
|
Journal of Cancer Research and Therapeutics
Medknow Publications on behalf of the Association of Radiation Oncologists of India (AROI)
ISSN: 0973-1482 EISSN: 1998-4138
Vol. 5, Num. 2, 2009, pp. 71-77
|
Journal of Cancer Research and Therapeutics, Vol. 5, No. 2, April-June, 2009, pp. 71-77
Review Article
Role of human papilloma virus in the oral carcinogenesis: An Indian perspective
Chocolatewala Noureen M, Chaturvedi Pankaj
Department of Head and Neck, Tata Memorial Hospital, Mumbai
Correspondence Address:Tata Memorial Hospital, Head & Neck Unit, Dr. E Borges Road, Parel, Mumbai - 400 012
chaturvedi.pankaj@gmail.com
Code Number: cr09022
DOI: 10.4103/0973-1482.52788
Abstract Oral squamous cell carcinoma (OSCC) is one of the most common cancers in the Indian subcontinent. Although tobacco and alcohol are the main etiologic factors for nearly three-fourth of these cancers, no definite etiologic factor can be identified in one-fourth of the cases. There is growing evidence that human papilloma virus (HPV) may act as a cocarcinogen, along with tobacco, in the causation of oral cancers. The role of HPV in the etiology of anogenital cancers has been firmly established, and infection with this virus has also been shown to have prognostic significance. However, there is no clear evidence to support its involvement in oral carcinogenesis.
We searched the PubMed database for all literature published from 1985 to 2008 and performed a systemic review in order to understand the relationship of HPV with oral cancers and its prevalence in various sub-sites in the oral cavity.
Association of HPV is strongest for oropharyngeal cancers, especially cancers of the tonsils, followed by those of the base of tongue. High-risk HPV-16 is the predominant type; it commonly affects the younger age-groups, with males appearing to have a predisposition for infection with this strain. Its prevalence increases from normal to dysplasia and finally to cancer. HPV prevalence has been reported to be twice as high in premalignant lesions as in normal mucosa and is nearly five times higher in OSCC. The overall prevalence of HPV in OSCC ranges between 20-50%. OSCCs associated with HPV have been found to have better outcomes, being more responsive to radiotherapy and showing higher survival rates.
In view of the association of HPV with OSCC, it should be worthwhile to conduct further experimental studies to elucidate its role in oral carcinogenesis.
Keywords: Human papilloma virus, oral cancer, oral cavity
Introduction
Head and neck squamous cell carcinomas (HNSCC) are a biologically heterogeneous group of cancers. They are a major cause of cancer morbidity and mortality worldwide, especially so in the Indian subcontinent. Head and neck cancers, 90% of which are squamous cell carcinomas (SCC), ranks sixth among all malignancies worldwide. [1],[2] In the Indian subcontinent, oral squamous cell carcinoma (OSCC) is the most common malignancy, accounting up to 40-50% of all malignant cancers. [3] Despite advances in treatment, there has been no significant decline in the mortality rate.
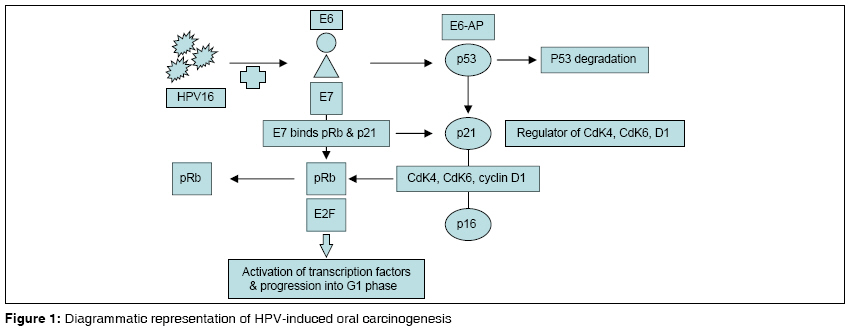
The most frequently detected genetic alteration in cancers of the oral cavity is the loss of tumor suppressor protein such as p53, antiproliferative proteins, and the product of the retinoblastoma gene (pRb). This is a result of either genetic mutation or interaction with viral oncoproteins like human papilloma virus (HPV) E6/E7. [4],[5] Any disruption in their activity permits the accumulation of genetic mutations, leading to a carcinogenic phenotype [Figure - 1]. Other viruses/proteins that can bind to the p53 protein and inactivate its function in the regulation of cell proliferation are the SV40 T antigen and the adenovirus E1B protein.
Globally, the main risk factors for oral cancer are tobacco and alcohol. Exposure to one or both of these factors accounts for more than 75% of oral cancers in developed countries. [6] The combined effect is multiplicative rather than additive. [7],[8],[9] Diets lacking in essential micronutrients, exposure to agents such as radiation, poor oral hygiene, genetic susceptibility of the individual, and certain viruses have also been associated with an increased risk of cancer. [10],[11],[12],[13],[14] However, approximately 20% of oral cancers occur in people lacking these established risk factors, [15],[16],[17] and there is strong epidemiologic and experimental evidence indicating that HPV may account for the majority of these cancers. [18],[19],[20] The role of HPV as an etiologic agent in cancer was first recognized in the uterine cervix and is now well established. It has been estimated that HPV infections account for 6% of cancers worldwide. Most HPV-related cancers are anogenital cancers. [21]
Pathogenesis
HPVs are small (55 nm), nonenveloped, icosahedral, epitheliotropic DNA tumor viruses that are acquired early in life. [22],[23],[24],[25] More than 118 HPVs have been completely described. [26] The role of HPV in the development of anogenital cancers has been widely studied. Approximately 50 different types of HPV can infect surfaces in the anogenital region. [27] Many of these types have also been identified in mucosal lesions of the oral cavity, including precancerous lesions and cancer-derived cell lines, as well as in lymph node metastases.
