 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
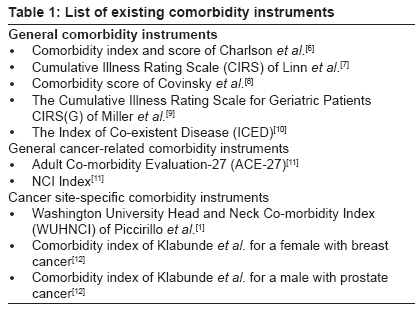
Journal of Cancer Research and Therapeutics, Vol. 5, No. 3, July-September, 2009, pp. 145-147 Editorial Significance and prognostic impact of co-morbidity in head and neck cancer Kazi Rehan, Nutting ChrisM, Rhys-Evans Peter, Harrington KevinJ Head and Neck Unit, Royal Marsden Hospital, London SW3 6JJ Code Number: cr09039 PMID: 19841553 DOI: 10.4103/0973-1482.57117 Introduction In medicine, comorbidity literally means any distinct additional disorder/disease that has existed or that may occur during the clinical course of a patient who has the index disease under study. It describes the sum of the effects of all other diseases from which an individual patient may suffer, other than the primary disease of interest. [1],[2],[3],[4] We already know that with advancing age, there is an increased vulnerability to cancer. However, old age brings with it a host of other related chronic health problems such as heart disease, diabetes, chronic obstructive pulmonary disease, hypertension, and peripheral and cerebrovascular disease. [5] The presence of cancer along with pre-existing health problems raises very important issues for the oncologist in regard to clinical decision making and treatment. The evaluation of the impact of the burden of these comorbidities in every newly diagnosed cancer patient is crucial to providing quality cancer care. Comorbidity has a direct and consequential impact on the management and, ultimately, the survival of cancer patients. This is especially true in patients with head and neck cancer who often suffer from significant tobacco- and alcohol-related diseases. [2],[3] In this situation, an appropriate and a meticulous assessment of the comorbidity burden can significantly improve the decision-making process for clinicians and may influence patient outcomes. Comorbidity Assessment An accurate assessment of the comorbidity burden (i.e., medical, surgical, physical, social, and physiologic problems) of the head and neck cancer patient, in addition to the customary time-honored classification of tumor characteristics (i.e., tumor-node-metastasis staging), can provide valuable prognostic information. [1],[2],[3] This information can be derived from a number of sources, such as a review of patients′ medical records, personal interviews, a review of discharge data, death certificates, and most importantly comorbidity indices. [5] Several comorbidity indices derived from the presence of selected conditions-assigned severity scores offer varying assistance in comorbidity assessment. These indices approach the relationship between and among conditions in diverse, but with a common goal of deriving a single comorbidity score. However, whilst they appear simple to use, the collection of accurate, valid, and meaningful comorbidity data requires formal training. A thorough understanding of the comorbid diseases and terminologies is crucial to avoid ambiguities in data collection. A wide variety of comorbidity scales are available in the literature and it is imperative to use one that is appropriate, valid, and reliable. General comorbidity instruments are intended to be used across a broad range of clinical conditions whilst, disease-specific comorbidity instruments are intended for a specific disease/condition [Table - 1]. Several researchers have compared and studied the suitability of the general indices in head and neck cancer patients with good results, despite their apparent lack of specificity. Piccirillo et al. developed the only head and neck cancer-specific commercial index available to date called the WUHNCI (Washington University Head and Neck Co-morbidity Index). [1],[2],[3] The scale is based on a modified version of the Kaplan-Feinstein index. The WUHNCI identifies seven important prognostic comorbidities that include congestive heart failure, cardiac arrhythmia, peripheral vascular disease, pulmonary disease, renal disease, previous history of cancer now controlled, and previous history of cancer now uncontrolled. The index can be consulted at http://oto.wustl.edu/clinepi. It has a strong development process and has proven its validity in a number of retrospective and prospective studies across the globe. However, as with any index, there is a learning curve that is crucial to obtaining meaningful and valid data. Comorbidity Impact Comorbidity has a direct consequential impact on the management and, ultimately, the survival of cancer patients. [1],[2],[3] The presence of comorbid conditions has a significant impact on tumor- and treatment-specific outcomes. The prognostic importance of comorbidity on survival has been shown for patients with a variety of cancers, such as those of the oral cavity, oropharynx, nasopharynx, larynx, lung, breast, rectum, and