 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
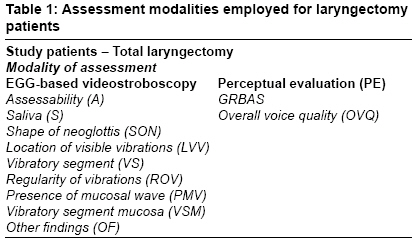
Journal of Cancer Research and Therapeutics, Vol. 5, No. 2, April-June, 2009, pp. 85-92 Original Article Is electroglottography-based videostroboscopic assessment of post-laryngectomy prosthetic speech useful? Kazi RehanA, Singh Arvind, Venkitaraman Ramachandran, Sayed SuhailI, Rhys-Evans P, Harrington KevinJ ENT and Head-Neck Surgery, Grant Medical College and Sir J. J. Group of Hospitals, Mumbai Code Number: cr09024 DOI: 10.4103/0973-1482.52792 Abstract Objectives: To use an electroglottography (EGG)-based videostroboscopy tool to assess the anatomical and morphologic characteristics of the pharyngoesophageal (PE) segment in tracheoesophageal (TO) speakers.
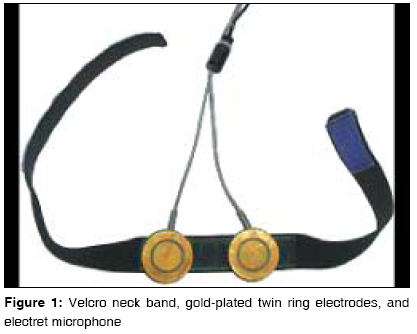
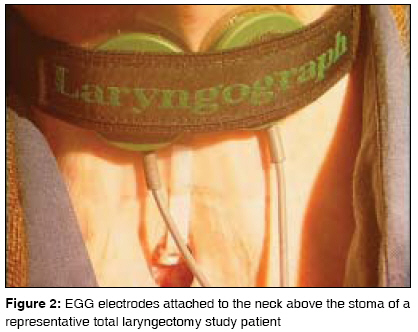
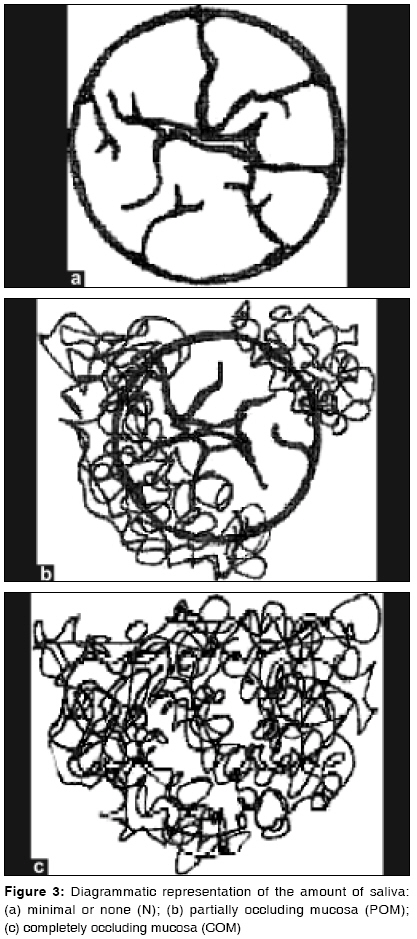
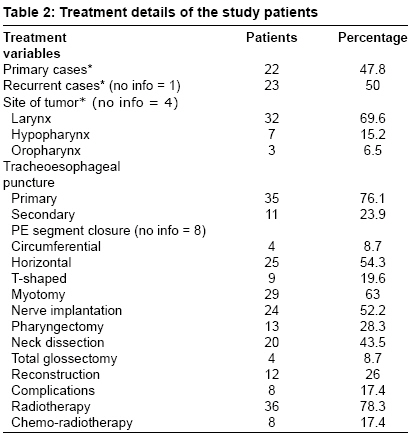
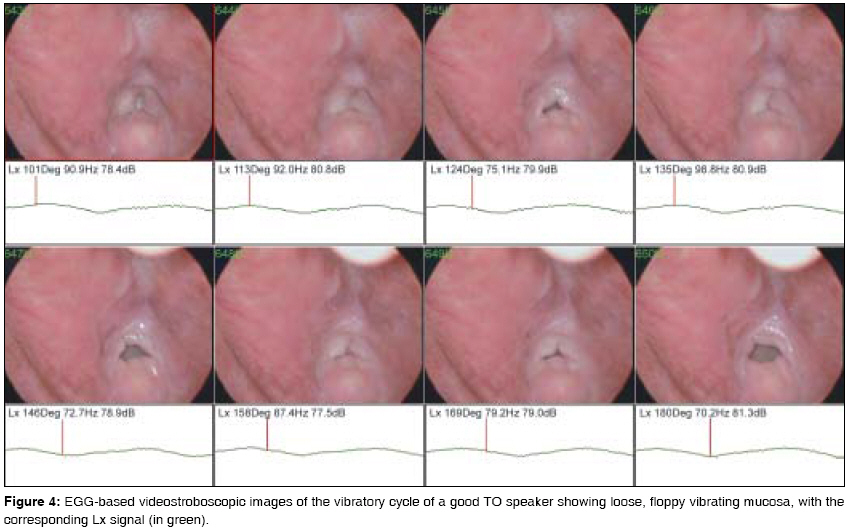
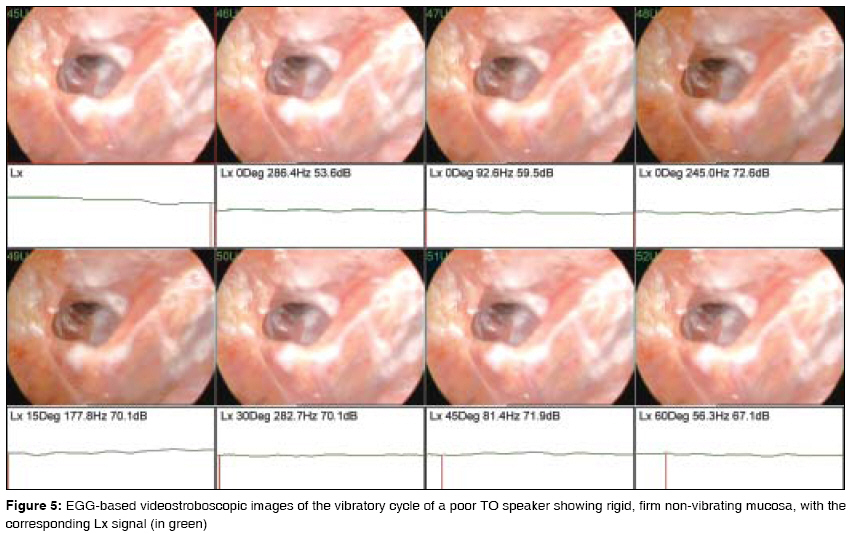
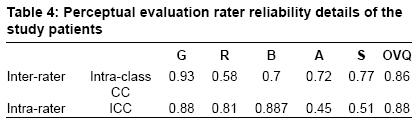
Keywords: Electroglottography, perceptual evaluation, pharyngoesophageal segment, videostroboscopy Introduction The application of stroboscopy to the study of vocal fold vibration has led to dramatic advances in the understanding of vocal fold physiology in health and disease. Laryngeal stroboscopy is now a common clinical tool and is ′an invaluable instrument in the armamentarium of the laryngeal surgeon.′ [1],[2] This technique provides valuable information about the nature of the vibration and a visual image that can be used both for immediate analysis and as a permanent record for comparison with investigations repeated at a later date. Conventional stroboscopy takes advantage of Talbot′s law by sampling the vibratory cycle at selected points from multiple waveforms. [1] An admitted limitation of the stroboscopic image is that vocal fold vibration must be relatively periodic to allow visualization of a slow-motion representation of the phonatory cycle. [2] A logical solution to this limitation is the use of a desktop computer to control the stroboscope on the basis of electroglottographically obtained period-to-period closure information. [3] In normal voice, the main acoustic excitation of the vocal tract coincides with vocal fold closure. Since this is a salient aspect, the laryngograph (Lx) signal derived from electroglottography (EGG) is widely relied on as a rich source of voice quality information in an attempt to strobe possibly even irregular, aperiodic voices. [4] In recent years this has led to the combined use of EGG-derived Lx waveform information and laryngeal stroboscopy, so that both synchronisation synchronization and wave-shape are obtained from an Lx signal source. [5],[6] Tracheoesophageal (TO) puncture and valved speech has been used for more than 20 years as an effective surgical voice restoration technique after total laryngectomy (TL). [7] However, in a small percentage of cases, effective TO speech is not achieved. [8],[9] TO speech is still regarded as variable and irregular as compared to normal laryngeal speech. Several internal and external factors (i.e., anatomical, physiological, psychological, social, and educational factors) may influence fluent speech production and this remains to be completely understood. It would be reasonable to assume that additional information on the anatomical and morphological characteristics of the neoglottis will aid in developing a more thorough understanding of TO speech. Although voice can be objectively measured in many ways, perceptual evaluation is still widely regarded as the ′gold standard.