 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
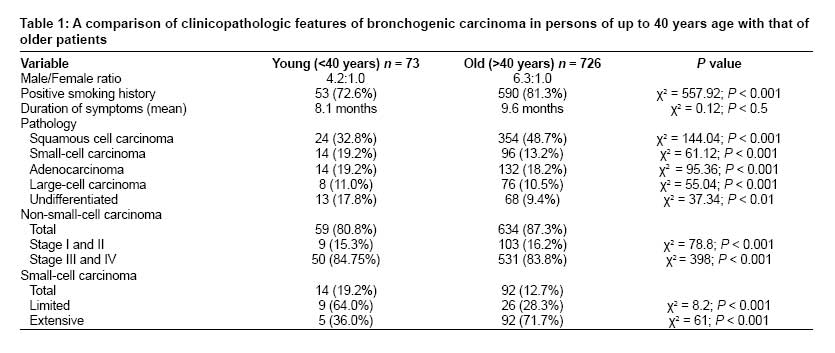
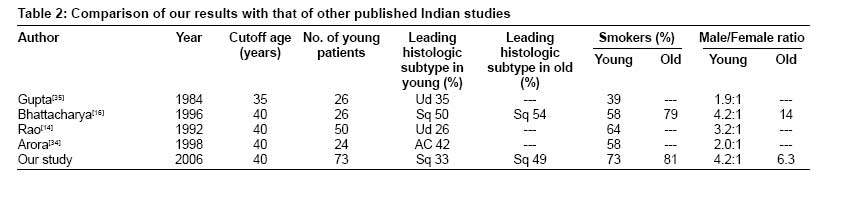
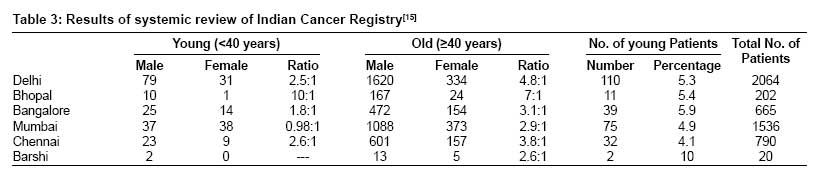
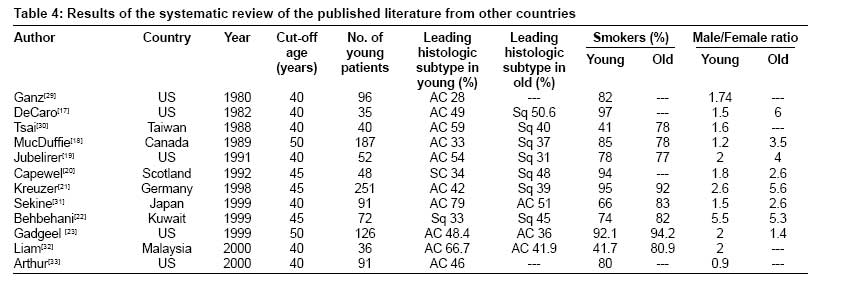
Journal of Cancer Research and Therapeutics, Vol. 5, No. 1, January-March, 2009, pp. 31-35 Original Article Comparison between young and old patients with bronchogenic carcinoma Prasad, R; Verma, SK & Sanjay Department of Pulmonary Medicine, King George's Medical University, Lucknow - 226 003, India. Code Number: cr09007 Abstract Objective: This study was undertaken to explore the clinicopathological profile of bronchogenic carcinoma in young patients.Materials and Methods: The present study was conducted on 799 consecutive histopathologically proven cases of bronchogenic carcinoma that were referred from different parts of Uttar Pradesh. Results: Out of 799 patients, 73 patients (9.1%; 59 males and 14 females) were ≤ 40 years of age and were classified as 'young' patients. The mean ages of the subjects in the younger and older patient groups were 36 and 58 years, respectively. Among the older patients, 590 (81.3%) were smokers, and there were 53 (72.6%) smokers among the younger patients. Squamous cell carcinoma was the commonest histological subtype in both the groups, but squamous cell carcinoma was more frequently diagnosed in older patients than in younger patients. Conclusion: This study suggests that, regardless of age or sex, lung cancer must be ruled out in all patients who have persistent signs of pulmonary disease and a history of heavy smoking. Keywords: Bronchogenic carcinoma, histopathology, smoking, young Introduction Bronchogenic carcinoma was considered to be a rare disease at the beginning of the 20 th century [1] but has now reached almost epidemic proportions. It is the leading cause of cancer deaths in developed countries and its incidence is rising at alarming rates in developing countries. [2] In India, bronchogenic carcinoma has been considered to be an infrequent disease [3] but an increased rate of diagnosis of bronchogenic carcinoma was recognized in the early 1960s. [4] Bronchogenic carcinoma is the commonest malignancy in men over 50 years of age and is uncommon before the age of 40 years. [5] However, there have been reports of an increase in the incidence of bronchogenic carcinoma in patients below 40 years of age. [6] This rise may be due to an increase in the smoking habit and also in exposure to other carcinogens. There are not many Indian studies on the pattern of bronchogenic carcinoma in patients below 40 years and the present study was planned to throw some light on this aspect. Materials and Methods The present study was conducted between July 1985 and December 2006 in the Department of Pulmonary Medicine, King George's Medical University, Lucknow, India, a tertiary level hospital and teaching center. This retrospective study enrolled 799 consecutive histopathologically proven cases of bronchogenic carcinoma referred to this institute from different parts of Uttar Pradesh. Seventy-three of the 799 patients were 40 years of age or younger. patients with metastatic cancer in the lungs, carcinoid tumor, lymphoma, and sarcoma of the lung were not included in the study. All patients were diagnosed on the basis of clinicoradiological findings and histopathological examination. Details of smoking were noted carefully with regard to type, amount smoked, and duration of the smoking habit. With regard to type of smoking, we identified four types: cigarette; bidi (tobacco wrapped in the leaf of the tendu tree and smoked like a cigarette); Chilam (a small clay pipe, in which tobacco is placed along with a piece of glowing charcoal; the Chilam is held in the cupped hands and the smoke is drawn through the opening in the lower end. Hucca (which is a system where a Chilam is attached to one end of a long wooden tube, the other end of which is immersed in water contained in a brass pot. The smoke is drawn through a flexible tube attached to the brass pot; the smoke, therefore, bubbles through the water before it