HPVs can be categorized into two major groups based on the oncogenic potential. HPV-6 and -11 are the two most common low-risk types; they account for the majority of genital warts, which rarely progress to malignancy. HPV-16 and -18 are the major high-risk types and predominate in invasive anogenital cancers. [5],[28] As in genital lesions, HPV-16 is the most common type and is associated with a wide range of oral lesions, from benign to premalignant and malignant. [29]
HPVs have been a prime suspect in the etiology of OSCC due to their morphological association with squamous cell carcinomas and their ability to immortalize oral keratinocytes and bring about transformation of epithelial cells. [30] The buccal mucosa, being the site that is most exposed to chemical carcinogens, infections, and trauma, is most vulnerable to carcinogenesis. It has been postulated that abrasions caused due to this continuous exposure might make this mucosal surface more susceptible to HPV by making it easier for the virus to gain entry into the basal cells. [31],[32],[33]
The proposed mechanism of action of HPV in tumorigenesis includes the following [Figure - 1]:
- A breakpoint in the E1/ E2 sequence allows integration of HPV into the host genome and significantly increases its tumorigenicity through upregulation of E6 and E7 encoded in the early open reading frame of the virus.
- Expression of E6 and E7 is negatively regulated by E2 protein, which is also encoded in the early open reading frame of the virus.
- By altering host genome functions, HPV E6 and E7 disrupts the p53 and pRb tumor suppressor genes, as well as numerous cellular proteins involved in carcinogenesis. [4]
- Subsequently, infected cells develop defects in gene expression controlling apoptosis, DNA repair, and cell cycle, thus paving the way for cellular transformation.
Materials and Methods It is unknown whether the physical state of the virus influences tumor biology. Application of a real-time PCR technique in the determination of the physical status of HPV-16 in OSCC samples found that patients who harbored episomal HPV-16 DNA more often had large tumors than did those whose samples contained integrated or mixed forms. [34] They observed no correlation between the physical status of HPV-16 DNA and prognosis in a series of 12 HNSCC patients. [35] Seroreactivity against the viral capsid proteins and oncogenes has been consistently associated with an increased risk of head and neck cancer.
Review of Literature
HPV, a known tumor virus, has been identified as the causative agent in 99.7% of cervical cancers. [36] In recent years, there has been mounting evidence of the role of HPV as the etiologic agent in a subset of head and neck cancers. [37] We searched the PubMed database for literature published from January 1985 through August 2008 reporting any relationship between HPV and normal oral mucosa, leukoplakia, intraepithelial neoplasia (i.e., dysplasia and carcinoma in situ ), verrucous carcinoma, and OSCC. We also searched for reports on the site-wise prevalence of the virus within oral cavity. We performed a systematic review of the available literature to test the hypothesis that HPV infection is a risk factor for OSCC, while addressing its relationship to various oral sites.
An association between HPV and head and neck cancer was first noticed during the 1960s, when there were reports of conversion of recalcitrant laryngeal papillomas to malignancy after radiation therapy. [38],[39] A possible role for HPV in the etiology of cancers at other sites within the head and neck was first suggested by Lüning et al. in 1985. [40]
There is increasing evidence of the role of HPV in the development of OSCC. Although the role is less clear in OSCC than in cervical cancer, HPV DNA has been identified in primary tumors of the tonsil, larynx, hypopharynx, oral cavity, tongue, and nasopharynx, as well as in celllines derived from a variety of head and neck carcinomas and in inverted papillomas that have progressed to SCC. Precancerous lesions and metastatic lymph nodes have also been shown to contain DNA of the same HPV type as in the primary tumor in 76% of the cases, supporting the involvement of HPV in the development of SCC. [41],[42],[43],[44],[45],[46],[47]
The prevalence of HPV in OSCC, which was initially underestimated to be between 20-30%, [48] is now considered to be as high as 50% if not more; in other words, it is likely that every alternate OSCC patient is HPV positive. [49],[50],[51],[52],[53],[54] The association is strongest in the oropharynx, most notably in the tonsil [55],[56],[57],[58],[59] and base of tongue, which present more frequent basaloid morphology and less frequent p53 mutations.
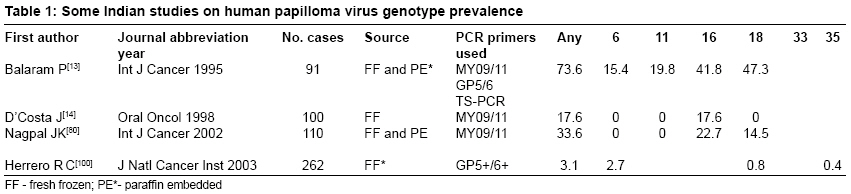
HPV Genotypes Of the HPV family, more than 12 types have been found in oral lesions, including HPVs 1, 2, 4, 6, 7, 11, 13, 16, 18, 30, 32, and 57. [30] HPV-13 and -32 appears to be restricted to oral lesions. Although we found heterogeneity among the various studies [Table - 1], HPV-16 and -18 were detected in 80% of cases, revealing that high-risk HPV viruses were detected 2.8 times more often than the low-risk types in oral carcinomas; the latter appeared to be more often associated with premalignant lesions.
Age / Gender Mucosal cancer occurring in the younger age-groups-with little or no exposure to known risk factors-is increasing in incidence and has long been thought to constitute an etiologically distinct group. [60],[61] The disease may be mutilating and fatal and therefore has tremendous social implications, especially in the young. Controversy exists concerning the prognosis and treatment of these young patients. Although the picture is still not very clear, some studies have documented that high-risk HPV types are three times more likely to be detected in OSCC in young patients than in patients above 60 years of age; [62],[63] this is due to viral transmission by direct physical contact. Tumor site may also vary by age, with a higher frequency of tongue or oral cavity tumors in the younger age-groups. A higher risk of oral cancer has been found to be associated with number of sexual partners, younger age at first sexual intercourse, practice of oral sex, and history of genital warts. [64],[65],[66] However, further investigations are needed to clarify these findings.
