 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
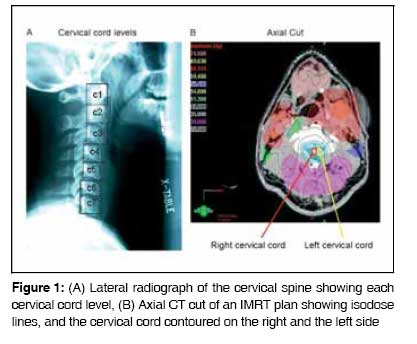
Journal of Cancer Research and Therapeutics, Vol. 5, No. 1, January-March, 2009, pp. 36-40 Brief Report Importance of contouring the cervical spine levels in initial intensity-modulated radiation therapy radiation for head and neck cancers: Implications for re-irradiation Parashar Bhupesh, Kuo Chi, Kutler David, Kuhel William, Sabbas Albert, Wernicke Gabriella, Nori Dattatreyudu Department of Radiation Oncology and Otolaryngology, Weill Cornell Medical Center, New York, NY 10021, USA. Code Number: cr09008 Abstract Aim: To evaluate the maximum differential cervical spinal (C-spine) cord dose in intensity-modulated radiation therapy (IMRT) plans of patients undergoing radiotherapy for treatment of head and neck cancer.Materials and Methods: The C-spine of ten head and neck cancer patients that were planned using IMRT and each cervical vertebral body and the right and left sides was contoured by splitting the cord in the center. Dose-volume histograms (DVH) and maximum point doses were obtained for each contour and compared. Results: The dose to the cord varied with the location of the primary tumor but such variation was not consistently seen. This report provides information that is critical for planning reirradiation treatments. We recommend that contouring of the C-spine cord with IMRT should include outlining of each cervical cord level and identification of the right and the left sides of the cord on each plan. Keywords: Cervical, contouring, cord, intensity-modulated radiation therapy, radiation Introduction Intensity-modulated radiation therapy (IMRT) is a widely-utilized new modality for delivering a highly conformal dose of radiation to patients with cancers of the head and neck. One advantage of treatment with IMRT is the sparing of the parotid and the normal mucosa. IMRT may also provide improved local control and reduction in late complications. [1] However, locoregional recurrence remains a problem in head and neck cancers, especially in locally advanced cases. [2] Treatment options for patients with a locally recurrent cancer include surgical resection (with or without postoperative radiation) and chemotherapy. [3] In locally recurrent but unresectable disease definitive radiation, with or without chemotherapy, can be offered. [4] In patients who have received a prior full course of radiation, chemotherapy was traditionally offered as the sole treatment option because of the risk of injury to such critical structures as the spinal cord and brainstem. [4] The response rate of recurrent head and neck tumors to chemotherapy alone is poor, with a median survival of only a few months. [5] However, with the advent of IMRT, a full course of reirradiation is possible because it allows highly conformal treatment; moreover, reirradiation with IMRT may render cure. [6] Conventional radiation treatment plans using three-dimensional (3D) or two-dimensional (2D) planning systems document the maximum radiation dose delivered to each critical organ. For example, the tolerance limit of the spinal cord is usually considered to be 45-50 Gray (Gy), [7] though there are data to suggest that the cord may tolerate higher doses. [8] In a non-IMRT plan (i.e., 2D or 3D plans), the C-spine gets a fairly uniform dose. However, only limited additional radiation can be added since the entire C-spine would have received, or is presumed to have received, the maximum permissible dose. This is not true for IMRT plans, where the dose distribution is not uniform and some areas of the cervical cord may receive a significantly higher dose than other sites. This dose disparity has significant implications for the treatment of patients who present with locally recurrent disease or a second primary in the head and neck area. In fact, the cord dose close to the site of recurrence may determine the total final reirradiation dose that can be delivered to these patients. In this study, we wanted to evaluate the differential C-spine cord dose with IMRT treatment to patients with head and neck cancer after contouring each cervical cord level (using cervical vertebrae), as well as dividing each level into right and left sides. Materials and Methods Ten patients who had previously received radiation to the head and neck area were included in the study. An IMRT plan and dose-volume histograms (DVH0 were generated for each patient. The dose prescriptions were given for each patient according to the volume and extent of disease. Four patients received a total dose of 70 Gy, in 2 Gy per fraction, to gross disease. Areas at high risk for microscopic disease received 60-63 Gy at 1.8 Gy per fraction and areas at lower risk of microscopic disease received 50-56 Gy at 1.8-1.6 Gy per fraction. One patient received an IMRT boost to his nasopharynx primary to a dose 20 Gy at 2 Gy per fraction. Three patients (two postoperative oral cavity primaries and one tonsillar primary) received ipsilateral neck