 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
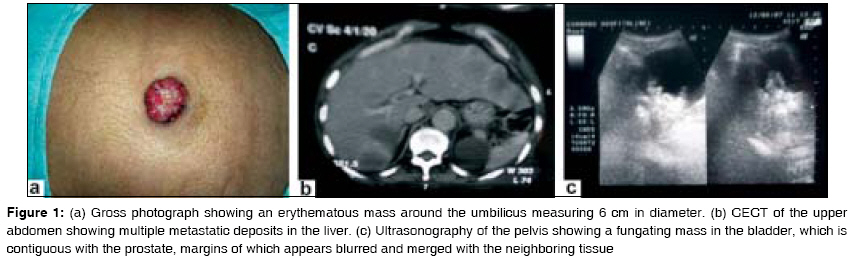
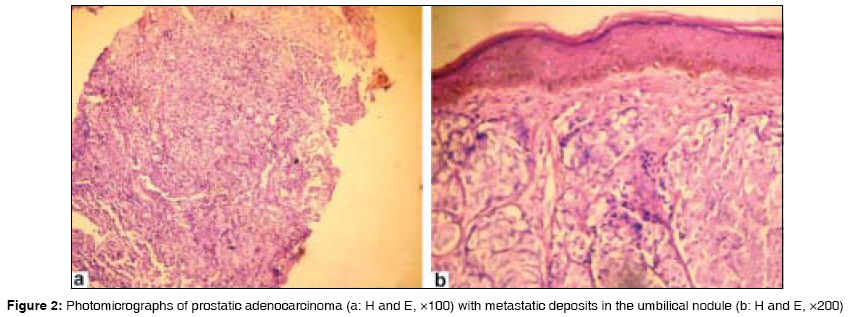
Journal of Cancer Research and Therapeutics, Vol. 5, No. 2, April-June, 2009, pp. 127-129 Case Report Sister Mary Joseph nodule as the presenting sign of disseminated prostate carcinoma Deb Prabal, Rai RadheyShyam, Rai Rahul, Gupta Ekawali, Chander Yogesh Department of Pathology, Military Hospital, Udhampur, Jammu & Kashmir Code Number: cr09032 DOI: 10.4103/0973-1482.52793 Abstract Sister Mary Joseph's nodule is referred to as metastasis of visceral malignancy to the umbilicus. Most common primaries are in the gastrointestinal or genital tract, while other locations are rare. We recently encountered a 76-year-old male who was referred to the surgery clinic with an erythematous nodule in the umbilicus measuring 6 cm in diameter with complaints of painless profuse hematuria. History revealed severe obstructive voiding symptoms of 2-year duration, along with significant loss of weight and difficulty in walking. A detailed examination showed hard nodular hepatomegaly, along with grade IV prostatomegaly. Serum prostate-specific antigen was 3069 ng/ml. A pelvic radiograph displayed multiple osteolytic lesions, while ultrasonography showed multiple iso- and hypoechoic lesions in both lobes of the liver, suggestive of metastasis. Histopathology of a Tru-cut biopsy of the prostate confirmed an adenocarcinoma (Gleason score 9) with umbilical metastasis. The patient was on regular follow-up and died 3 months later.Keywords: Metastasis, prostate carcinoma, umbilicus Introduction The ′Sister Mary Joseph nodule′ (SMJN) is referred to as metastasis of visceral malignancy to the umbilicus. Most common sites of origin are in the gastrointestinal or genital tracts, while other locations are rare. [1],[2],[3],[4],[5],[6],[7],[8] Prostate as a primary site has been reported in few case reports only. [1],[2],[3],[4],[5],[6],[7]We recently encountered a 76-year-old male who presented with umbilical nodule, which was subsequently diagnosed as a case of prostate carcinoma with extensive metastases. Case Report A 76-year-old man was referred to the surgery clinic with painless profuse hematuria associated with an umbilical nodule. History revealed severe obstructive voiding symptoms of 2-year duration, along with significant weight loss over past 6 months and difficulty in walking. He was a known hypertensive on regular medication since past 30 years, and there was no other systemic illness. A detailed examination showed hard nodular hepatomegaly, along with grade IV prostatomegaly. Serum prostate-specific antigen (PSA) was 3069 ng/ml. An examination revealed a poorly nourished male with normal vital parameters. A per abdominal examination showed an erythematous, nontender mass around the umbilicus measuring 6 cm in diameter [Figure 1a]. Liver was enlarged, firm- to- hard in consistency, nodular, and nontender. There was no free fluid in the peritoneal cavity. Direct rectal examination (DRE) revealed grade IV hard nodular prostate with obliteration of median sulcus. Serum PSA was 3069 ng/ml. Ultrasonographic and contrast-enhanced computerized tomography (CECT) studies of upper abdomen and pelvis showed a fungating mass in the bladder, which was contiguous with the prostate. The latter measured 5 x 3.2 x 7 cm in size and 69 g in weight. The prostate had irregular and indistinct capsular margins, which appeared merged with the neighboring tissue [Figure 1b]. The rectoprostatic planes and those between the seminal vesicles and prostate were indistinct. The liver was 14.5 cm in mid-clavicular line, with multiple iso- and hypoechoic lesions in both lobes suggestive of metastasis [Figure 1c]. In addition, it also revealed a 35 x 15 mm sized enhancing umbilical nodule with a soft-tissue defect in the left periumbilical region. A pelvic radiograph showed multiple osteolytic lesions, while chest radiographs were normal. Histopathology of six-quadrant trucut biopsy specimen from the prostate showed features of adenocarcinoma (Gleason score 9) [Figure 2a], while biopsy from the umbilical nodule confirmed presence of adenocarcinoma metastasis [Figure 2b]. The patient was on regular follow-up and died 3 months later. Discussion Neoplastic nodules in the umbilical region are uncommon and generally represent metastases