 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
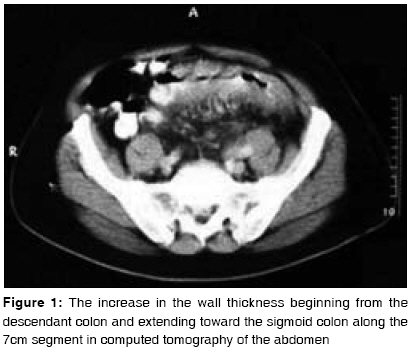
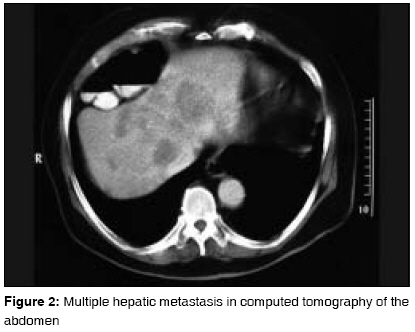
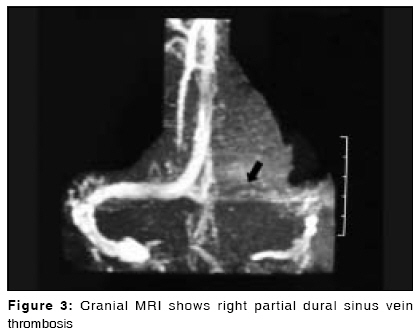
Journal of Cancer Research and Therapeutics, Vol. 5, No. 2, April-June, 2009, pp. 130-132 Case Report Dural sinus vein thrombosis in a patient with colon cancer treated with FOLFIRI/bevacizumab Ozen Alaattin, Cicin Irfan, Sezer Atakan, Uzunoglu Sernaz, Saynak Mert, Genchellac Hakan, Karagol Hakan Department of Medical Oncology, Faculty of Medicine, Trakya University, Edirne Code Number: cr09033 DOI: 10.4103/0973-1482.52791 Abstract The adverse effects of regimes in cancer treatment have forced us to change to new targeted therapy options. Understanding these side effects, which can lead to discontinuation of the new therapy strategies, will allow the clinical management of these side effects and result in continuing therapies with effective medications. Bevacizumab, which is an IgG1 antibody against vascular endothelial growth factor, has side effects such as proteinuria, hypertension, venous and arterial thromboembolic events, and hemorrhage. This is the first reported case of dural sinus vein thrombosis, during the treatment with bevacizumab. Keywords: Bevacizumab, dural sinus vein, thrombosis Introduction The treatment options in patients with advanced colon cancer have been increasingly developing. The targeted therapies, such as bevacizumab, cetuximab, and panitumumab, have become the main constituents of the current therapy for the advanced colon cancer. [1] With these new therapy options, side effects have also changed. Bevacizumab, a monoclonal antibody against vascular endothelial growth factor (VEGF), causes side effects such as perforation in the gastrointestinal system, hemorrhage, arterial-venous thromboembolic events, hypertension, and proteinuria. [2] Understanding these side effects, which can lead to discontinuation of the new therapy strategies, will allow the clinical management of these side effects and will result in continuing therapies with effective medications. In addition, overcoming the life-threatening events will become possible. In this paper, a case of dural sinus vein thrombosis (DSVT), arising due to the use of bevacizumab, which has not been reported previously in the literature is presented.Case Report A 64-year-old male patient suffering from rectal hemorrhage was admitted to our hospital in January 2007. A mass was detected. Biopsy was taken in a rectoscopic examination at 20 th cm of the rectum. The lesion was diagnosed as adenocarcinoma. An abdominal computed tomography (CT) scan revealed multiple metastatic lesions in the liver and wall thickening in the sigmoid colon [Figure - 1] and [Figure - 2]. No metastasis was observed by CT of the thorax. Laboratory tests were significant only for carcinoembryonic antigen (CEA) (347 ng/ml; range: 0.52-6.3 ng/ml). The patient received the FOLFOX4 regimen. A partial response was detected by abdominal CT, and CEA was found to be 119 ng/ml. After the 11 th cycle of FOLFOX4 therapy, bowel obstruction was observed. CEA was found to be 203 ng/ml, and progressive disease was detected by abdominal CT. Sigmoid colon resection was performed. The patient began bimonthly chemotherapy of the FOLFIRI/bevacizumab regimen following the recovery of the postoperative wound, which consisted of 5 mg/kg of bevacizumab and 125 mg/m 2 of irinotecan on day 1, in addition to a bolus of 200 mg/m 2 of leucovorin and 400 mg/m 2 of 5-FU, followed by a 22-h continual infusion of 600 mg/m 2 of 5-FU on days 1 and 2. The patient was admitted to the emergency service in a state of unconsciousness with seizures after the third cycle of the FOLFIRI/bevacizumab regimen. By cranial magnetic resonance imaging, global atrophy and partial DSVT were revealed [Figure - 3]. The patient had no additional pathology and clinical/metabolic reason which would have led to DSVT, except malignancy and combined chemotherapy including bevacizumab. Chemotherapy was interrupted and anticoagulant therapy was begun. An apparent clinical recovery was observed. The patient, after refusing other therapy options, died of progressive colon cancer in March 2008.Discussion Many studies indicate that progression-free survival and overall survival