′ [10] Listeners′ judgments are usually the standard against which other measures and assessment methods of voice are evaluated and their importance essentially depends on their meaningful relation to experienced listeners′ impressions of voice quality. Therefore, in this study, we have also compared perceptual evaluation with EGG-based videostroboscopy (VS). Although several investigators over the last two decades have studied the anatomy and physiology of alaryngeal speech, only limited stroboscopic data are available on the vibratory characteristics of the PE segment in TO speakers using valved speech. [11],[12],[13],[14] Concern has been expressed that conventional stroboscopy is incapable of strobing TO speakers. [8] However, as yet, no study has examined the use of EGG-based VS in this group of patients. Therefore, the aim of this study was to explore the possible usefulness of EGG-based VS in TL patients using valved speech. A second objective was to correlate this stroboscopic data with perceptual evaluation to determine any useful links. Materials and Methods From the Hospital Speech and Language Therapy database we identified 52 patients who had undergone TL. All patients were disease free and were using the Blom-Singer voice prosthesis during the period of this cross-sectional study. The patients were assessed using a combination of EGG recording and VS [Table - 1]. Time from inception to completion of this study was 18 months. The study was approved by the local research ethics committee. For the acoustic analysis, the subject was seated in a quiet room and a pair of surface electrodes (gold-plated, measuring 3 cm in size) consisting of a ring electrode encircling each of the two other electrodes was attached a few centimeters above the stoma [Figure - 1]. The electrodes were mounted on a flexible Velcro band [Figure - 2]. The length of the band could be adjusted to hold the electrodes in a steady position all through the recording, while allowing the subject to speak comfortably and breathe naturally. A capsule electret microphone (Sony, London, UK) was used to pick up the sound; it was placed at a constant mouth-to-microphone distance of 15 cm to prevent the air burst from plosives from affecting the acoustic analysis. Electrodes were supplied with an AC sinusoidal current with a frequency (3 MHz) that was sufficiently high to be able to pass through the poorly conductive skin layer without the use of additional conductive paste. The signal was transmitted to the laryngograph processor (an all-in-one electro-laryngograph, microphone preamplifier, and speech- or laryngograph-based fundamental frequency (′pitch′) extractor). This was linked to a recorder (DAT) for the recording or playback of the speech (Sp) and laryngograph (Lx) waveforms and to the PCLX interface card which could convert the analog waveforms into digital form on a 500 MHz Pentium II-based personal computer having a graphics card with 128 MB RAM and running Windows 98E. The recording protocol was explained to all the subjects and they allowed a few practice attempts prior to commencing the recording. The Lx signal on the machine was adjusted and calibrated to the optimal gain position for each subject individually and then kept constant during the entire voice recording. Every effort was made to avoid changes in the electrode position during the recording. Similarly, after preliminary explanations and practice attempts, the stroboscopic video recordings were performed immediately following the voice recordings, in the same quiet room and with the Lx electrodes still attached to the neck. The examination was carried out with the subject seated and leaning forward from the waist, often with hands on the knees. The patient′s head was kept in a neutral position, with the chin and tongue protruded. The tongue was gently held with a piece of gauze and a rigid Machida 10mm, 70° scope was introduced into the oropharynx, taking care to avoid touching the soft palate. The scope was powered by a 300 W Xenon light source attached to a Hitachi 3CCD remote head camera connected to the personal computer. The patient was asked to produce a sustained vowel (/e/) at a comfortable pitch and loudness for at least 2-10 s. Recordings were made with a stroboscopic flashlight (Lx synchronized) during phonation. Occasional patients with