 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
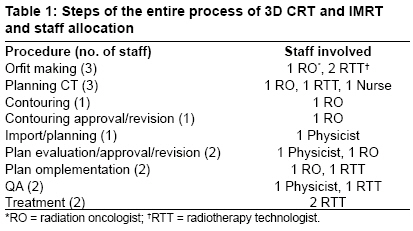
Journal of Cancer Research and Therapeutics, Vol. 5, No. 2, April-June, 2009, pp. 107-112 Original Article Time trial: A prospective comparative study of the time-resource burden for three-dimensional conformal radiotherapy and intensity-modulated radiotherapy in head and neck cancers Murthy Vedang, Gupta Tejpal, Kadam Avinash, Ghosh-Laskar Sarbani, Budrukkar Ashwini, Phurailatpam Reenadevi, Pai Rajeshri, Agarwal Jaiprakash Department of Radiation Oncology, Tata Memorial Hospital and Advanced Centre for Treatment, Research and Education in Cancer (ACTREC), Tata Memorial Centre, Navi Mumbai Code Number: cr09027 DOI: 10.4103/0973-1482.52800 Abstract Introduction: An ongoing institutional randomized clinical trial comparing three-dimensional conformal radiotherapy (3D CRT) and intensity-modulated radiotherapy (IMRT) provided us an opportunity to document and compare the time-manpower burden with these high-precision techniques in head and neck cancers.Materials and Methods: A cohort of 20 consecutive patients in the ongoing trial was studied. The radiotherapy planning and delivery process was divided into well-defined steps and allocated human resource based on prevalent departmental practice. Person-hours for each step were calculated. Results: Twelve patients underwent IMRT and eight patients had 3D CRT. The prerandomization steps (upto and including approval of contours) were common between the two arms, and expectedly, the time taken to complete each step was similar. The planning step was carried out postrandomization and the median times were similar for 3D CRT (312 min, 5.2 person-hours) and IMRT (325.6 min, 5.4 person-hours). The median treatment delivery time taken per fraction varied between the two arms, with 3D CRT taking 15.2 min (0.6 person-hours), while IMRT taking 27.8 min (0.9 person-hours) (P<0.001). The total treatment time was also significantly longer in the IMRT arm (median 27.7 versus 17.8 person-hours, P<0.001). The entire process of IMRT took 48.5 person-hours while 3D CRT took a median of 37.3 person-hours. The monitor units delivered per fraction and the actual "beam-on" time was also statistically longer with IMRT. Conclusions: IMRT required more person-hours than 3D CRT, the main difference being in the time taken to deliver the step-and-shoot IMRT and the patient-specific quality assurance associated with IMRT. Keywords: Intensity-modulated radiotherapy, three-dimensional conformal radiotherapy, workload, person-hours, burden, manpower Introduction Head and neck squamous cell carcinoma (HNSCC) is ideally suited for treatment with intensity-modulated radiation therapy (IMRT) due to the presence of complex target volumes in close proximity to critical structures and the proven need for high doses of radiation for long-term control. Several studies on IMRT in HNSCC have shown impressive outcomes in terms of improved locoregional control, decreased acute toxicity, and better quality of life (QOL), though long-term results are still awaited. [1],[2],[3],[4],[5] Despite several potential advantages, this revolutionary new technology is not readily available in many centers, even in the developed world [6] due to economical, technical, and logistical factors, such as the need to procure additional software and hardware, human resource issues, and time-burden implications on a busy clinical department. A suitable alternative to inverse planning typically associated with IMRT could be the use of forward planning with three-dimensional conformal radiotherapy (3D CRT) to produce dose distributions superior to conventional two-dimensional (2D) treatment. [7],[8] While concerns have been raised regarding the resource implications with the use of IMRT at various sites, only a handful of studies have addressed this issue by measuring the additional time burden imposed by its introduction in clinical practice. [9],[10],[11],[12] No study has previously directly compared each step involved in the treatment planning and delivery process of 3D CRT and IMRT in HNSCC. A prospective randomized trial comparing 3D CRT and IMRT in moderately advanced HNSCC with appropriate clinical endpoints is currently ongoing at our institution. Clinical and dosimetric results of this trial are still awaited, and will be reported in due course. This trial provided us with an opportunity to prospectively document and compare the time-manpower resource burden involved with the use of these high-precision radiotherapeutic techniques in head and neck cancers. Materials and Methods The study population consisted of a cohort of 20 consecutive patients randomized into one of the two treatment arms of an ongoing trial comparing forward planned 3D CRT with inverse planned IMRT in moderately advanced HNSCC between May and November 2007. These 20 patients were accrued during the mid-course of the primary trial reducing the influence of the learning curve associated with such high-precision and resource-intensive techniques. The inclusion criteria for the primary trial was previously untreated, histologically proven squamous cell carcinoma of the oropharynx, hypopharynx or larynx staged as T1-T3 (excluding T1 vocal cord) and N0-2b with no distant metastases planned for radical intent treatment with definitive radiotherapy with or without concurrent systemic chemotherapy as per the prespecified protocol. For the purpose of this study for assessing the time burden, the entire planning and delivery process was divided into specific steps [Table - 1]. Each step is a well-defined entity, and was allocated human resource based on prevalent departmental practice to aid in the estimation of time and human resource requirement. A time sheet was maintained during the entire process of planning, verification, and delivery. To objectively describe the time-person burden required for the process, person-hours for each step were calculated as follows:
