 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
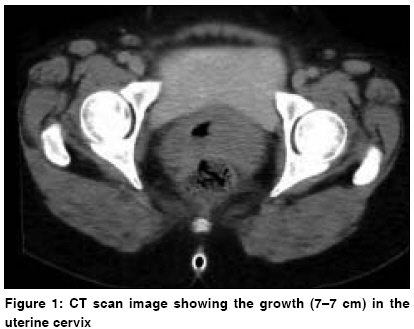
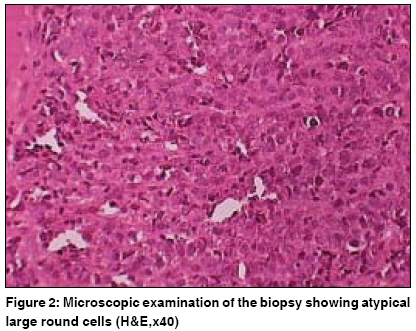
Journal of Cancer Research and Therapeutics, Vol. 5, No. 2, April-June, 2009, pp. 140-142 Case Report Diffuse large B-cell lymphoma of the uterine cervix: A rare case managed novelly Baijal Gunjan, Vadiraja BM, Fernandes DonaldJ, Vidyasagar MS Department of Radiotherapy and Oncology, Shirdi Sai Baba Cancer Hospital, Kasturba Medical College, Manipal, Udupi, Karnataka Code Number: cr09036 DOI: 10.4103/0973-1482.52784 Abstract Non-Hodgkin's lymphoma (NHL) of the uterine cervix is exceedingly rare. The management of the disease is not standardized. A 44-year-old lady presented with a history of bleeding pervaginum and a foul-smelling discharge of 2 months' duration. A 7 x 7 growth was seen in the cervix. A biopsy revealed it to be a CD20-positive diffuse large B-cell (DLBCL)-type NHL. She was diagnosed as stage IE after staging work-up, and managed with three courses of rituximab, cyclophosphamide, vincristine, adriamycin, and prednisolone followed by external beam radiotherapy (46 Gy in 23 fractions) by 3D conformal technique. She attained a complete response, and has been in remission for 1 year 3 months. Keywords: Non-Hodgkin′s lymphoma, rituximab, uterine cervix Introduction Non-Hodgkin′s lymphoma (NHL) affects the extranodal regions in about one-third of patients. NHL of the cervix affects only about 1 in 730 cases of non-Hodgkin′s lymphoma or 1 in 175 cases of extranodal lymphomas. [1] A review of the literature corroborates the rarity of the disease as not many cases are reported and are mostly in the form of case reports and small case series. The confusion is heightened by the fact that the management of this disease is not well defined in the literature. Even though the role of chemotherapy in conjunction with radiotherapy/surgery seems to be standard, the role of monoclonal antibodies like rituximab has not been well elucidated in the literature. Thus, we wish to report a case of a rare disease [diffuse large B-cell lymphoma (DLBCL) of the uterine cervix] managed novelly with CHOP-rituximab followed by consolidation radiotherapy. Case Report A 44-year-old noncomorbid perimenopausal lady presented to us with a history of bleeding pervaginum and a foul-smelling discharge of 2 months′ duration for which she was treated with antifungals elsewhere. An examination revealed a growth in the cervix 7 x 7 cm in dimension [Figure - 1]. The parametrium was not indurated and the rectal mucosa seemed uninvolved. There was no lymphadenopathy/hepatosplenomegaly, and the chest was clear. A biopsy from the growth was reported as a DLBC-type NHL (verified at two centers). The specimen showed diffuse infiltration by atypical large round cells with minimal intervening stroma. The cells had high N/C ratio, oval nuclei, and clumped chromatin [Figure - 2]. The immunohistochemistry revealed the tumor to be positive for LCA and CD20 [Figure - 3] and negative for pan cytokeratin and CD3. Staging work-up with CT scan, routine blood, bone marrow aspirate, and biopsy was negative. In view of the above findings, the diagnosis of primary NHL (DLBCL) of the uterine cervix (stage IE) was established. The patient was planned for three courses of CHOP-R (cyclophosphamide, adriamycin, vincristine, prednisolone, and rituximab) chemotherapy followed by 46 Gy of radiation therapy to the pelvis with 3D conformal radiation therapy on a linear accelerator as 200 cGy per fraction. After three courses of chemotherapy, patient had a partial clinical response to therapy and was planned for radiation therapy as stated above. At the end of the radiation, patient had a complete clinical response. She was reassessed with CT of the abdomen and the pelvis at the end of 3 months of treatment. The CT scan showed a complete response [Figure - 4]. She has been in