 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
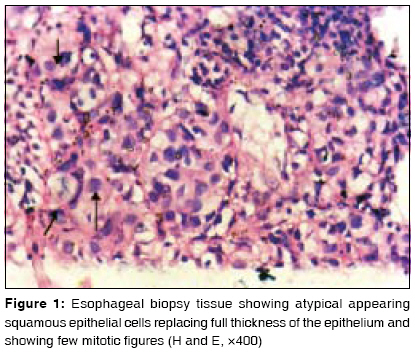
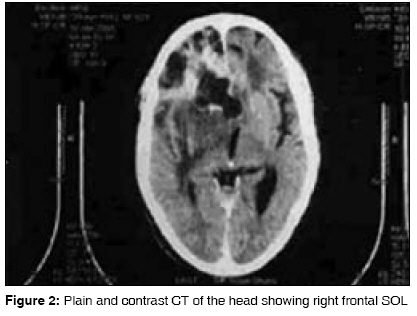
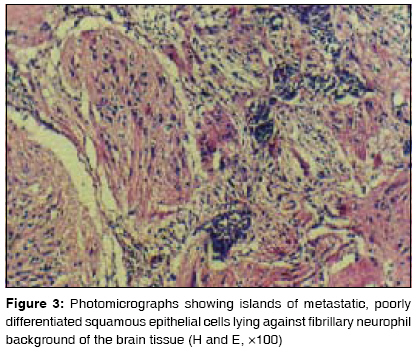
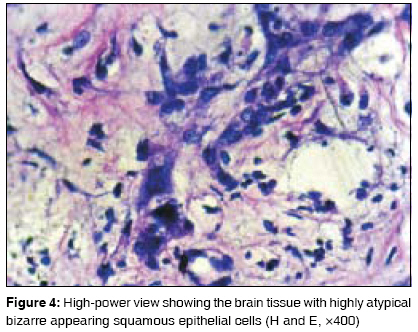
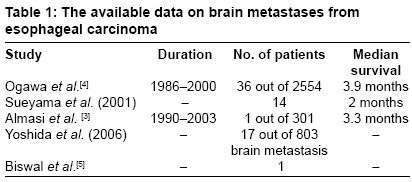
Journal of Cancer Research and Therapeutics, Vol. 5, No. 2, April-June, 2009, pp. 137-139 Case Report Brain metastasis from esophageal carcinoma Agrawal Rashi, Shukla Prity, Shukla Vikas, Chauhan Arvind J K Cancer Institute, Kanpur, Uttar Pradesh Code Number: cr09035 DOI: 10.4103/0973-1482.52785 Abstract Esophageal carcinoma rarely metastasizes to brain. In our center, among 504 cases of esophageal cancer registered for treatment during a 15-year (1990-2005) period, brain metastasis from esophageal carcinoma was detected in only 1 case. An unusual case of esophageal carcinoma that presented with brain metastasis is reported here.Keywords: Brain metastasis, carcinoma esophagus, spread Introduction Metastatic spread to the central nervous system is a relatively common occurrence in patients with systemic cancer. Esophageal carcinoma commonly metastasizes to lung, pleura, liver, stomach, peritoneum, kidney, adrenals, and bone but it rarely metastasizes to brain as evidenced by very small number of clinical series and published case reports. [1] Recently, advances in neuroimaging and the increased survival of these patients have led to more frequent and earlier detection of brain metastasis.Case Report A 60-year-old male presented with progressive dysphagia for 1 year in September 2002. He was diagnosed as a case of middle third esophageal carcinoma. Pathologic study of an endoscope-guided biopsy revealed that histology was squamous cell carcinoma [Figure - 1]. He then received three cycles of platinum-compound-based neoadjuvant chemotherapy at 3-week intervals followed by external radiotherapy. External radiotherapy to anterior and posterior aspects of mediastinum was given. A tumor dose of 6000 cGy in 30 fractions was delivered by cobalt machine. Endoscopy done 6 weeks after completion of treatment showed no evidence of disease. Patient remained asymptomatic for the next two and half years. The patient complained of severe and progressively increasing headache in April 2005, approximately two and half years after the diagnosis of esophageal cancer was made. On admission, he was in altered sensorium after one episode of seizure. On systemic examination, no other organ involvement (lung, liver, and bones) was found. Ultrasound (whole abdomen), an X-ray of the chest, complete blood count, liver function test including serum alkaline phosphatase, and kidney function test were within normal limits. Plain and contrast CT scan of the head showed right frontal heterogeneous space-occupying lesion predominantly cystic, solid, measuring 7 x 5 x 5 cm with perifocal edema causing compression of the ipsilateral ventricle and genu of corpus callosum [Figure - 2]. Right frontal craniotomy with decompression of SOL was done. Histopathological examination showed islands of metastatic, poorly differentiated squamous epithelial cells lying against fibrillary neurofibril background of the brain tissue [[Figure - 3]- H and E, X 100, [Figure - 4] - H and E, X 400]. On comparison, the original esophageal biopsy tissue [Figure - 2] was consistent with the metastatic, poorly differentiated esophageal squamous cell carcinoma. After surgery, patient′s general condition slightly improved. Postoperative radiotherapy was advised but attendants of the patient were reluctant to it. Afterwards, the patient came for follow-up after 5 months; his general condition was deteriorating and he expired after 22 days. Discussion The overall incidence of brain metastasis from various malignant tumors can vary from 13.5 to 37% often as