Site There has been wide variation in HPV positivity rates in cancers at different sites in the head and neck region. Approximately 25-75% [67] of oropharyngeal cancers have tested HPV positive, with rates in tonsillar cancer being the highest, followed by cancers of the tongue and of the buccal mucosa. In one study, 74% of SCCs removed from the lateral aspect of the tongue were found positive for oncogenic subtypes of HPV, while other authors have reported 72.5-91% prevalence of HPV in tongue cancers. [68],[69],[70] These results suggest that oncogenic HPV should be considered as a risk factor for tongue cancer.
HPV in Oral Premalignant Lesions
The likelihood of detecting HPV increases from normal mucosa to premalignant lesions to oral cancer; HPV is 2-3 times more likely to be detected in precancerous oral mucosa and 4.7 times more likely to be detected in OSCC than in normal mucosa. [70]
A review of 16 studies on leukoplakia revealed that HPV was prevalent in 14.8% of the cases, with the mean age of the patients being 40.7 years. Buccal mucosa, tongue, and palate were the sites commonly harboring these viruses. [71],[72]
In verrucous carcinoma HPV showed a mean prevalence of 27%, demonstrating that the virus has a greater predisposition for buccal mucosa, alveolus, and palate. The commonest genotype was HPV 6/11, being seen in 47% of cases. [69]
Association as Cocarcinogen Certain studies show HPV infection to be associated with an increased risk (up to three times) of OSCC, independent of exposure to alcohol or tobacco, [37],[54] demonstrating that the relative risk of OSCC with HPV infection is equal to or exceeds the risk associated with tobacco and alcohol consumption. Thus, as has been discussed elsewhere, four risk factors have been found to be significantly associated with an increase in HPV detection, i.e., male gender, oropharyngeal tumors, less tobacco usage, and history of oro-genital sex. [59],[73],[74]
Prognosis
Reports on the impact of HPV positivity on prognosis in HNSCC have not been consistent. Pintos and coworkers [75] reported that HPV infection is unlikely to play any role in the prognosis of patients with cancers of the upper aerodigestive tract. Ringstrφm and coworkers, [74] however, observed that HNSCC patients who had HPV-positive tumors had better overall and disease-specific survival than HPV-negative patients.
Several studies have reported that detection of HPV DNA is highly associated with poorly differentiated cancer grade, positive lymph nodes, and late-stage disease. [58],[62],[76] Despite this, improved survival among HPV-positive head and neck cancers has been noted by others. [77] This may suggest that the effects of HPV on the p53 and Rb proteins are not as detrimental as the more classic mutations induced by other known carcinogens, such as tobacco and alcohol. It is possible, for example, that p53 inactivation may depend on the level of HPV E6 present, and that some p53 may ′escape′ inactivation. These residual functional p53 may mediate cellular apoptosis following radiotherapy. Although this is still controversial, the role of p53 in HPV-induced OSCC has been linked with better radiosensitivity of tumor. [78],[79] Some studies also support factors such as genetic predisposition being responsible for the high rate of oral cancers. P53 codon 72 genotype frequencies in Indian oral cancer patients were 0.55(Arg) and 0.45(Pro) in 37/110 patients, suggesting that Arg/Arg genotypes are more susceptible to HPV infection and oral carcinogenesis. [80]
Cell Markers of HPV Infection
HPV DNA has been detected in the full spectrum of disease, including in precancerous lesions, cancer-derived cell lines, and lymph node metastases. HPV viral load-a measure of the amount of viral DNA in the biopsy specimen-alone or in conjunction with well-characterized HPV serological assays, may also clarify the role of HPV in oral carcinoma. Antibodies against HPV E6 and E7 are strong markers of invasive HPV-associated malignancy, [81],[82] unlike antibodies against HPV DNA virus-like particles, which are considered a marker of cumulative, lifetime HPV infection and are associated with HPV-related diseases. [83],[84] These seromarkers were relatively higher among cases having high viral load as compared to those having low viral load.
Survivin expression, an index of apoptosis blockage, is higher in HPV-negative cases than in HPV-positive ones and is also more pronounced in solid tumors. [85],[86] It has been documented that increased survivin is associated with poor prognosis and reduced survival. [87] Thus, HPV-positive oral cancers show relatively good clinical and biomolecular behavior, no recurrence, 5% mortality, and better response to radiotherapy.
HPV Prevalence in Indian Oral Cancers Not much data is available regarding the incidence of HPV-induced oral cancers in the Indian scenario. Whereas the tongue and the floor of the mouth are the common sites for the development of SCC in Western countries, [12] the buccal mucosa is the most common site for SCC in India; this is chiefly attributable to the common habit of placing a tobacco and betel quid in the gingival sulcus. Studies on patients with tobacco-induced OSCC have produced some interesting findings; for example, 33.6% of OSCC patients were HPV positive in Eastern India as compared with 67% in South India and 15% in Western India. [13],[14] HPV infection is more prominent in OSCC cases from India than in patients from other countries; for example, only 23% of Japanese patients, 8-20% of American patients, and 19% of Dutch patients are HPV positive. Apparently, HPV plays a very important role in the development of oral cancers in the Indian population. Among oropharyngeal SCCs that are positive for HPV DNA, 90% show the presence of HPV-16. In a study of 110 patients from Eastern India with tobacco-induced OSCC, out of 37 patients who were HPV positive, HPV-16 was the most frequently involved type (22.7%), followed by HPV-18 (14.5%) and HPV-16/18 coinfection (10%). [80] These findings are in agreement with that of other groups except that of Balaram et al ., [13] whose study was based on a South Indian population.
