 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
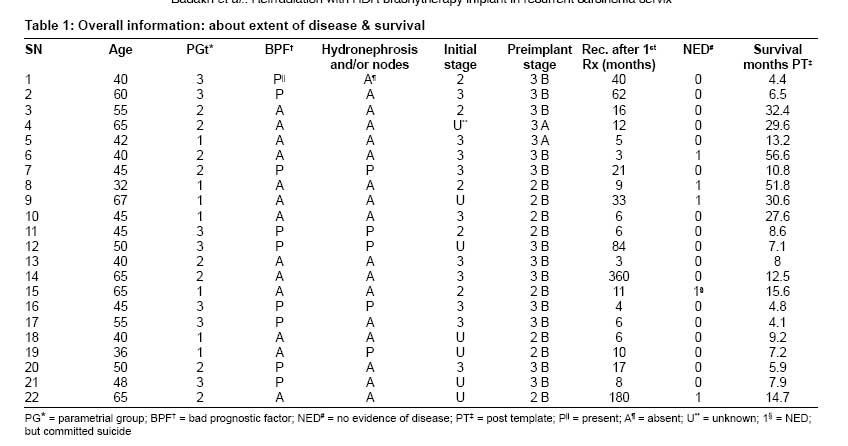
Journal of Cancer Research and Therapeutics, Vol. 5, No. 1, January-March, 2009, pp. 24-30 Original Article Reirradiation with high-dose-rate remote afterloading brachytherapy implant in patients with locally recurrent or residual cervical carcinoma Badakh, Dinesh K.; Grover, Amit H. Dr. D K Gosavi Memorial, Siddhivinayak Ganpati Cancer Hospital, Miraj-Sangli Road, Miraj - 416 410, Maharashtra, India. Code Number: cr09006 Abstract Purpose: To assess the outcome for patients with postradiation locally recurrent or residual cervical malignancies treated with high-dose-rate (HDR) remote afterloading brachytherapy implant. This is a prospective study.Materials and Methods: Twenty-two patients with postradiation recurrent cervical carcinomas were treated with HDR interstitial brachytherapy. All of these 22 patients had received some form of radiotherapy prior to implant placement and had biopsy-proven recurrence. Implant dose for these patients was in the range of 12-45 Gy, with a median dose of 25.80 Gy. Results: Overall survival was better for patients in the 'no bad prognostic factor' (NBPF) group than for patients in the 'bad prognostic factor' (BPF) group and this difference was statistically significant. Overall survival was better for patients who had stage II disease before implant placement than for those who had stage III disease and also for patients who had relatively less parametrial disease. Grade 4 complications were seen only in four patients and were within acceptable limits. Multivariate analysis showed that only the BPF variable had a statistically significant effect on survival. Conclusion: We conclude that reirradiation with HDR brachytherapy implant in recurrent or residual carcinoma cervix can give a good chance of survival, with acceptable morbidity, if proper selection of patients is done. This treatment should not be done for palliative purposes. Keywords: Carcinoma cervix, interstitial brachytherapy, local recurrence Introduction Cervical cancer is the most common cancer of women at our institute, accounting for about one-third of all cancer cases seen by us. Ninety percent of these patients have stage II or stage III disease at diagnosis. A persistent or recurrent malignancy in the pelvis after definitive radiation therapy for carcinoma cervix is not an infrequent occurrence. Surgical salvage is feasible in only a small number of central recurrences and that too with all the associated morbidity and mortality. Surgery, in most of these patients, amounts to either anterior or posterior or total exenteration . [1] The general outcome of recurrent cervical carcinoma following definitive radiation therapy was studied by Sommers et al ., who showed that there was no major difference in survival after recurrence by type of treatment or initial stage of the disease. The overall survival at 5 years for all untreated patients was 1%. [2] Reirradiation with interstitial implant for recurrent carcinoma of the uterine cervix has been tried in the past with radium and radon seeds, but the overall results were poor and there was a high complication rate. Some investigators reirradiated recurrent pelvic carcinoma patients with afterloading perineal low-dose-rate (LDR) brachytherapy implant or iodine-125 seeds and reported some degree of success. We, as a pilot project, selected patients who had recurrent carcinoma cervix after radical or external radiation and treated them with high-dose-rate (HDR) perineal interstitial implant. In this paper, we present our findings. Materials and Methods Between October 1998 and December 2003, 22 patients with postradiation recurrent cervical carcinomas were treated with HDR interstitial brachytherapy, using Martinez Universal Perineal Interstitial Template (MUPIT), in the department of radiation oncology. All of these 22 patients had received some form of radiation prior