adenocarcinoma or squamous cell carcinoma, 31 and 9%, respectively. In lung carcinoma, the frequency of brain metastasis was 4.8% in adenocarcinoma and 2.5 % in squamous cell carcinoma patients at the time of the diagnosis. Distant metastases from esophageal carcinoma were most commonly diagnosed in lymph nodes (45%) followed by liver (35%), lung (20%), cervical/supraclavicular lymph nodes (18%), bone (10%), adrenal (5%), and peritoneum (2%) [2] whereas the incidence of brain metastasis was only 1.5%. [3] Lassman and Angelis reviewed nine studies and found that the highest numbers of cases developing brain metastasis from gastrointestinal malignancies were of colorectal carcinoma (2-12%). Available data on brain metastasis from carcinoma esophagus are showed in [Table - 1]. Metastatic spread to the brain through blood circulation occurs mostly via arterial circulation. The most common histology in both primary tumor and brain metastasis was adenocarcinoma in the United States, while the most common histology in our country is squamous cell carcinoma. A CT scan of the chest and abdomen should be done for the initial evaluation of the disease. Recent studies have shown that the addition of PET to standard staging studies can improve the accuracy of detecting stage IV disease by 18%, upstage patients by 15%, and downstage patients by 7%. [6] Intracranial metastases and primary high-grade gliomas can be differentiated by using conventional magnetic resonance (MR) imaging and clinical history. Most metastases are round, well-demarcated lesions located at the junction of gray and white matter and have mass effect. Leakage from tumor vessels results in an extensive zone of edema surrounding the tumor. A total of 80% are located in the arterial distribution zones of the cerebral hemisphere while extensive glioblastomas most commonly have much more irregular lobulated configurations and greater heterogeneity of density on contrast-enhanced images. [7] Perfusion-weighted and proton spectroscopic MR can be used to differentiate high-grade primary gliomas and solitary metastases on the basis of differences in vascularity and metabolite levels in peritumoral regions. [8] Immunohistochemistry using antineuron-specific nuclear protein, antivimentin, and antiepithelial membrane antigen would help to differentiate between primary and secondary tumors. In secondary brain tumors with unknown primary tumor, by cautious use of immunohistochemistry we can search for primary tumor. Metastatic brain tumor from melanoma will have HMB- 45 antigen, prostate PSAP, thyroid thyroglobulin, and so on. In general, surgical excision is done in cases with a solitary lesion or adjacent multiple metastasis, cases with diagnostic uncertainty, or cases with life-threatening and critically located metastases. Patients with nonadjacent, multiple, or inoperable lesions are usually treated with palliative whole brain radiotherapy. Surgical excision of solitary/single lesion combined with adjuvant whole brain radiotherapy yields a better survival than radiotherapy alone. The rationale of adjuvant whole brain radiotherapy is to sterilize the tumor bed which contains microscopic foci. Patchell et al. reported significantly better survival (70% vs. 18%, P < 0.001) and an improved quality of life without any overall survival benefit. [9] With variable success, stereotactic radiosurgery provides a substitute to conventional surgery. Most of the reports have indicated that esophageal cancer patients who developed brain metastasis, in general, have poor prognosis (median survival ranged from 3.6 to 3.9 months). [10] References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09035f2.jpg] [cr09035f1.jpg] [cr09035f3.jpg] [cr09035t1.jpg] [cr09035f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}