Future Directions
Although several studies have supported the presence of an association between HPV infection and oral cancers, the significance of HPV in the prognosis of oral cancers has not been firmly established. The reason for this underlying therapeutic benefit may be treatment related. It is interesting to note that overall survival was significantly higher in these HPV-HR compared to HPV-negative cases. [77],[78],[79],[80],[81],[82],[83],[84],[85],[86],[87],[88] Future clinical management and treatment decisions may need to take into consideration differences in the extent of disease associated with HPV infection and perhaps recognize virus-related tumors as a separate disease entity.
Understanding the role of HPV in the etiology of oral cancer may be essential in determining prognosis and treatment and for disease prevention. Over the past few years, there have been significant advances in the understanding of the tumor pattern, and various options are now available as far as treatment modalities and techniques of surgical reconstruction are concerned. However, there has been no significant improvement in the 5-year survival of these patients, which continues to be around 40%. Thus, additional information regarding the pathogenesis of these tumors is necessary that would aid us in providing better prognosis for these patients. Various cellular proteins, such as p53, cyclin D1, and p27, have been identified as prognostic markers [89],[90] but none have gained universal acceptance. However, the use of immunohistochemistry, with screening of oral cancers for HPV-16 by PCR for p16 expression as a marker of HPV E7 oncogene activity, has now been extensively studied and should soon find universal acceptance as a method for identifying the etiology of these cancers; this will also have prognostic implications.
The identification of HPV-16 and -18 as the major types causing cervical cancers, and HPV-6 and -11 as causing the majority of genital warts, have resulted in the development of prophylactic vaccines based on their viral capsids; these vaccines have shown beneficial results in clinical trials [91],[92],[93],[94],[95],[96],[97],[98],[99],[100] and should soon become available in the market. This is encouraging and gives us hope that it should be possible to develop such vaccines against head and neck cancers too; it would be especially useful in advanced cases, where its therapeutic benefit when given along with other treatment modalities would result in a better prognosis for the patient.
Conclusions
There has been a rising international recognition of the role of HPV as an etiologic agent in a subset of oral cancers. The HPV detection rate of 20-50% in oral carcinomas is among the highest of any extragenital human malignancy. Given this high rate of positivity, HPV may be recognized as a tumorigenic factor for the development of head and neck cancers.
HPV association has been linked with better overall survival of these patients. It therefore becomes essential to consider cytological screening of patients who may harbor latent high-risk HPV in their oral mucosa. This knowledge would be helpful in certain situations; for example, the detection of HPV in a patient with dysplastic oral will be of great help in guiding decision making. Also, treatment modalities are different for HPV-associated OSCCs vs non-HPV-associated OSCCs.
References
| 1. | Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world cancer burden: Globocan 2000. Int J Cancer 2001;94:153-6. Back to cited text no. 1 |
| 2. | Parkin DM, Pisani P, Ferlay J. Global cancer statistics. CA Cancer J Clin 1999;49:33-6. Back to cited text no. 2 |
| 3. | Ferlay J, Bray F, Pisani P, Parkin DM. Globocan 2000-cancer incidence, mortality and prevalence worldwide, version 1.0. IARC Cancer Base No. 5. Lyon: IARC; 2001. Back to cited text no. 3 |
| 4. | Parker MF, Arroyo GF, Geradts J. Molecular characterization of adenocarcinoma of the cervix. Gynecol Oncol 1997;64:242-51. Back to cited text no. 4 |
| 5. | Das BC, Gopalkrishna V, Hedau S, Katiyar S. Cancer of the uterine cervix and human papillomavirus infection. Curr Sci 2000;78:52-63. Back to cited text no. 5 |
| 6. | Dobrossy L. Epidemiology of head and neck cancer: Magnitude of the problem. Cancer Metastasis Rev 2005;24:9-17. Back to cited text no. 6 |
| 7. | Blot WJ, McLaughlin JK, Winn DM, Austin DF, Greenberg RS, Preston-Martin S, et al . Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res 1988;48:3282-7. Back to cited text no. 7 |
| 8. | Smith EM, Hoffman HT, Summersgill KS, Kirchner HL, Turek LP, Haugen TH. Human papillomavirus and risk of oral cancer. Laryngoscope 1998;108:1098-103. Back to cited text no. 8 |
| 9. | Day GL, Blot WJ, Austin DF, Bernstein L, Greenberg RS, Preston-Martin S, et al . Racial differences in risk of oral and pharyngeal cancer: Alcohol, tobacco, and other determinants. J Natl Cancer Inst 1993;85:465-73. Back to cited text no. 9 |