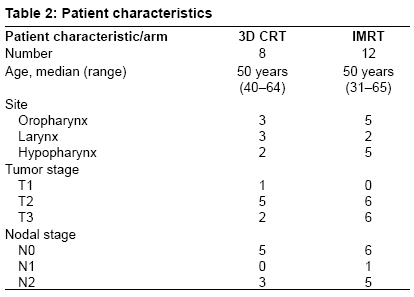
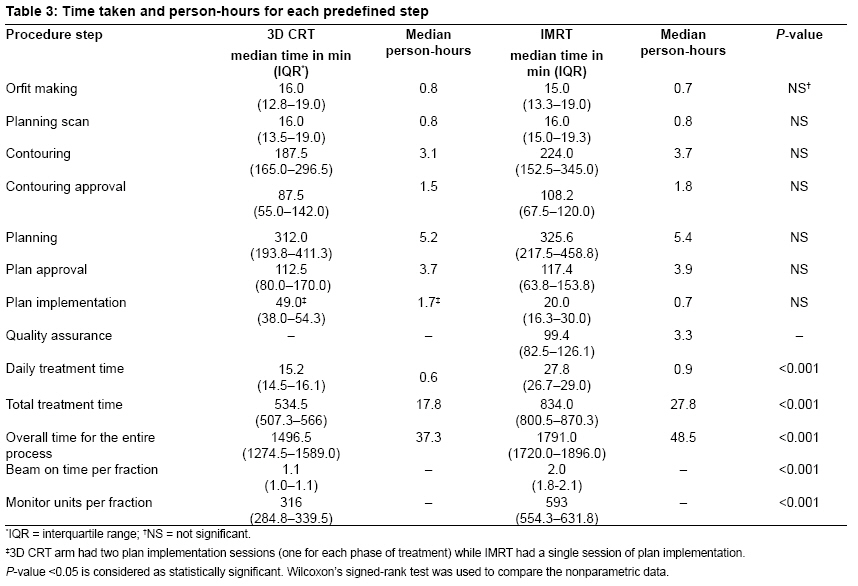
Immobilization Planning CT scan Contouring Contouring approval Physics planning Treatment planning IMRT planning was done using 6-MV photons with seven to nine equispaced coplanar beams with five to seven intensity levels. The inverse planning module of Plato uses a gradient-search algorithm for optimization. Unlike 3D CRT, which was planned in two phases as a sequential boost, IMRT was a single-phase plan using the simultaneous integrated boost (SIB) technique. The gross disease with margins was planned with a higher dose per fraction (220 cGy/fraction) for 30 fractions for a total dose of 66 Gy in 30 fractions, whereas the high-risk and low-risk elective volumes were treated with a lower dose per fraction (200 and 180 cGy/fraction, respectively) for 30 fractions. Radiobiologically, both the 3D CRT and IMRT doses that were employed were deemed equivalent. Plan approval Plan implementation Quality assurance Absolute output measurement of the machine was done using 0.6-cc cylindrical ion chamber at a 5-cm depth with a field size of 10 x 10 cm 2. The IMRT plan was then transferred to a virtual water phantom with the isocenter set at the center of the effective volume of the ion chamber, placed at a depth of 5 cm. Profiles were generated for each beam and points defined off-axis in the plateau region, away from any sharp dose gradients. Doses at these points were also noted from the planning system. Measured doses and calculated doses were compared and confirmed with film dosimetry. Set-up verification and treatment delivery Results Twenty patients were included in the study. Patient demographics are shown in [Table - 2]. There were 12 patients who had IMRT, and 8 patients had 3D CRT. [Table - 3] shows the median time taken to undertake each defined step with the two techniques. The prerandomization steps (up to and including contouring approval) were similar between the two arms and expectedly the time taken to complete each step was no different. The contouring step had a wide range in both the arms due to the involvement of the junior trainees with varying level of experience. The planning step was carried out postrandomization, and the median time taken for producing a 3D CRT plan was 312 min (5.2 person-hours), while the IMRT plan took a median of 325.6 min (5.4 person-hours). This difference was not statistically significant. The time taken for the daily treatment varied between the two arms, with 3DCRT taking a median of 15.2 min (0.6 person-hours) for each fraction while IMRT taking longer at a median of 27.8 min (0.9 person-hours). This difference (and the difference in person-hours) was statistically significant. The total treatment time was also significantly longer in the IMRT arm (median 27.7 versus 17.8 person-hours, P < 0.001). QA was an additional step taken in patients undergoing IMRT only, and the process took an additional median time of 99.4 min (3.4 person-hours). The entire process of IMRT took 1791 min (48.5 person-hours) and was significantly longer than the process of 3D CRT which took a median of 1496.5 minutes (37.3 person-hours). The monitor units delivered per fraction and the actual "beam-on" time was also statistically different for the two arms. Discussion While the comparative dosimetric and clinical outcomes with these techniques will be evaluated and reported once the trial concludes in due course, this randomized trial provided us with an opportunity to prospectively estimate and document the time and human resource burden required by a department while undertaking resource-intensive procedures such as 3D CRT and IMRT in HNSCC. This study showed that the time required for the process of IMRT is significantly longer than that for 3D CRT in HNSCC with the main difference being in the duration of treatment delivery and the extra procedure of patient-specific QA with IMRT. There is an anticipated benefit with high-precision techniques in HNSCC. While IMRT has been used, evaluated, and reported extensively, [1],[2],[3],[4],[5] the utility and feasibility of 3D CRT remains relatively untested in this setting. In limited resource centers, 2D treatment with conventionally simulated fields is still considered as the standard of care. Current best evidence mandates a paradigm shift from conventional 2D to volumetric-imaging-based high-precision radiotherapy. However, there is a steep learning curve associated with the introduction of IMRT in a busy clinical department. In addition, this