a severe gag reflex required a topical anesthetic spray. The best of three consecutive video recordings was saved for further viewing and analysis. A laryngeal stroboscopy scoring and evaluation sheet was created with adaptations from the work done by Van. [8] The protocol consisted of nine well-defined subjective parameters. Two of the parameters were accompanied by companion line diagrams to help further quantification. Three experienced otolaryngologists were used as raters. Raters were blinded to the subject′s identity. Recordings were played from the computer monitor at a standard distance of 20cm. The video recordings were replayed at different speeds and as many times as necessary in each session for the rater to come to a final decision. Assessability (A) was scored as: visible (V) - view of multiple consecutive frames (>10) of vibrating mucosa on screen; partly visible (PV) - view of multiple consecutive frames (< 10) of vibrating mucosa; or not visible (NV). Saliva/mucus (S) present in the neoglottis was estimated as: minimal or none (N); partially occluding mucosa (POM), and completely occluding mucosa (COM) [F on a 500 MHz Pentium II-based personal computer having a graphics card with 128 MB RAM and running Windows 98E [Figure 3a],[Figure 3b],[Figure 3c]. Shape of neoglottis (SON) defined the predominant geometric shape of the neoglottis in a vibratory cycle as: circular (C) ; on a 500 MHz Pentium II-based personal computer having a graphics card with 128 MB RAM and running Windows 98E triangular (T) ; split side-to-side (SSS) ; split anterior-to-posterior (SAP) ; irregular (I ); or not assessable (NA) . Location of visible vibrations (LVV) defined the predominant site/s of mucosal vibrations as: posterior (P) ; ant Location of visible vibrations (LVV) anterior (A) ; left (L) ; right (R) ; all walls (AW); or not assessable (NA). Vibratory segment (VS) gave an overall estimate of the strength of vibrations in the vibratory segment as: strong (S) - obvious well-defined vibrations over multiple frames; weak (W) - poorly defined vibrations over a few frames only; moderate (M) - in between the two above categories, neither strong nor weak vibrations; absent (A) - no vibrations seen in any frame; or not assessable (NA). Presence of mucosal wave (PMW) differentiated a mucosal wave (in analogy to the travelling wave on vocal folds) from the vibrations of the wall of the neoglottis or reconstructed pharynx. This was scored as: strong (S) - obvious well-defined travelling wave from inferior to superior over multiple frames associated with a strobe effect; moderate (M) - a travelling wave from inferior to superior over a few frames; weak (W) - a poorly defined travelling wave from inferior to superior over 1-2 frames; absent (A) - no travelling wave seen in any frame; or not assessable (NA). Regularity of vibrations (ROV) scored the visual impression of the regularity of the vibrations as: regular (R) - associated with a consistent shape of the wave across multiple frames; irregular (IR) - not associated with a consistent shape of the wave across multiple frames; or not assessable (NA). Vibratory segment mucosa (VSM) gave an estimate of the tone/state of the mucosa of the vibratory portion of the PE segment as: floppy mucosa (FM) - loose, flacid, and floppy mucosa exhibiting good volitional control/ movement; rigid mucosa (RM) - firm, rigid mucosa exhibiting poor volitional control/ movement; or unremarkable mucosa (UR) - no outstanding or remarkable diagnostic features. Other findings (OF) noticed during stroboscopy were also recorded, such as a pseudo-epiglottis or any outstanding or unusual mucosal lesion or feature. We used two experienced otolaryngologists as raters to grade the patients using the widely used GRBAS scale of the Japan Society of Logopaedics and Phoniatrics. [15] This system consists of five well-defined parameters: G (overall grade of hoarseness), R (roughness), B (breathiness), A (asthenicity), and S (strain). Each