to implant placement and had a biopsy-proven recurrence. Except for one patient with an adenocarcinoma, all had histologically proven squamous cell carcinoma. Six patients had received only external radiation (incomplete treatment), and three patients had undergone hysterectomy and had received postoperative radiation; the remaining patients had received radical radiation therapy with external radiation and intracavitary brachytherapy (LDR or HDR) prior to the recurrence. These patients had received treatment prior to recurrence at different radiation centers, including ours. Some patients had late recurrences after initial treatment for carcinoma cervix [Table - 1]; they were included in the study although they could also be labeled as patients with a second primary. Criteria for inclusion in this study were as follows:
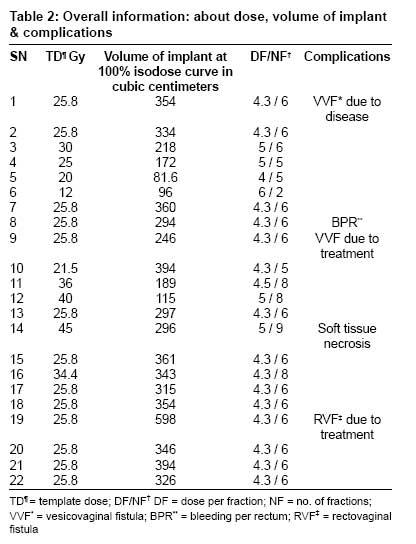
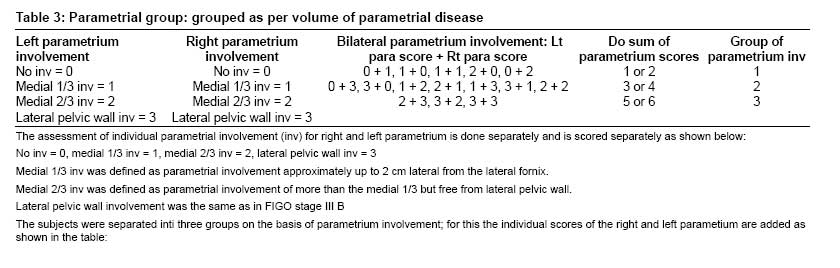
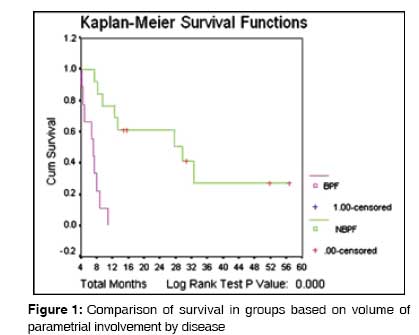
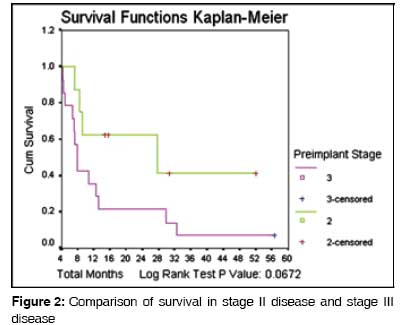
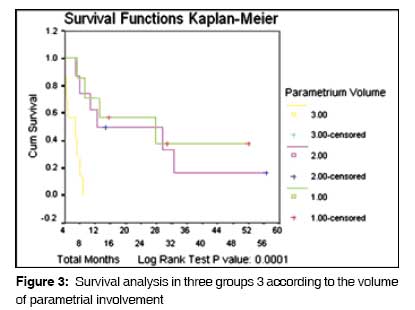
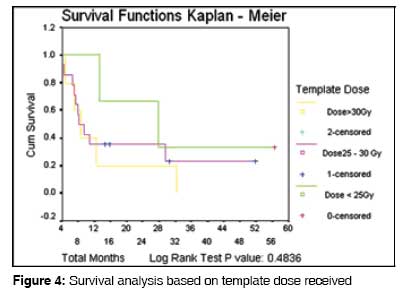
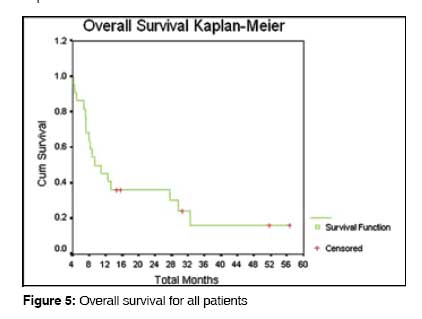
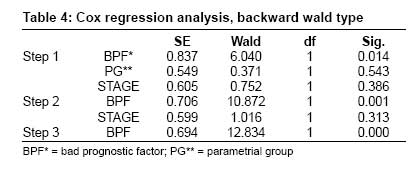
Metastatic workup included chest x-ray and ultrasonography of the abdomen and pelvis. The 22 patients were treated with perineal implants. Follow-up was available for all patients; they were followed either until their death or, if alive, until a recent follow-up (in the latter part of the year 2004). Some patients were regular with their follow-up, but in the case of others information had to be obtained by making home visits or, if that was not feasible, by follow-up letters or by telephone interviews. All details of these patients are given in [Table - 1] and [Table - 2]. Staging was done on the basis of the findings from examination under anesthesia done before implant placement; we used the criteria given by the International Federation of Gynecology and Oncology (FIGO) for staging of primary carcinoma of the cervix. SPSS 10 software was used for statistical analysis. Survival time was calculated from the day of implant placement. Analysis was done for overall survival. Comparison between groups was performed using univariate analysis and statistical significance was assumed at P ≤ 0.05 level (at 95% confidence interval). Kaplan-Meier survival curves were plotted and compared with the log rank test; The results of comparison of Kaplan - Meier survival curves by log rank test are given below each graph are given below each curve. Multivariate analysis was done using Cox regression analysis (backward Wald) for only those variables that showed a statistically significant difference on univariate analysis or the log rank test or both. Results The median age of the patients was 46.5 years (range 32-67 years). The minimum survival of these patients was 4.1 months, the maximum survival was 56.6 months at last follow-up, and the median survival was 9.2 months. After template treatment, five of the 22 patients (22.7%) had no evidence of disease (NED). One of these five NED patients had committed suicide because of problems unrelated to the disease (as verified by a home visit); for this patient, follow-up was available for 15.6 months, and she was considered as NED during analysis. One NED patient had follow-up of only 14.7 months because her implant was done in November 2003; the other three NED patients had follow-up of over 30 months. The template dose given was in the range of 12-45 Gy (median dose: 25.8 Gy). Those patient who had recurrence after long gap with higher doses with template- guided radiation techniques. All these patients received twice-a-day treatment with the dose per fraction ranging from 4 Gy to 6 Gy and the median dose being 4.3 Gy, at a 100% isodose curve. Patients were treated, twice daily for 3-5 consecutive days, depending upon the number of fractions given. The cumulative rectal and bladder doses in most of these patients cannot be stated accurately