has significant logistic, technical, financial, and human resource implications and may not be practically achievable universally. [6] Moreover, this technology is being aggressively promoted and marketed while open questions remain about its long-term efficacy and cost effectiveness. [14] In order to circumvent some of these issues while attempting to improve the therapeutic ratio, use of 3D CRT may be considered as a suitable intermediate step, which has been largely ignored by the head and neck radiation oncology community. Although, based on the published evidence, the value of IMRT in sparing normal tissues while enabling dose escalation is unquestionable, the role of 3D CRT as a suitable alternative needs to be better defined. The parent trial design mandated that randomization should be done after the approval of volume delineation. This not only reduced the potential bias during the contouring process but also maintained consistency in volume delineation. As a result, the time taken for the preplanning steps was very similar in the two arms. Although detailed data on the time burden for immobilization and CT simulation are not available in the literature, they are likely to be similar to our results across institutions. The time spent on volume delineation is a direct function of the experience of the clinician and is likely to be variable. This time is also likely to reduce as the learning curve is negotiated. Our results of the contouring time are similar to those from Miles et al . who reported a median contouring time of 2.3 h (range 0.7-3.5 h) for IMRT in head and neck cancers with the authors admitting a more variable time requirement for head and neck than prostate and pelvic nodal contours. [11] The reason for this variability though not specified is likely to be similar to what has been reported here. We found no statistically significant difference in the time taken for the actual physics planning between 3D CRT and IMRT. Based on our experience gained while planning the treatment of the first 20 patients in the trial (prior to starting this time trial), a significantly longer planning time was expected for 3D CRT as compared to IMRT. However, this was not the case and both the techniques took similar times for planning. It is difficult to say whether this was purely due to chance or related to the learning curves associated with either of these techniques. The optimization and planning time obtained in this study are similar to those reported in the multicenter ESTRO-QUASIMODO project. [15] According to our departmental guidelines and based on the trial protocol requirements, patient-specific QA was carried out as an extra step in patients receiving IMRT. This added substantially to the overall time taken per patient. Palta et al . [16] have indicated that the current "estimates′ of the additional time necessary for patient-specific QA in an IMRT program of 40 patients per year is 200 h. The main difference in the two treatment techniques was however the time taken for the actual treatment delivery (room-in to room-out) with 3D CRT taking a median of 15.2 min as compared to 27.8 min for IMRT ( P < 0.001). When restricting the analysis to radiation beam-on time and monitor units delivered, this difference remained statistically significant. While the monitor units and consequently beam-on time were longer for IMRT, they only partially contributed to the overall increase in the daily time by 10 min with IMRT, the main reason being the time for MLC repositioning inherent to the step-and-shoot IMRT. The IMRT treatment time in our study is longer than that reported in the Royal Marsden Hospital study (median 12 min) [11] and the ESTRO-QUASIMODO study (mean 19 min). [15] This could partly be due to the difference in the methods of time measurement (on-couch to off-couch versus room-in to room-out). It could also be influenced by the number of fields and other technical aspects of treatment delivery such as the machine output and the dynamic mode of treatment delivery. Overall, the delivery time was generally similar to that reported in the indexed medical literature for head and neck cancers. [10],[12],[15],[17] This work was an attempt to estimate the time-human resource burden prospectively while undertaking 3D CRT and IMRT in HNSCC in a clinical trial setting. Although in a busy service setting the time for each step may be reduced, the overall time difference between the two arms is still likely to persist. Simplification of the step-and-shoot IMRT technique may help reduce the planning and treatment delivery time further. [18] Although undertaking patient-specific QA and defining action levels before IMRT are common in most centers, there is some debate if this procedure can be omitted particularly after gaining considerable experience with IMRT. Further reductions in the time required for these procedures is likely with standardization of procedures, increasing familiarity, and use of class solutions. Acknowledgment The authors are thankful to Mrs. Sadhana Kannan for her assistance with statistical analysis and data management.References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09027t2.jpg] [cr09027t3.jpg] [cr09027t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}