cervix, and leukemia. [13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23] Comorbid conditions can often interact with the primary cancer to create a more lethal situation than that caused by the primary cancer alone. In some cases, the outcomes for patients who survive the initial period after diagnosis and treatment may be more dependent on their comorbidities than their cancers. [1] This impact of comorbidity on survival has been shown to be significant even after controlling for other important factors such as age, sex, race, site of cancer, and tumor stage. [1],[2] The inclusion of comorbidity information along with tumor mapping at local and national levels can significantly improve the value of cancer statistics and the management of head and neck cancer patients. [1],[2],[3],[13],[14],[15],[16],[17],[18],[19] Researchers have shown conclusively that comorbidity is an important prognostic attribute of cancer. Comorbid conditions could be simply classified as mild, moderate, or severe. [1],[2],[3] For example, a disease such as hypertension would be considered to be mild, whilst myocardial infarction would be considered to be severe. The incidence of comorbidity in head and neck cancer patients ranges from 3% to almost 40% in various studies of which the most commonly noticed comorbid conditions are hypertension and COPD. Based on their impact, comorbid conditions can be further classified into "prognostic" based on their effect on survival (e.g., myocardial infarction) or "therapeutic" based on their influence on treatment options (e.g., COPD in laryngeal cancer treatment). [1],[2],[3] Although the presence of advanced comorbid conditions in head and neck cancer patients is not associated with an increase in the rate of treatment-associated complications, they tend to be more severe in this population. [1],[2] Vascular disease and COPD are widely accepted as poor prognostic conditions for surgical management. For chemo-radiotherapy, conditions like diabetes and hypertension increase the risk of late radiation complications, and renal disease may affect the ability to deliver effective induction or concomitant chemotherapy. More importantly, advanced comorbidity has a negative effect on disease-free interval and tumor-specific survival in patients with head and neck cancer, independent of other factors. This suggests that comorbidity may impact on tumor behavior, presumably by altering the host′s response to cancer. The prognostic impact of comorbidity is believed to be a result of the physiological burden of chronic disease and its treatment. Despite evidence to the contrary, when reporting statistical survival data, local and national cancer registries do not routinely take into account the available comorbidity data. This is primarily due to the fact that the current TNM system of cancer classification is based primarily on the morphological spread of cancer and does not consider important host factors, such as comorbidity. [24] Use of the TNM system alone to compare outcomes for patients receiving different treatments is inadequate and incomplete. The addition of vital comorbidity data to the TNM cancer staging system may permit a more reliable and valid assessment of survival. [2],[3],[24] This is indeed an important shortcoming of the current staging system for head and neck cancer and may benefit from revision. The widespread use of validated comorbidity scales in outcomes research, with a solid conceptual and scientific base, can provide meaningful clinical yield to assure quality cancer care for head and neck cancer patients. The presence of multiple comorbid conditions in a cancer patient requires focussed monitoring. Due attention to the cumulative effects of the diseases, fluctuating nutritional status, disease clustering, and various interactions between the cancer and its treatment must be taken into account. All efforts must be directed into integrating reliable and valid comorbidity instruments into oncology practice. The continued exclusion of prognostic comorbidity data from clinical research and staging can no longer be justified. Further site- and treatment-specific longitudinal prospective studies are warranted to better define the prognostic role of comorbidity in head and neck cancers. [1],[2],[3] In the words of one of the pioneers in this field, Dr. Jay Piccirillo, "The cancer community can no longer continue to ignore the obvious prognostic importance of these factors. The continued focus on the description of the tumour while ignoring suitable descriptions of the cancer patient weakens the scientific accuracy of the cancer staging system and ultimately the humanistic care of patients." [3] References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09039t1.jpg] |
| |||||||||

{kind=link}