remission for 1 year 3 months posttreatment now. She had one episode of grade 3 myelosuppression during chemotherapy and grade 2 acute proctitis during radiation which resolved with conservative management. No late sequelae of treatment have been observed in the patient. Discussion The incidence of NHL is about 19.9 per 100,000 population. [2] Primary malignant lymphoma of the uterine cervix and upper vagina is an extremely rare tumor of the female genital tract. Median age of the patients affected by this neoplasm is 40 years. Clinical symptoms usually include vaginal bleeding (70%), perineal discomfort (40%), and persistent vaginal discharge (20%). [3] Papanicolaou smear has a limited diagnostic value because of the usual lack of surface cervical ulceration. [4] The majority of NHLs arising from the uterine cervix is represented by high-grade lymphomas with large B-cell histotype. [3] Our case presented in the correct decade and had corroborative symptoms, and in view of the rarity of diagnosis was subjected to biopsy and then slide review (verified at two centers) and immunohistochemistry to obtain the diagnosis. The adequate treatment of this malignancy has never been standardized. This tumor has been managed with chemotherapy and surgery demonstrating a long disease-free follow-up of up to 10 years for individual patients. In these reports, six cycles of CHOP chemotherapy followed by surgery or vice versa were used. [3],[4],[5] The use of chemotherapy and radiation was done by Stroh et al . who reported 16 cases of lymphomas of the cervix of which 12 had received radiation. In their series, 90% of patients with low risk factors were disease-free at 5 years. They concluded that combined modality treatment with CHOP-based chemotherapy and moderate doses of radiation was the best treatment for NHL of the cervix. [6] Recently Heredia et al . reported two cases of DLBCLs of the cervix treated with three courses of CHOP and involved field radiotherapy. Both patients were disease-free at 5 years and 15 months. [7] Rituximab is a novel monoclonal antibody against CD20 found to be active in NHL. Its use in DLBCL was validated by the GELA trial which showed that addition of rituximab to CHOP improved the overall survival in these patients. [8] The use of rituximab-CHOP has been reported once in an HIV-positive patient with HAART in context of DLBCL of the cervix. The patient was alive at 38 months of follow-up. [9] In another report, Chi Feng-Su et al . reported the use of rituximab with cyclophosphamide, vincristine, and prednisolone following surgery in a single patient who remained disease free after 3 years. Radiation was not used in either of these patients. [10] For early-stage aggressive NHL, the standard therapy is three courses CHOP followed by IFRT. Compared to CHOP alone, this resulted in a better progression-free and overall survival (77% vs. 64% and 82% vs. 72%). [11] However, the survival advantage was lost with the longer follow-up. Recently, the SWOG reported a trial of combining rituximab-CHOP (three courses) with radiation. Their results reveal that addition of rituximab may improve the progression-free survival (95% vs. 85% at 2 years compared to historical cohorts of SWOG 8736). [12] It is also known that prognosis of extranodal lymphomas is same as that of nodal lymphomas when all the prognostic variables are matched. Thus in view of the literary evidence, we chose to manage our patient with abbreviated CHOP-rituximab and consolidation RT eventually achieving a complete response. Conclusion We conclude that abbreviated CHOP-rituximab with consolidation RT maybe an effective treatment for patients with NHL and deserves attention in the setting of extranodal lymphomas.References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09036f4.jpg] [cr09036f3.jpg] [cr09036f2.jpg] [cr09036f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}