is inhaled. For each patient we calculated the smoking index, which was the average number of bidis or cigarettes consumed per day multiplied by the duration of smoking in years. Socioeconomic status was recorded according to a modified Kuppuswamy scale. [7] Fiberoptic bronchoscopic findings were noted carefully with regard to side, site, and type of lesion. The histological typing was based on the accepted system for the clinical staging of lung cancer [8] and the revised international system for lung cancer staging. [9] Every attempt was made to categorize each tumor, but those tumors that could not be accurately classified were designated as 'unclassified.'Results Demographic characteristics [Table - 1] A total of 799 cases of lung cancer were diagnosed in our hospital from July 1985 to December 2006; 685 were males and 114 were females. Out of these 799 patients, 73 (9.1%; 59 males and 14 females) were ≤ 40 years of age. In this group of younger patients, 61 (83.6%) were 31-40 years of age, 10 (13.7%) were 21-30 years old, and 2 (2.7%) were ≤ 20 years of age. The youngest patient was 16 years old and the oldest was 40 at diagnosis. The mean ages of the subjects in the younger and older patient groups were 36 and 58 years, respectively. In 33 of the 73 patients (45.2%) in the younger group the diagnosis was made at the age 39 or 40 years. The ratio of men to women in this group was 4.2:1. Of the younger patients, 37 (50.7%) belonged to the lower-middle class and 16 patients (21.9%) to the upper-lower class according to the modified Kuppuswamy scale. Of the 73 patients, 55 (75.3%) were Hindu, 16 (21.9%) were Muslim, 1 (1.4%) was Sikh, and 1 (1.4%) was Christian. Fifty-six patients (76.7%) were from rural areas. Smoking and occupational history [Table - 1] Among the older patients, 590 (81.3%) were smokers, and 53 (72.6%) patients were smokers among the younger patients. Of the 53 smokers among the younger patients, 40 (75.5%) were bidi smokers, 11 (20.7%) were cigarette smokers, and 2 (3.8%) smoked the hucca and chilam. All of the female smokers (2) smoked bidis exclusively. Thirty-three (62.3%) patients had a smoking index of > 100, with the majority (31 patients; 94%) having smoked for more than 10 years. Occupational history was available for all patients. Three patients had possible occupational exposure to carcinogenic substances; one was a traffic policeman, one a microwelder, and one an automobile mechanic. History of exposure to household smoke was present in all female patients. Most of the other patients had nonindustrial jobs, and were farmers, housewives, or office workers. General features of patients The average duration of symptoms at the time of diagnosis was 8.1 months in the younger patients and 9.6 months in the older patients. In young patients, cough was the most common symptom (67 patients; 91.8%), followed by chest pain (53 patients; 72.6%), breathlessness (53 patients; 72.6%), fever (51 patients; 69.9%), anorexia (50 patients; 68.5%), expectoration (43 patients; 58.9%), hemoptysis (23 patients; 31.5%), hoarseness of the voice (14 patients; 19.2%), dysphagia (7 patients; 9.6%), and facial swelling (8 patients; 11%). Peripheral lymphadenopathy was noted in 31 (42.5%) of the young patients, anemia in 23 (31.5%), clubbing in 19 (26%), superior vena cava syndrome in 7 (9.6%), and Horner's syndrome in 2 (2.7%). In the older patients, hemoptysis was the most common complaint (595 patients; 81.9%) and was followed by breathlessness (454 patients; 62.5%), anorexia (451 patients; 62.1%), cough (407 patients; 56.1%), hoarseness of voice (52 patients; 7.2%), dysphagia (20 patients; 2.8%), and facial swelling (14 patients; 1.9%). Physical examination revealed peripheral lymphadenopathy in 497 patients (68.5%), anemia in 452 (62.3%), clubbing in 234 (32.2%), superior vena cava syndrome in 17 (2.3%), and Horner's syndrome in 14 (1.9%). One hundred and ninety-six (27%) of the older patients and 59 (80.8%) of the younger patients had been misdiagnosed as having pulmonary tuberculosis and had been prescribed antituberculous drugs before coming