parameter is scored using a 4-point ordinal scale from 0 to 3 (0 - normal, 1 - mild, 2 - moderate, and 3 - severe). The patients were asked to read a common standard passage called ′Arthur the rat′ at a comfortable pitch and loudness. The raters were blinded to the subject′s identity. Recordings were played from two speakers at a standard distance of 1 m in a quiet room. The recordings were replayed as many times as necessary in each session for the raters to come to a final decision on the GRBAS score. Apart from the GRBAS, the raters were also asked to give a simple overall judgment of the voice quality (OVQ) for each patient to assist assess the correlation. OVQ consisted of three categories: G (good - near normal/normal voice), P (poor - very deviant from a normal voice), and R (reasonable - between the two categories). Data were entered into a worksheet (Excel 05; Microsoft Corp, Washington) and the means (±SD) were computed. Statistical analysis was performed using the Statistical Package for Social Sciences 14.0 (SPSS Inc, Chicago version III). Statistical differences between patient groups for the stroboscopy parameters was assessed using Pearson′s chi-square tests with sociodemographic and treatment variables such as age, sex, neck dissection, primary/recurrent cases, myotomy, nerve implantation, reconstruction procedure, pharyngoesophageal (PE) segment closure, chemotherapy, radiotherapy, and complications. Chi-square tests were used to find the correlation between GRBAS and OVQ assessment. Only G of GRBAS was selected for correlation as this represents the overall grade of hoarseness and is widely believed to be the most reliable/consistent of the five parameters. [15] This was confirmed in our inter- and intra-rater (test-retest) reliability tests using intra-class correlation coefficients (ICCC;> 0.80 is considered as high). A P value less than 0.05 was considered as significant. Results Of the 52 patients in the study, VS recordings were possible in only 46 patients (one patient refused; four exhibited severe gagging that was resistant to all methods of control; and one patient had a short immobile tongue, precluding examination). There were 36 males and 10 females with a mean age of 63.4 ± 10.5 years. All patients were using the Blom-Singer valve. Median time since TL was 2 years. The treatment details of the study patients are shown in [Table - 2]. A strobe effect was seen in only nine patients in our study. The details of the videostroboscopic parameters of our study patients [Figure - 4],[Figure - 5] were as follows: The neoglottis/neopharynx was visible (V) in 26 patients; saliva (S) was not an issue (N) in 20 patients, split shapes were the most common (SSS in 15 and SAP in 11 patients); LVV was associated with AW in 16 patients; a strong vibratory segment was seen in nine patients; regular (R) vibrations were seen in only nine patients; presence of mucosal wave (PMW) was seen in nine patients and was associated with a strobe effect; floppy, loose mucosa was seen in 12 patients and rigid, firm mucosa in only two patients; no unusual mucosal lesion was noticed apart from a pseudo-epiglottis in seven patients. We had an equal number of patients ( n = 13) in both the G1 category of the GRBAS and the good voice category of the OVQ. Other scores for the GRBAS scale were G2 in 25 patients and G3 in six patients. For the OVQ, 26 patients were scored as having a reasonable voice and five patients as having poor voice. Using Pearson′s chi-square tests, we found significant statistical correlation between G1/good OVQ and little or no saliva ( P = 0.03 and 0.02, respectively) and LVV on all walls of the neoglottis ( P = 0.05 and 0.03, respectively). Using Pearson′s chi-square tests, statistically significant differences were found between patients subgroups for individual parameters between saliva according to site ( P = 0.01) and reconstruction ( P = 0.009). Significant correlation was also seen between ROV and site ( P = 0.01), PMW