| 10. | Portugal LG, Goldenberg JD, Wenig BL, Ferrer KT, Nodzenski E, Sabnani JB, et al . Human papillomavirus expression and p53 gene mutations in squamous cell carcinoma. Arch Otolaryngol Head Neck Surg 1997;123:1230-4. Back to cited text no. 10 |
| 11. | Shindoh M, Chiba I, Yasuda M, Saito T, Funaoka K, Kohgo T, et al . Detection of HPV DNA sequences in oral squamous cell carcinomas and their relation to p53 and proliferating cell nuclear antigen expression. Cancer 1995;76:1513-21. Back to cited text no. 11 |
| 12. | Paz IB, Cook N, Odom-Maryon T, Xie Y, Wilczynski SP. Human papillomavirus (HPV) in head and neck cancer: An association of HPV-16 with squamous cell carcinoma of Waldeyer's tonsillar ring. Cancer 1997;9:595-604. Back to cited text no. 12 |
| 13. | Balaram P, Nalinakumari KR, Abraham E, Balan A, Hareendran NK, Bernard HU, et al . Human papilloma virus in 91 oral Indian betel quid chewers: High prevelance and multiplicity of infections. Int J Cancer 1995;61:450-4. Back to cited text no. 13 |
| 14. | D'Costa J, Saranath D, Dedhia P, Sanghvi V, Mehta AR. Detection of HPV-16 genome in human oral cancers and potentially malignant lesions from India. Oral Oncol 1998;34:413-20. Back to cited text no. 14 |
| 15. | Wiseman SM, Swede H, Stoler DL, Anderson GR, Rigual NR, Hicks WL Jr, et al . Squamous cell carcinoma of the head and neck in nonsmokers and nondrinkers: An analysis of clinicopathologic characteristics and treatment outcomes. Ann Surg Oncol 2003;10:551-7. Back to cited text no. 15 |
| 16. | Lingen M, Sturgis EM, Kies MS. Squamous cell carcinoma of the head and neck in nonsmokers: Clinical and biologic characteristics and implications for management. Curr Opin Oncol 2001;13:176-82. Back to cited text no. 16 |
| 17. | Yamaguchi T, Shindoh M, Amemiya A, Notani K, Fukuda H, Sakaoka H, et al . Identification of human papillomavirus DNA sequence in the hyperplastic epitheliumof an oral denture fibroma. Dis Markers 1997;13:135-40. Back to cited text no. 17 |
| 18. | Klussmann JP, Gültekin E, Weissenborn SJ, Wieland U, Dries V, Dienes HP, et al . Expression of p16 protein identifies a distinct entity of tonsillar carcinomas associated with human papillomavirus. Am J Pathol 2003;162:747-53. Back to cited text no. 18 |
| 19. | Venuti A, Badaracco G, Rizzo C, Mafera B, Rahimi S, Vigili M. Presence of HPV in head and neck tumours: High prevalence in tonsillar localization. J Exp Clin Cancer Res 2004;23:561-6. Back to cited text no. 19 |
| 20. | Li W, Thompson CH, Cossart YE, O'Brien CJ, McNeil EB, Scolyer RA, et al . The expression of key cell cycle markers and presence of human papillomavirus in squamous cell carcinoma of the tonsil. Head Neck 2004;26:1-9. Back to cited text no. 20 |
| 21. | Shanta V, Krishnamurthi S, Gajalakshmi CK, Swaminathan R, Ravichandran K. Epidemiology of cancer of the cervix: Global and national perspective. J Indian Med Assoc 2000;98:49-52. Back to cited text no. 21 |
| 22. | Scully C, Cox MF, Prime SS, Maitland NJ. Papillomaviruses: The current status in relation to oral disease. Oral Surg Oral Med Oral Pathol 1988;65:526-32. Back to cited text no. 22 |
| 23. | Sedlacek TV, Lindheim S, Eder C. Mechanisms for human papillomavirus transmission at birth. Am J Obstet Gynecol 1989;161:55-9. Back to cited text no. 23 |
| 24. | Tseng CJ, Lin CY, Wang RL, Chen LJ, Chang YL, Hsieh TT, et al . Possible transplacental transmission of human papillomavirus. Am J Obstet Gynecol 1992;166:35-40. Back to cited text no. 24 |
| 25. | Moscicki AB, Palefsky J, Gonzales J, Schoolnik GK. Human papillomavirus infection in sexually active adolescent females: Prevalence and risk factors. Pediatr Res 1990;28:507-13. Back to cited text no. 25 |
| 26. | de Villiers EM, Fauquet C, Broker TR, Bernard HU, zur Hausen H. Classification of papillomaviruses. Virology 2004;324:17-27. Back to cited text no. 26 |
| 27. | Motoyama S, Ladines-Llave CA, Luis Villanueva S, Maruo T. The role of human papillomavirus in the molecular biology of cervical carcinogenesis. Kobe J Med Sci 2004;50:9-19. Back to cited text no. 27 |
| 28. | Zur Hausen H. Viruses in human cancer. Science 1991;254:1167-73. Back to cited text no. 28 |
| 29. | Syrjanen SM, Syrjanen KJ, Happonen RP. Human papillomavirus (HPV) DNA sequences in oral precancerous lesions and squamous cell carcinoma demonstrated by in situ hybridization. J Oral Pathol 1988;17:273-8. Back to cited text no. 29 |
| 30. | Chang F, Syrjanen S, Kellokoski J, Syrjanen K. Human papillomavirus (HPV) infections and their associations with oral disease. J Oral Pathol Med 1991;20:305-17. Back to cited text no. 30 |
| 31. | Jeon S, Allen-Hoffmann BL, Lambert PF. Integration of human papillomavirus type 16 into the human genome correlates with a selective growth advantage of cells. J Virol 1995;69:2989-97. Back to cited text no. 31 |
| 32. | Syrjanen SM, Syrjanen KJ, Happonen RP. Human papillomavirus (HPV) DNA sequences in oral precancerous lesions and squamous cell carcinoma demonstrated by in situ hybridization. J Oral Pathol 1988;17:273-8. Back to cited text no. 32 |
