is available regarding radiation-induced secondary malignancies, it would certainly be wise to reduce the monitor units. A recent study by van der Geld et al . has shown that the respiratory-gated radiotherapy technique has not resulted in significant decrease in the renal doses as compared to 3D-conformal radiotherapy or IMRT. [8] Hence, the FIF technique can be safely employed for routine treatment of UAM. The following are some of the advantages of FIF technique over wedge-based planning: (i) It reduces the scattered dose to the patient; (ii) the monitor units can be considerably reduced; (iii) the total time required for treating a patient can be reduced; (iv) some hotspots may persist even after the use of wedge due to extreme tissue inhomogeneities and contour irregularities, and this can be avoided by adopting the FIF technique. The placement of isocenter plays an important role in the FIF technique. After studying, the calculated unwedged plan dose, the isocenter may be shifted to a region where the cold spot occurs in the target volume. This ensures that in the FIF technique the isocenter will not be shielded by any of the MLC subfields. In reality, due to the presence of irregular inhomogeneities and the nonuniform body shape, the use of a wedge does not result in perfect dose uniformity inside the target volume; however, in the case of the FIF technique, the MLCs allows the planner to reduce the high-dose region present in a nonuniform pattern by shielding them. The use of simple static MLC segments does not require any optimization engine and hence FIF technique is simple and easy to plan. With MLCs gradually being incorporated in telecobalt machines, the FIF technique can also be employed to replace the wedges in these machines. Conclusion A comparison between the FIF technique and wedge-based treatment planning shows that FIF is superior to wedge-based treatment planning in terms of reduction in maximum dose and improved dose homogeneity. One of the biggest advantages of the FIF technique is that with FIF there is considerable reduction in the monitor units as compared to wedge-based planning. Hence, we feel that the FIF technique should be employed in place of wedges in routine radiotherapy treatment planning for UAM.References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09005t4.jpg] [cr09005t3.jpg] [cr09005t1.jpg] [cr09005f1.jpg] [cr09005t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}