with pharyngectomy ( P = 0.05), primary cases ( P = 0.03) and, finally, between VSM and nerve implantation ( P = 0.02). Test-retest assessment using ICCC for the parameters was very high at> 0.9. Finally inter-rater agreement among the three expert raters using ICCC for the parameters was again high (>0.8). Only one parameter (vibratory segment) exhibited low reliability (0.425) [Table - 3]. Inter- and intra-rater reliability was very high between G of GRBAS and OVQ. The details are as shown in [Table - 4]. Discussion The methodology followed for EGG-based VS in laryngectomees is very similar to that for other groups of patients, except with regard to the placement of the gold-plated electrodes. During this study, we experimented with different sizes and placement positions of the electrodes. From our experience we feel the regular-sized adult laryngeal electrodes are the best option. In order to prevent an overload/underload of the Lx waveform, we believe that the electrodes should be placed roughly 4 cm apart and 2-3 cm above the stoma. However, this position may need to be individualized to obtain an optimal waveform. Using a rigid scope we were able to strobe only around 20% of the study patients, which was a big disappointment considering the sound theoretical background of methodology used. This is in large part due to the highly variable and irregular nature of alaryngeal voice, making synchronization extremely difficult even with EGG. The neoglottis was assessable in only 56% of our patients as the presence of saliva obstructed the view in the rest of the cases. On investigating the possible correlation between stroboscopy parameters and the voice quality, we found significant correlation only with saliva and the LVV. Our good speakers exhibited little or no saliva and mucosal vibrations involving opposing walls of the neoglottis. Saliva was an issue in almost 60% of our series, causing a wet and gurgly voice and precluding effective examination. We tried a number of ways to overcome this but were unsuccessful. In addition, we noticed a lot of reflux of saliva/secretions in these patients and are unsure of its exact origin. The significant correlation with the LVV could be a reflection of better and widespread volitional mucosal control. We did not find any correlation with SON and this is understandable as we found a mix of shapes in our group of patients. In addition, this parameter is difficult to quantify as the shape of the neoglottis is constantly changing during phonation.[8] However, we were surprised to find no correlation between voice quality and vibratory segment, regularity of vibrations, presence of mucosal wave, and vibratory segment mucosa. This suggests that acceptable voice quality can be achieved even in TO speakers with irregular vibrations, moderate vibratory segments, and poor mucosal waves. Furthermore, the inability of the commonly measured parameters derived from VS to predict voice quality in TL patients raises real concerns about the justification for subjecting these patients to this invasive investigation. [8],[13] A number of our stroboscopy protocol parameters showed correlation with treatment variables. While some are understandable (like the relationship of saliva and reconstruction), the influence of nerve implantation on the vibratory segment mucosa is interesting and deserves further dedicated research. Perceptual evaluation is essential for the assessment of vocal quality, overall severity of defects, and their impact on communication skills. The reliability of the raters′ perceptions is known to be influenced by a number of factors, such as the experience and training of the raters, the voice pathology, and the type of speech material. [16],[17],[18] We used only experienced raters and a common standard passage as this has been shown in literature to be most reliable. We used the OVQ as this has been used before and found to be reliable in laryngectomees. Both systems showed good correlation with