as many of these patients were treated in other institutions before the implant. Thus the exact rectal and bladder doses were not known. The rectal dose for these implant patients was in the range of 7-31.5 Gy, with a median dose of 20 Gy; the bladder dose was in the range of 11.4-51.3 Gy, with a median dose of 34.2 Gy. These rectal and bladder doses are for the point receiving maximum dose. Patients were grouped into three groups as per volume of parametrial involvement by disease as shown in [Table - 3]. For analysis, the patients were divided into two groups: Patient were grouped into three groups as per volume of parametrial involvement by disease as shown in [Table - 3]. The patients with parametrial volume involvement amounting to group 3 were taken into the bad prognostic factor group. On analysis, there was significant difference between these two groups in survival (univariate analysis: P = 0. 035). This significant difference was also seen by the log rank test ( P = 0.000) as shown in [Figure - 1]. Univariate analysis showed that the preimplant stage of the disease had a statistically significant effect on survival. Though a trend for better survival in those with stage II disease compared to those with stage III disease was seen [Figure - 2], it was not statistically significant when the log rank test was applied for analysis. It is to be expected that stage II disease will have better survival than stage III disease and this is confirmed by univariate analysis; the failure to demonstrate statistical significance by the log rank test could be due to the small sample size. Patients were divided into three groups [Table - 3] according to the volume of parametrial involvement and statistical analysis for survival was done by both univariate analysis and the log rank test. A significant difference in overall survival was found by the log rank test [Figure - 3] but the same was not seen by univariate analysis ( P = 0.06). Again, the statistical significance might not be evident by univariate analysis because of the small number of patients. There was no statistically significant difference in survival when patients were compared on the basis of the template doses received. The majority of the patients (13/22 patients; 59%) received a template dose of 25.80 Gy, delivered at 4.3 Gy per fraction for six fractions (twice daily for 3 days) and their survival was better than, or equal to, that of other dose groups, even those that received higher doses. However, only a small number of patients received a template dose other than 25.80 Gy (only two patients in each group receiving doses higher or lower than 25.80 Gy). We can conclude that a total template dose of 25.80 Gy, with a dose of 4.3 Gy per fraction prescribed at 100% isodose curve, is safe and effective [Figure - 4], but we cannot comment about the other doses because the number of patients receiving these doses is too small. Analysis according to time gap between first treatment and development of recurrence The time gap between first radiation treatment and recurrence ranged from 3 to 360 months, with the median time to recurrence being 10.25 months. On the basis of time to recurrence, patients were divided into two groups: those who had recurrence within 24 months (early relapse) and those who had recurrence after 24 months (late relapse). On comparison, there was no statistically significant difference in survival between the two groups. Univariate analysis was carried out for the other factors; these included age, hydronephrosis, upper and lower vaginal involvement, hemoglobin levels, creatinine levels, preimplant external radiation and brachytherapy doses, and prerecurrence stage. None of these factors had any statistically significant effect on survival. The overall survival for all patients is shown in [Figure - 5]. Multivariate analysis was done for prognostic variables like BPF and NBPF, parametrial volume, and stage of disease. As shown in [Table - 4], only BPF was found to have a statistically significant effect on survival ( P = 0.000). In our series, four patients had grade IV complications because of treatment. These four patients were free of disease locally when the complications were detected and these were therefore considered to be due to the treatment. One patient developed a vesicovaginal fistula (VVF), one developed a rectovaginal fistula, and one patient had soft tissue necrosis. Thus the grade IV complication rate turns out to be around 18%. One other patient had a VVF, but she also had local disease and the VVF was assumed to be due to the disease. Almost all treated patients had vaginal fibrosis; females who continued to have sexual intercourse had patent vaginas. Two patients had bleeding per rectum and one patient had bleeding per urethra; they were managed conservatively. One of these two patients had bleeding per rectum for more than a year and this was considered as a grade IV complication. Discussion For our study we selected only those patients of carcinoma cervix who had failed after some kind of radiation treatment and were being reirradiated with brachytherapy implant. A recurrent cancer after primary treatment with surgery or irradiation is a difficult management problem and evokes pessimism among surgeons and radiation oncologists. In this study, 5 out of the 22 patients (22.7%) are NED. Our study population had locally advanced, recurrent carcinoma cervix. The majority of our patients were not candidates for surgical exenteration because they had parametrial involvement up to, or close to, the lateral pelvic wall. A few patients were inoperable because of disease-related hydronephrosis of kidney(s), their nodal status, or their age. In our study, 14/22 patients (63.6%) had stage III disease and the rest (8/22 patients; 36.4%) stage II disease at recurrence [Table - 1]. These patients could be said to be having advanced local disease and proper selection of patients from among them, with treatment at an early stage of recurrence for low volume of disease, should improve results. For the analysis, we divided the patients into two groups: group 1 with BPF and group 2 with NBPF. The BPF group had 9 patients (41%); no patient in this group was NED, and median survival for this group was 6.9 months. In comparison, the NBPF group had 13 patients (59%); the median survival for this group was 29.6 months and 38.5% of these patients were NED. The difference in overall survival was statistically significant. Five patients in the BPF group had either hydronephrosis or pelvic nodes and all five failed. In retrospect, we think that these patients should not have been selected for treatment with implant brachytherapy. Statistical analysis was done with univariate analysis, but as only five patients were NED and the total number of patients was only 22, the results of statistical analysis may be erroneous. Multivariate analysis was done for various prognostic factors, of which only the BPF variable was found to have a statistically significant effect. Sommers et al . reported that about one-third of patients of cervical cancer will develop recurrent disease after initial therapy and, if left untreated, these patients have a 5-year survival of only 1%. [2] The chance of survival also depended on the site of the recurrence and the stage of disease at diagnosis. Survival was better for patients who failed more than 36 months after initial treatment. The 5-year survival for ten patients who underwent pelvic exenteration as curative management was 16%; patients failing only in the pelvis and who underwent reirradiation as a curative measure had a 40% (2/5) 5-year survival. The authors concluded that long-term survival could be achieved in a small percentage of selected patients who fail after definitive radiation. We reviewed the literature on recurrent cervical carcinoma. Puthawala et al . studied reirradiation with interstitial implant