to our institute. Radiological pattern X-ray findings in the younger patients were as follows: 44 (60.3%) presented with a mass lesion, 32 (43.8%) with pleural effusion, 14 (19.2%) with collapse/consolidation, 9 (12.3%) with mediastinal widening, 1 (1.4%) with rib erosion, and 1 (1.4%) with cavitation in a lung. Of the older patients, 502 (69.1%) presented with a mass lesion, 352 (48.5%) with collapse/consolidation, 232 (32%) with pleural effusion, 102 (14.1%) with mediastinal widening, and 23 (3.2%) with rib erosion. Diagnostic procedures In younger patients, diagnosis of bronchogenic carcinoma was made by transthoracic fine needle aspiration cytology (FNAC) in 36 patients (49.3%), by fiberoptic bronchoscopy in 24 (32.9%), by pleural fluid cytology in 26 (35.6%), by FNAC of a lymph node in 24 (35.6%), by sputum cytology in 10 (13.7%), and by pleural biopsy in 3 (4.1%). In older patients, diagnosis of bronchogenic carcinoma was by transthoracic FNAC in 382 (52.6%) patients, by fiberoptic bronchoscopy in 258 (35.5%), by pleural fluid cytology in 152 (20.9%), by FNAC of a peripheral lymph node in 280 (38.6%), and by sputum cytology in 22 (3.0%). Histological typing [Table - 1] Squamous cell carcinoma was the commonest histologic subtype in both the groups, but squamous cell carcinoma was more frequently diagnosed in older patients than in the younger patients. In both the groups, the majority of those with non-small-cell carcinoma had advanced (stage III and IV) disease; however, the majority of those with small-cell carcinoma in the younger group (9/14 patients; 64%) had limited disease at the time of diagnosis though, in the older group, the majority of those with small-cell carcinoma (66/92 patients; 71.7%) had advanced disease. Discussion In the present study, 73 out of 799 patients (9.1%) with bronchogenic carcinoma seen at our tertiary care center were 40 years old or younger at diagnosis. Other Indian studies on bronchogenic carcinoma have also found a similar proportion of young (≤ 40 years) patients, the figures reported ranging from 9 to 14% [10],[11],[12],[13],[14] [Table - 2]. The proportion of young patients as per the Indian cancer registry ranges from 4.1 to 10% [15] [Table - 3]. One problem when comparing earlier studies on lung cancer with the Indian cancer registry is the variation in the definition of 'young.' In the present study, we took 40 years as the cutoff age, so as to ensure that there were an adequate number of younger patients. The ratio of male to female patients among the younger patients was 4.2: 1, which is lower than the 6.3: 1 male to female ratio seen among the older patients. This is in concordance with most previous studies [16],[17],[18],[19],[20],[21],[22],[23] [Table - 4]. These other studies were conducted in western populations and the higher proportion of females among younger patients may be explained partly by the fact that a high percentage of young women smoke in western countries. There is also evidence that women have an increased susceptibility to lung carcinogens. Zang and Wynder have shown that the relative risk for developing lung cancer was 1.5 times higher in women than in men, even after controlling for lifetime exposure to tobacco. [24] In our study, most of the female Among younger group (12/14 female patients; 85.7%) were nonsmokers; however, exposure to household smoke and the higher susceptibility of females, that was mentioned earlier, may be reasons for lung cancer among females in the younger age-groups. Smith, in a study conducted in four villages in western India, reported that the average daily exposure to benzo(a)pyrene during cooking was nearly 4000 ng/m 3 , which is equivalent to smoking approximately 20 packs of cigarettes per day. [25] A review of the Indian cancer registry [15] reveals that, for bronchogenic carcinoma, the ratio of male to female patients among the young in metropolitan cities like Delhi, Bangalore, Mumbai, and Chennai ranges from 0.98-2.6, whereas in Bhopal the ratio was 10 [Table - 3] which may be due to higher prevalence of smoking habits among female in