| 33. | Tsuchiya H, Tomita Y, Shirasawa H, Tanzawa H, Sato K, Simizu B. Detection of human papillomavirus in head and neck tumors with DNA hybridization and immunohistochemical analysis. Oral Surg Oral Med Oral Pathol 1991;71:721-5. Back to cited text no. 33 |
| 34. | Koskinen WJ, Chen RW, Leivo I, Mδkitie A, Bδck L, Kontio R, et al . Prevalence and physical status of HPV in SCC of head and neck. Int J Cancer 2003;107:401-6. Back to cited text no. 34 |
| 35. | Badaracco G, Venuti A, Morello R, Muller A, Marcante ML. Human papillomavirus in head and neck carcinomas: Prevalence, physical status and relationship with clinical/pathological parameters. Anticancer Res 2000;20:1301-5. Back to cited text no. 35 |
| 36. | Ostrow RS, Manias DA, Fong WJ, Zachow KR, Faras AJ. A survey of human cancers for human papillomavirus DNA by filter hybridization. Cancer 1987;59:429-34. Back to cited text no. 36 |
| 37. | Brandsma JL, Abramson AL. Association of papillomavirus with cancers of the head and neck. Arch Otolaryngol Head Neck Surg 1989;115:621-5. Back to cited text no. 37 |
| 38. | Dekelboum AM. papillomas of the larynx. Arch Otolaryngol 1965;81:390-7. Back to cited text no. 38 |
| 39. | Rabbett WF. Juvenile laryngeal papillomatosis: The relation of irradiation to malignant degeneration in this disease. Ann Otol Rhinol Laryngol 1965;74:1149-63. Back to cited text no. 39 |
| 40. | Lφning T, Ikenberg H, Becker J, Gissmann L, Hoepfer I, zur Hausen H. Analysis of oral papillomas, leukoplakias, and invasive carcinomas for human papillomavirus type related DNA. J Invest Dermatol 1985;84:417-20. Back to cited text no. 40 |
| 41. | Shroyer KR, Greer RO, Fankhouser CA, McGuirt WF, Marshall R. Detection of human papillomavirus DNA in oral verrucous carcinoma by polymerase chain reaction. Mod Pathol 1993;6:669-72. Back to cited text no. 41 |
| 42. | Dekmezian RH, Batsakis JG, Goepfert H. In situ hybridization of papillomavirus DNA in head and neck squamous cell carcinomas. Arch Otolaryngol Head Neck Surg 1987;113:819-21. Back to cited text no. 42 |
| 43. | Howell RE, Gallant L. Human papillomavirus type 16 in an oral squamous carcinoma and its metastasis. Oral Surg Oral Med Oral Pathol 1992;74:620-6. Back to cited text no. 43 |
| 44. | Woods KV, Shillitoe EJ, Spitz MR, Schantz SP, Adler-Storthz K. Analysis of human papillomavirus DNA in oral squamous cell carcinomas. J Oral Pathol Med 1993;22:101-8. Back to cited text no. 44 |
| 45. | Fouret P, Monceaux G, Temam S, Lacourreye L, St Guily JL. Human papillomavirus in head and neck squamous cell carcinomas in nonsmokers. Arch Otolaryngol Head Neck Surg 1997;123:513-6. Back to cited text no. 45 |
| 46. | Bradford CR, Zacks SE, Androphy EJ, Gregoire L, Lancaster WD, Carey TE. Human papillomavirus DNA sequences in cell lines derived from head and neck squamous cell carcinomas. Otolaryngol Head Neck Surg 1991;104:303-10. Back to cited text no. 46 |
| 47. | Ishibashi T, Matsushima S, Tsunokawa Y, Asai M, Nomura Y, Sugimura T, et al . Human papillomavirus DNA in squamous cell carcinoma of the upper aerodigestive tract. Arch Otolaryngol Head Neck Surg 1990;116:294-8. Back to cited text no. 47 |
| 48. | Miller CS, White DK. Human papillomavirus expression in oral mucosa, premalignant conditions, and squamous cell carcinoma: A retrospective review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:57-68. Back to cited text no. 48 |
| 49. | Sugerman PB, Shillitoe EJ. The high risk human papillo maviruses and oral cancer: Evidence for and against a causal relationship. Oral Dis 1997;3:130-47. Back to cited text no. 49 |
| 50. | Chang KW, Chang CS, Lai KS, Chou MJ, Choo KB. High prevalence of human papillomavirus infection and possible association with betel quid chewing and smoking in oral epidermoid carcinomas in Taiwan. J Med Virol 1989;28:57-61. Back to cited text no. 50 |
| 51. | Cruz IB, Snijders PJ, Steenbergen RD, Meijer CJ, Snow GB, Walboomers JM, et al . Age-dependence of human papillomavirus DNA presence in oral squamous cell carcinomas. Eur J Cancer B Oral Oncol 1996;32:55-62. Back to cited text no. 51 |
| 52. | Miller CS, Zeuss MS, White DK. Detection of HPV DNA in oral carcinoma using polymerase chain reaction together with in situ hybridization. Oral Surg Oral Med Oral Pathol 1994;77:480-6. Back to cited text no. 52 |
| 53. | Ostwald C, Müller P, Barten M, Rutsatz K, Sonnenburg M, Milde-Langosch K, et al . Human papillomavirus DNA in oral squamous cell carcinomas and normal mucosa. J Oral Pathol Med 1994;23:220-5. Back to cited text no. 53 |
| 54. | Watts SL, Brewer EE, Fry TL. Human papillomavirus DNA types in squamous cell carcinomas of the head and neck. Oral Surg Oral Med Oral Pathol 1991;71:701-7. Back to cited text no. 54 |
| 55. | Dahlstrand H, Dahlgren L, Lindquist D, Munck-Wikland E, Dalianis T. Presence of human papillomavirus in tonsillar cancer is a favourable prognostic factor for clinical outcome. Anticancer Res 2004;24:1829-35. Back to cited text no. 55 |
| 56. | Gillison ML. Human papillomavirus-associated head and neck cancer is a distinct epidemiologic, clinical, and molecular entity. Semin Oncol 2004;31:744-54. Back to cited text no. 56 |