from distant tumors. Furthermore, umbilical metastasis of visceral malignancy is rare and is encountered in 1-3% of all intra-abdominal and/or pelvic malignancy. [8] In various series, [1],[2],[8],[9] the most common sites of primary tumors were the stomach and colon in males, and ovaries in females. In the series of Charoenkul et al. , [10] the site of origin remained unknown in as many as 30% cases. Other reported primary sites were the cecum, pancreas, gall bladder, fallopian tube, and endometrium, [1],[8],[10] and rarely from the lung and prostate. [1],[2],[3],[4],[5],[6],[7] SMJN as the initial manifestation of an internal malignancy has been reported in 14-45% cases in various series, [11] and case reports, [1],[4],[11] including secondaries originating from prostatic adenocarcinoma, [1],[2],[3],[4],[5],[6],[7] similar to the present case. Most of the metastatic lesions to the umbilicus were irregular firm nodules, measuring 1-1.5 cm in diameter, with occasional cases of diameter as large as 10 cm. [12] These lesions are occasionally painful, rarely ulcerated, and may show mucoid discharge depending on the primary tumor. Our case was erythematous, nontender, and measured 6 cm in diameter. The differential diagnosis of this uncommon condition includes nonmetastatic diseases like umbilical hernia, hypertrophic scar, pyogenic granuloma, and pilonidal sinus. [9] Interestingly, the literature is replete with cases masquerading as umbilical hernias finally turning out to be metastatic deposits. [8] Histopathology, including immunohistochemistry, [2],[3] plays a vital role in confirming and suggesting possible sites of primary tumors. Though prostatic adenocarcinoma is one of the most frequently diagnosed tumors in the male population, the most common sites of secondary involvement are iliac lymph nodes, bones, and lungs, and rarely bladder, liver, testis and brain. [13] Skin is an uncommon site, with prostate carcinoma accounting for less than 1% of all skin metastases. [4] The common areas for skin metastases include the penis, anterior aspect of the thighs, suprapubic area, and the perineum, with few cases reported in the scalp, chest, back, and even the face. [4] Umbilical involvement is rare, and has been reported in about seven cases only. [1],[2],[3],[4],[5],[6],[7] Of all the cases of cutaneous metastasis of prostate cancer reported in Japan, only three metastases have occurred in the umbilical region. [2],[5],[6] The present case not only showed umbilical metastasis but also a presence of multiple secondaries in the liver and bone. A recent review by Gabriele et al . [14] has discussed the various mechanisms of umbilical metastasis of visceral malignancy, namely, venous, arterial, lymphatic, and direct extension. In the present case, metastatic deposits in the bones and liver were possibly blood borne as well as a resultant of the lymphatic spread, while the mass in the urinary bladder was due to direct infiltration of prostate carcinoma. Irrespective of the primary site, SMJN is an ominous diagnostic sign heralding a poor prognosis with fatal outcomes. A mean survival time of 10 months has been reported, with rare cases surviving 2 years after initial diagnosis. In contrast, SMJN is a late feature in patients with prostate adenocarcinoma, with most cases already having multiple metastases. Thus, the overall outcome in these cases is more dismal with survival ranging between 2 and 10 months (mean 4 months), similar to the index case [Table - 1]. Management of these cases is controversial, with some advocating aggressive surgery and adjuvant therapy, [9],[12] while others recommending palliative therapy, in view of the poor prognosis. [10] To conclude, we report a rare case of prostate adenocarcinoma presenting as an umbilical nodule. This case also highlights the importance of awareness of this entity, which can lead to an appropriate workup with noninvasive diagnostic techniques like estimation of serum PSA levels, and ultrasound studies, especially in an elderly male. Final confirmation in these cases may be obtained either by immunostaining for PSA and prostatic acid phosphatase [2],[3] or by obtaining a six-quadrant needle biopsy of the prostate, as in this case. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09032f1.jpg] [cr09032t2.jpg] [cr09032f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}