metropolitan cities. The difference between our study and the Indian cancer registry may be due to differences in the studied population. The cause for early onset of bronchogenic carcinoma may be heavy smoking, environmental exposure to carcinogens and, perhaps, genetic predisposition. [26] In the present study, Among younger group (53/73 patients; 72.6%) were smokers, with the majority (40/53 patients; 75.5%) being bidi smokers. Notani and Sanghvi, in a retrospective study of 520 cases from Mumbai, reported that bidi smoking was an important contributing factor in the development of bronchogenic carcinoma in India. [27] Notani and Sanghavi [27] and Jussawalla and Jain [28] have reported a higher risk of lung cancer in bidi smokers compared with cigarette smokers. The risk of bronchogenic carcinoma also increases with increase in the smoking index. In the present study, 62.3% of patients had a smoking index > 100. The mean duration of symptoms in younger patients in our study was 10.2 months, whereas it was only 9.6 months in older patients. Twenty-seven percent of the older patients and 80.8% of the younger patients had been misdiagnosed and given treatment for tuberculosis. The lower degree of suspicion in younger patients probably accounts for this difference. All studies from America, Taiwan, Canada, Germany, Japan, and Malaysia [Table - 4] have reported that adenocarcinoma was the leading histological type in young patients. [17],[18],[19],[21],[23],[29],[30],[31],[32],[33],[34] A study from Scotland [20] showed that small-cell carcinoma was the predominant type, while a study from Kuwait [22] showed that squamous cell carcinoma was the predominant type in young patients. Bhattacharya [16] from India has reported squamous cell carcinoma as being the predominant histological type, and this is the case in the present study also. The high prevalence of smoking among males and household smoke exposure in females could be the cause of this finding in our study. However, other studies from India [Table - 2] have shown undifferentiated cell carcinoma to be the predominant type. [14],[35] In the present study, the majority (88.1%) of non-small-cell carcinoma patients had advanced stage disease (IIIb and IV) and 64% of small-cell carcinoma patients had limited disease at the time of diagnosis. One problem when comparing the stage of lung cancer in young patients in this study with that reported by prior studies on young lung cancer cases is that the earlier studies used the same system of staging for both small-cell and non-small-cell cancers. It is not clear why patients in the younger age-group have advanced disease when first seen. It is likely that because bronchogenic carcinoma is rare in the young, both the patient and the doctor may be late in suspecting that the symptoms could be due to this serious disease. Younger patients have better chances for successful resection and cure because they are not likely to have serious underlying medical problems that might preclude operation. This same factor, however, may contribute to delay in seeking medical attention and thus delay diagnosis until the disease is at a more advanced stage and no longer curable. Moreover, physicians often may not suspect an underlying carcinoma despite persistent pulmonary symptoms or abnormal findings on chest roentgenograms. Lack of diagnostic and treatment facilities at peripheral health centers could be another cause for delay in diagnosis of bronchogenic carcinoma. This study-and others-suggest that, regardless of age or sex, patients who have persistent signs of pulmonary disease and a history of heavy smoking must be considered at risk for lung cancer. Diagnostic tests should be performed early to exclude the possibility of lung cancer. If non-small-cell bronchogenic carcinoma is diagnosed and signs of distant metastasis are lacking, exploration should be done because improved survival depends on surgical resection. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09007t2.jpg] [cr09007t1.jpg] [cr09007t4.jpg] [cr09007t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}