| 57. | El-Mofty SK, Lu DW. Prevalence of human papillomavirus type 16 DNA in squamous cell carcinoma of the palatine tonsil, and not the oral cavity, in young patients: A distinct clinicopathologic and molecular disease entity. Am J Surg Pathol 2003;27:1463-70. Back to cited text no. 57 |
| 58. | Klussmann JP, Weissenborn SJ, Wieland U, Dries V, Kolligs J, Jungehuelsing M, et al . Prevalence, distribution, and viral load of human papillomavirus 16 DNA in tonsillar carcinomas. Cancer 2001;92:2875-84. Back to cited text no. 58 |
| 59. | Mork J, Lie AK, Glattre E, Hallmans G, Jellum E, Koskela P, et al . Human papillomavirus infection as a risk factor for squamous cell carcinoma of the head and neck. N Engl J Med 2001;344:1125-31. Back to cited text no. 59 |
| 60. | Fujimoto S, Takahashi M, Ohkubo H, Mutou T, Kure M, Masaoka H, et al . Comparative clinicopathologic features of early gastric cancer in young and older patients. Surgery 1994;115:516-20. Back to cited text no. 60 |
| 61. | Cruz IB, Snijders PJ, Steenbergen RD, Meijer CJ, Snow GB, et al . Age-dependence of human papillomavirus DNA presence in oral squamous cell carcinomas. Oral Oncol Eur J Cancer 1996;32B:55-62. Back to cited text no. 61 |
| 62. | Schwartz SM, Daling JR, Doody DR, Wipf GC, Carter JJ, Madeleine MM, et al . Oral cancer risk in relation to sexual history and evidence of human papillomavirus infection. J Natl Cancer Inst 1998; 90:1626-36. Back to cited text no. 62 |
| 63. | Mellin H, Friesland S, Lewensohn R, Dalianis T, Munck-Wikland E. Human papillomavirus (HPV) DNA in tonsillar cancer: Clinical correlates, risk of relapse, and survival. Int J Cancer 2000;89:300-4. Back to cited text no. 63 |
| 64. | Kreimer AR, Alberg AJ, Daniel R, Gravitt PE, Viscidi R, Garrett ES, et al . Oral human papillomavirus infection in adults is associated with sexual behavior and HIV serostatus. J Infect Dis 2004;189:686-98. Back to cited text no. 64 |
| 65. | Garrote LF, Herrero R, Reyes RM, Vaccarella S, Anta JL, Ferbeye L, et al . Risk factors for cancer of the oral cavity and oro-pharynx in Cuba. Br J Cancer 2001;85:46-54. Back to cited text no. 65 |
| 66. | Maden C, Beckmann AM, Thomas DB, McKnight B, Sherman KJ, Ashley RL, et al . Human papillomaviruses, herpes simplex viruses, and the risk of oral cancer inmen. Am J Epidemiol 1992;135:1093-102. Back to cited text no. 66 |
| 67. | Syrjanen S. Human papillomavirus (HPV) in head and neck cancer. J Clin Virol 2005;32:S59-66. Back to cited text no. 67 |
| 68. | Mineta H, Ogino T, Amano HM, Ohkawa Y, Araki K, Takebayashi S, et al . Human papilloma virus (HPV) type 16and 18 detected in head and neck squamous cell carcinoma. Anticancer Res 1998;18:4765-8. Back to cited text no. 68 |
| 69. | Miller CS, White DK. Human papillomavirus expression in oral mucosa, premalignant conditions, and squamous cell carcinoma: A retrospective review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:57-8. Back to cited text no. 69 |
| 70. | Miller CS, Johnstone BM. Human papillomavirus as a risk for oral squamous cell carcinoma: A meta-analysis, 1982-1997. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91:622-35. Back to cited text no. 70 |
| 71. | Greer RO Jr, Eversole LR, Crosby LK. Detection of human papillomavirus - genomic DNA in oral epithelial dysplasias, oral smokeless tobacco - associated leukoplakias, and epithelial malignancies. J Oral Maxillofac Surg 1990;48:1201-5. Back to cited text no. 71 |
| 72. | Gassenmaier A, Hornstein OP. Presence of human papillomavirus DNA in benign and precancerous oral leukoplakias and squamous cell carcinomas. Dermatologica 1988;176:224-33. Back to cited text no. 72 |
| 73. | Koch WM, Lango M, Sewell D, Zahurak M, Sidransky D. Head and neck cancer in nonsmokers: A distinct clinical and molecular entity. Laryngoscope 1999;109:1544-51. Back to cited text no. 73 |
| 74. | Ringstrφm E, Peters E, Hasegawa M, Posner M, Liu M, Kelsey KT. Human papillomavirus type 16 and squamous cell carcinoma of the head and neck. Clin Cancer Res 2002;8:3187-92. Back to cited text no. 74 |
| 75. | Pintos J, Franco EL, Black MJ, Bergeron J, Arella M. Human papillomavirus and prognoses of patients with cancers of the upper aerodigestive tract. Cancer 1999;85:1903-9. Back to cited text no. 75 |
| 76. | Gillison ML, Koch WM, Capone RB, Spafford M, Westra WH, Wu L, et al . Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst 2000;92:709-20. Back to cited text no. 76 |
| 77. | Ritchie JM, Smith EM, Summersgill KF, Hoffman HT, Wang D, Klussmann JP, et al . Human papillomavirus infection as a prognostic factor in carcinomas of the oral cavity and oropharynx. Int J Cancer 2003;104:336-44. Back to cited text no. 77 |
| 78. | Lindel K, Beer KT, Laissue J, Greiner RH, Aebersold DM. Human papillomavirus positive squamous cell carcinoma of the oropharynx: A radiosensitive subgroup of head and neck carcinoma. Cancer 2001;92:805-13. Back to cited text no. 78 |
| 79. | Gillison ML, Koch WM, Shah KV. Human papillomavirus in head and neck squamous cell carcinoma: Are some head and neck cancers a sexually transmitted disease? Curr Opin Oncol 1999;11:191-9. Back to cited text no. 79 |