for recurrent pelvic malignancies (including cervical cancers); they found that 13 of 40 patients (33%) remained alive and disease free for the minimum follow-up period of 2 years; serious complications and soft tissue necrosis occurred in 15% of patients, but there was no mortality. [3] With regard to recurrent cancers of the uterine cervix, 50% (7/14) of patients were locally controlled; out of these seven patients, four (28.5%) were alive at the end of the study. All the three patients that died were locally controlled at the time of death. These investigators used exploratory laparotomy for local staging before selection of patients for implants. Gupta et al . used interstitial implant for treatment of locally advanced and recurrent gynecological malignancies. [4] They reported a 3-year actuarial local control rate of 49% (15/69) for patients who had received prior radiation treatment vs 63% (54/69) for those who had not. These investigators included all pelvic malignancies in their study and there were only six carcinoma cervix patients who were treated after radiation failure. Chapra et al . treated 78 patients of carcinoma cervix or endometrium with localized vault recurrence using an intravaginal template, either alone or in combination with external radiation. [5] There were 41 cervical and 37 endometrial cancers. Ninety-seven percent of these patients had undergone surgery as primary treatment and 37% (29/78 patients) had received radiation before developing vault recurrence. The authors reported an overall 5-year survival rate of 61% for patients who had not received prior irradiation and 47% for patients initially treated with radiation. The 5-year survival rate was 63% for tumors less than 4 cm in diameter and 37% when the tumor diameter was ≥ 4 cm ( P = 0.015). This shows that with proper selection of cases good results can be obtained in localized vault recurrence. In their series, 73% patients had tumor diameter less than 4 cm. Prempree et al . reported their results of treatment of late second malignancies or late recurrent squamous cell carcinoma of the uterine cervix after successful initial treatment. [6] They treated six patients by radiation; three patients (50%) survived with no evidence of disease for more than 5 years. The most important published surgical series was by Lawhead et al . from Memorial Sloan-Kettering Cancer Center on pelvic exenteration for recurrent or persistent gynecologic malignancies. [1] They reported 23% 5-year, 38% 3-year, and 48% 2-year survival. They treated 65 patients with pelvic exenteration for recurrent or persistent gynecological malignancies. In their series, the pelvic sidewall was involved in four patients and, of these, three died of the malignancy and one died in the postoperative period. Four patients were noted to have histologically positive pelvic nodes and all four died from persistent cancer. Eleven patients had histologically positive surgical margins and, among these, eight out of the nine patients available for follow-up died of the cancer. These investigators reported an operative mortality of 9.2%. It is interesting to note that in the surgical series by Lawhead et al ., all patients with nodal involvement or disease extending up to the lateral pelvic wall failed, [1] and that eight out of the nine patients with positive surgical margins (for whom follow-up is available) failed. Coleman et al . in their series studied 50 selected patients of carcinoma cervix who had postradiation persistent or recurrent disease. These patients had limited pelvic disease that was not fixed to the pelvic wall and without evidence of extrapelvic metastases. They concluded that these patients can be potentially salvaged by radical hysterectomy or pelvic exenteration. [7] The 5- and 10-year survival rates were 72% and 60%, respectively; there was one (2%), postoperative death. The 10-year survival rate was 80% in the 12 patients with tumor size less than 2 