radiation. The maximum permissible dose to any level of spinal cord was 50 Gy in nine of ten patients, whether treatment was for a primary tumor or for recurrent disease. One patient received definitive reirradiation (3 rd course of radiation) to the nasopharynx and the cumulative point dose (< 1% of volume) to a part of the cervical cord was ~51 Gy. Eight of the ten patients received chemotherapy concurrently with radiation. The C-spine of each patient was contoured by the same physician, with a separate contour generated for each cervical vertebral body [Figure - 1]. In addition, the right and left sides of each vertebral body were also specified by splitting the cord in the center. A DVH and maximum point dose were obtained for each contour. The patient characteristics are outlined in [Table - 1]. The study was done in after obtaining the institutional review board's approval and in accordance with its guidelines. Results For each of the ten patients, the radiation doses to all cervical cord levels, left and right side, were normalized to the maximum cord dose [Table - 2] and [Figure 2A-F],[Figure 2G-J]. In patients who received radiation to the primary site of disease as well as the neck, the doses to cervical cord levels ranged from 63 to 100% of maximum cord dose. In two patients, one of whom was planned for IMRT boost treatment only and the other for radiation to the primary site only (patient #4 and #5, respectively) [Table - 1], the dose range was significantly larger among between the cord levels (4-100%). The cord dose varied between vertebral bodies and was dependant on the location of the primary tumor as well as other high-risk areas. Cervical cord levels located in the vicinity of the high-dose area received a higher maximum dose compared to the cervical cord levels that were situated away from that region, though such variation was not consistently seen. For example, in patient #1 who had a left-sided primary tonsil cancer, the maximum dose was to the left cervical cord levels [Table - 2], patient 1, C1-C6. Overall, for all patients, the range of normalized cord doses to different sections of the cervical cord varied from 4 to 100%. Patients who were treated only to the primary site using IMRT plan (i.e., no radiation to the nodal areas) had most of the C-spine cord levels spared from the high radiation dose, except for the region that was in the immediate vicinity of the primary tumor [Table - 2], patient #4 and #5. Patients #9 and #10 had ipsilateral (right) neck radiation; however, the dose to the left side of cervical cord was not significantly lower than that to the right side, except for the lower cervical cord levels [Table - 2];[Figure 2 I and J]. Discussion As demonstrated in our study, different levels of the C-spine cord receive significantly different doses of radiation if IMRT techniques are employed. The normal output of a treatment planning system includes dose statistics (maximum, minimum, and mean dose) and the DVHs for various regions of interest. This information, although useful, does not convey the much needed spatial information as to the location of the hot spots in the C-spine cord. By separately outlining the various levels of the C-spine, we can more effectively assess the radiation doses along the cervical vertebrae and isolate the hot spots. This finding has important implications in patients who may require reirradiation for locally recurrent disease. If a patient develops recurrent disease in an area where the cord received less than 95% of the maximum tolerated cord dose then, in our experience, a highly conformal reirradiation plan can be generated that can provide definitive/curative high radiation doses. On the other hand, one should not make an assumption regarding the cord dose on the contralateral side of the cord for patients receiving ipsilateral radiation since the contralateral side may have also received a significant radiation dose with an IMRT plan. Since this information is critical in planning reirradiation treatments, we recommend that contouring of the cervical cord for any IMRT plan should include outlining of each cervical cord level and identification of the right and the left sides in each plan. For patients who have received primary IMRT for their head and neck malignancy in another institution, this information becomes even more relevant since it may be difficult to review dose distribution for each CT slice of primary treatment planning. We submit that introducing assessment of the maximum differential C-spine dose, using the contouring method of each cervical cord level and evaluating the right and the left sides separately, may make reirradiation safer and more effective. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09008t2.jpg] [cr09008t1.jpg] [cr09008f1.jpg] [cr09008f2G-J.jpg] [cr09008f2A-F.jpg] |
| |||||||||

{kind=link}
![[Table - 1]](/showimage?cr/photo/cr09008t1.jpg){kind=link}
![[Table - 2]](/showimage?cr/photo/cr09008t2.jpg){kind=link}
{kind=link}
{kind=link}