| 80. | Nagpal JK, Patnaik S, Das BR. Prevalence of high-risk human papilloma virus types and its association with p53 codon 72 polymorphism in tobacco addicted oral squamous cell carcinoma (OSCC) patients of Eastern India. Int J Cancer 2002;97:649-53. Back to cited text no. 80 |
| 81. | Sun Y, Eluf-Neto J, Bosch FX, Muρoz N, Booth M, Walboomers JM, et al . Human papillomavirus-related serological markers of invasive cervical carcinoma in Brazil. Cancer Epidemiol Biomarkers Prev 1994;3:341-7. Back to cited text no. 81 |
| 82. | Meschede W, Zumbach K, Braspenning J, Scheffner M, Benitez-Bribiesca L, Luande J, et al . Antibodies against early proteins of human papillomaviruses as diagnostic markers for invasive cervical cancer. J Clin Microbiol 1998;36:475-80. Back to cited text no. 82 |
| 83. | Dillner J, Kallings I, Brihmer C, Sikstrφm B, Koskela P, Lehtinen M, et al . Seropositivities to human papillomavirus types 16, 18, or 33 capsids and to Chlamydia trachomatis are markers of sexual behavior. J Infect Dis 1996;173:1394-8. Back to cited text no. 83 |
| 84. | Kjaer SK, Chackerian B, van den Brule AJ, Svare EI, Paull G, Walbomers JM, et al . High-risk human papillomavirus is sexually transmitted: Evidence from a follow-up study of virgins starting sexual activity (intercourse). Cancer Epidemiol Biomarkers Prev 2001;10:101-6. Back to cited text no. 84 |
| 85. | Tanaka K, Iwamoto S, Gon G, Nohara T, Iwamoto M, Tanigawa N. Expression of surviving and its relationship to loss of apoptosis in breast carcinomas. Clin Cancer Res 2000;6:127-34. Back to cited text no. 85 |
| 86. | Ito T, Shiraki K, Sugimoto K, Yamanaka T, Fujikawa K, Ito M, et al . Survivin promotes cell proliferation in human hepatocellular carcinoma. Hepatology 2000;31:1080-5. Back to cited text no. 86 |
| 87. | Lo Muzio L, Staibano S, Pannone G, Mignogna MD, Mariggiò A, Salvatore G, et al . Expression of the apoptosis inhibitor survivin in aggressive squamous cell carcinoma. Exp Mol Pathol 2001;70:249-54. Back to cited text no. 87 |
| 88. | Mellin H, Dahlgren L, Munck-Wikland E, Lindholm J, Rabbani H, Kalantari M, et al . Human papillomavirus type 16 is episomal and a high viral load may be correlated to better prognosis in tonsillar cancer. Int J Cancer 2002;102:152-8. Back to cited text no. 88 |
| 89. | Mineta H, Miura K, Takebayashi S, Ueda Y, Misawa K, Harada H, et al . Cyclin D1 overexpression correlates with poor prognosis in patients with tongue squamous cell carcinoma. Oral Oncol 2000;36:194-8. Back to cited text no. 89 |
| 90. | Bova RJ, Quinn DI, Nankervis JS, Cole IE, Sheridan BF, Jensen MJ, et al . Cyclin D1 and p16INK4A expression predict reduced survival in carcinoma of the anterior tongue. Clin Cancer Res 1999;5:2810-9. Back to cited text no. 90 |
| 91. | Street MD, Tindle RW. Vaccines for human papillomavirus-associated anogenital disease and cervical cancer: Practical and theoretical approaches. Expert Opin Invest Drugs 1999;8:761-76. Back to cited text no. 91 |
| 92. | Brinkman JA, Caffrey AS, Muderspach LI, Roman LD, Kast WM. The impact of anti HPV vaccination on cervical cancer incidence and HPV induced cervical lesions: Consequences for clinical management. Eur J Gynaecol Oncol 2005;26:129-42. Back to cited text no. 92 |
| 93. | Premoli-de-Percoco G, Christensen R. Human papillomavirus in oral verrucal-papillary lesions: A comparative histological, clinical and immunohistochemical study. Pathologica 1992;84:383-92. Back to cited text no. 93 |
| 94. | Tomson TT, Roden RB, Wu TC. Human papillomavirus vaccines for the prevention and treatment of cervical cancer. Curr Opin Invest Drugs 2004;5:1247-61. Back to cited text no. 94 |
| 95. | Pagliusi SR, Teresa Aguado M. Efficacy and other milestones for human papillomavirus vaccine introduction. Vaccine 2004;23:569-78. Back to cited text no. 95 |
| 96. | Taira AV, Neukermans CP, Sanders GD. Evaluating human papillomavirus vaccination programs. Emerg Infect Dis 2004;10:1915-23. Back to cited text no. 96 |
| 97. | Devaraj K, Gillison ML, Wu TC. Development of HPV vaccines for HPV-associated head and neck squamous cell carcinoma. Crit Rev Oral Biol Med 2003;14:345-62. Back to cited text no. 97 |
| 98. | DiPaolo JA, Alvarez-Salas LM. Advances in the development of therapeutic nucleic acids against cervical cancer. Expert Opin Biol Ther 2004;4:1251-64. Back to cited text no. 98 |
| 99. | Tran N, Rose BR, Christopher J. O'Brien, AM. Etiology of HPV in Head and Neck Cancer. Head Neck Oncol 2007;28:64-70. Back to cited text no. 99 |
| 100. | Herrero R, Castellsaguι X, Pawlita M, Lissowska J, Kee F, Balaram P, et al . Human papillomavirus and oral cancer: The International Agency for Research on Cancer multicenter study. J Natl Cancer Inst 2003;95:1772-83. Back to cited text no. 100 |
Copyright 2009 - Journal of Cancer Research and Therapeutics
The following images related to this document are available:
Photo images
[cr09022t1.jpg]
[cr09022f1.jpg]
|

{kind=link}
{kind=link}