cm, compared with 48% in those with larger lesions. In our series, the patients with NBPF had a median survival of 29.6 months and five cases were NED (38.5%). No patient was NED in the BPF group (i.e., patients with hydronephrosis, nodal involvement, or group 3 parametrial involvement) failed. Chapra et al ., Puthawala , et al ., and other researchers have shown that with proper selection of patients (i.e., patients with low-volume recurrent disease) local control rates and survival rates were good. [3],[5] Puthawala et al . and Lawhead et al . were able to show good survival and local control in their respective series of treatment of recurrent gynecological cancers with implant or surgical exenteration because of their proper selection of patients. [1],[3] Ampuero et al . in their study of the use of interstitial template for locally advanced gynecological malignancies reported a low cure rate and a high incidence of complications with the use of interstitial brachytherapy in advanced gynecological malignancies. [8] Complications occurred in 12 out of 28 patients (42%), and 33% patients had survival ranging from 25 to 51 months. Chapra et al ., Gupta et al ., and Puthawala et al . all concluded that implant therapy was effective, with an acceptable complication rate. [3],[4],[5] Demanes et al . in their study of 62 patients of cervical carcinoma treated with HDR interstitial brachytherapy reported high pelvic control and low complication rates. [9] Grade 3-4 morbidity occurred in 6.5% of patients and one patient developed a fistula. No mortality was reported in any of the radiation series. In our series, grade 4 complications were noted in four (18%) patients; we think that this complication rate is acceptable for these cases, all of whom were patients of cervical carcinoma who had previously been treated with some form of radiation and were now being reirradiated. In our series also there was no mortality due to treatment. Complications were graded by objective criteria using the LENT SOMA scales for all anatomic sites. [10],[11] From our study and the review of literature on the salvage of recurrent cervical cancer patients we believe that the following points are very important, irrespective of whether surgery or radiation treatment is chosen to treat recurrent cervical cancer patients:
In the surgical series of Lawhead et al ., the operative mortality reported was 9.2%, but no mortality has been reported in any of the radiation series; in this respect, radiation treatment may have an advantage over surgical exenteration. [1] In patients with parametrial involvement extending up to the lateral pelvic wall, either external radiation boost can be given to the lateral parametrial tissues to increase cure rates or else these patients should not be selected for radiation or surgical salvage treatment. There is a need to conduct largest studies to come to reliable conclusions. In our institute we are now selecting only low-volume disease, i.e., bilateral parametrial involvement of group 1 or group 2 for salvage with implant; we do not select patients with nodal disease or hydronephrosis for this treatment. Conclusion We conclude that reirradiation with HDR brachytherapy implant can give a good chance of survival, with acceptable morbidity, if proper selection of patients is done. This treatment should not be done for palliative purposes. HDR brachytherapy implant has definite advantages in comparison with surgical exenteration. We feel that with proper selection of patients, reirradiation with HDR brachytherapy implant may give cure rates comparable with that of surgery-with colostomy-free survival in most patients and with reduced or no treatment-related mortality.References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09006f2.jpg] [cr09006t3.jpg] [cr09006f4.jpg] [cr09006f5.jpg] [cr09006t4.jpg] [cr09006f1.jpg] [cr09006t1.jpg] [cr09006t2.jpg] [cr09006f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}