each other. The high inter- and intra-rater reliability values of our perceptual evaluation allowed useful comparison with the other outcome measures used in this study. Our protocol consisted of nine subjective parameters that were based on previous experience in the field. [8],[14] They were supplemented with simple line diagrams to improve quantification and association and this was appreciated by the experienced raters. In spite of the multidimensionality of the parameters, there was good inter- and intra-rater reliability. Only one parameter (vibratory segment) showed low reliability. Given that the statistical reliability of the calculations depends on significant variability in the responses from the raters, it could be possible that the low reliability of these dimensions as determined by the Spearman rho test can be attributed to the low variance present in the ′cases′ and may not represent a true limitation of the parameter. This study brings to light a number of key points. EGG-based VS still has serious limitations, especially in the highly variable, aperiodic TO speech. [15] Firstly, although EGG-based VS is an interesting concept in theory, we have not been able to get any more useful information/data in our study with laryngectomy patients than we would have with regular conventional scopy or stroboscopy. Thus, in this particular set of patients, EGG-based VS does not provide the clinician with any additional useful information that can contribute to decision making. Also, it is an invasive procedure, can be uncomfortable, and the rigid scope technique interferes with alaryngeal voicing. Correct placement of the electrodes so as to avoid overloading the waveform can be difficult and needs to be individualized. Importantly, the strobe effect and accessibility was very limited with the rigid scope, at least in our study. Although the use of EGG has possibly improved its functionality in irregular voices with regards to irregular voices, it is still difficult to strobe all irregular voices. This possibility needs to probed further in a larger study. Assessment of the PE segment in laryngectomees by other modalities such as conventional VS has been used by Dworkin et al. and more recently by digital high-speed imaging. [19],[20] Van As et al . concluded that high-speed systems have greater promise than other methods of stroboscopy and are ideally suited, in theory at least, for irregular and highly aperiodic voices (e.g., in TO speakers). With the rigid scope, it is only possible to have a bird′s-eye view of the neoglottis. It is not possible to see the origin of the vibratory segment or its length. Indeed, if there is more than one vibratory segment, this will not be known. Moreover, no data are obtained on the valve or the rest of the PE segment and this can be vitally important. Perhaps the use of a flexible videostrobsocopy system would be better in some respects. Another important limitation is its slow frame rate which can result in loss of information. Finally, its interpretation is dependent upon the skill and experience of the performing clinician, and more specifically, that of the diagnostic interpreter. Conclusion Laryngeal stroboscopy is widely agreed to be the single most important clinical voice assessment tool. This study is the first dedicated research on the use of an EGG-based stroboscopy instrument to evaluate TO prosthetic speech. Our observations suggest that as far as functional voice is concerned, saliva and LVV had statistically significant effects on voice quality. EGG- based stroboscopy, although is an attractive concept in theory, still has serious limitations, the most notable being that it is difficult to strobe all irregular and highly variable TO speakers.References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09024t3.jpg] [cr09024f4.jpg] [cr09024f1.jpg] [cr09024t1.jpg] [cr09024f5.jpg] [cr09024f3.jpg] [cr09024f2.jpg] [cr09024t2.jpg] [cr09024t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}