have improved by adding bevacizumab to various chemotherapy regimens for patients with metastatic colon cancer. [3],[4] VEGF is a glycoprotein molecule stimulating specific blood vessel formation and having a role in tumor growth and dissemination through VEGF receptors on the surface of the endothelial cells. Bevacizumab inhibits VEGF activity by binding VEGF receptors, and therefore, it prevents tumor growth and metastasis by inhibiting endothelial cell proliferation and angiogenesis. In addition to its direct antiangiogenic effects, bevacizumab may also improve the delivery of chemotherapy by altering tumor vasculature and decreasing the elevated interstitial pressure in tumors. [5] The side effects related to bevacizumab are proteinuria (38%), hypertension (34%), venous thromboembolic events (17%), arterial thromboembolic events (4%), congestive heart failure (4%), hemorrhage (3-4%), perforation in the gastrointestinal tract (2%), and reversible posterior leucoencephmalopathy syndrome (< 1%). [2] In a study in which bolus IFL (irinotecan, 5-flourouracil, and leucoverin) plus bevacizumab and bolus IFL and placebo were compared, thromboembolic events were seen in higher rates in the patients who received ILF plus bevacizumab (9% versus 26%). [4] Kuenen et al . reported the effect of VEGF inhibitor on the coagulation system and vascular wall after therapy in 17 patients diagnosed with various malignancies. This report demonstrated a significant increase in some parameters such as the von-Willebrand factor, E-selectin, tissue factor, and endogenous thrombin potential representing the increased vascular endothelial activation and coagulation potential of VEGF receptors. [6] Kilickap et al . reported that VEGF receptor inhibition increases endothelial cell dysfunction and subendothelial collagen exposure and that subendothelial collagen exposure may activate the tissue factor. [7] All of these reports indicate that VEGF is a regulating factor for endothelial cells and that the inhibition of VEGF receptors may increase the risk of thromboembolism. DSVT is a severe complication that can be seen in cancer disease. Hypercoagulability syndromes, systemic inflammatory diseases, oral contraceptives and other drugs, malignancy, malnutrition, severe dehydration, surgical intervention, trauma, severe systemic diseases, or local infections are the main causes. [8],[9],[10] The most affected dural sinuses are the superior sagittal sinus, transverse and sigmoid sinus, cavernous sinus, and sinus rectus. Half of the cases of DSVT demonstrate a subacute initiation. DSVT may exhibit clinical conditions such as headache, papilla edema, and isolated intracranial pressure increase syndrome accompanying the sixth cranial nerve involvement; focal deficit and/or epileptic seizures; or subacute encephalopathy, during which consciousness is disrupted sometimes accompanied by seizures. Anticoagulants and antiepileptic and symptomatic therapies are the basic treatment options, and thrombolytic therapy is another alternative in selected cases. [9],[10] During the 11 cycles of the FOLFOX4 therapy, no thromboembolic event was seen in our patient. In the recent therapy of FOLFIRI/bevacizumab, there was no risk factor, except chemotherapy and malignancy. Additional local or systemic disease, cerebral metastasis, and metabolic reasons that could explain the condition of the patient in a state of unconsciousness, with seizures could not be detected. The incidence of DSVT in colorectal cancer patients is unknown, but it is not common. These findings suggested that DSVT causing seizures and unconsciousness may be related to bevacizumab. Therefore, DSVT should be considered in a differential diagnosis besides cerebral metastasis and metabolic disorders in which unconsciousness and seizures develop in cancer patients using bevacizumab. We could not find any DSVT case in patients treated with bevacizumab in the literature. In addition, we have not a specific explanation for DSVT related to bevacizumab. In order to clarify this issue, reporting these cases will provide additional contributions to identifying the probable relationship. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09033f1.jpg] [cr09033f3.jpg] [cr09033f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}