 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
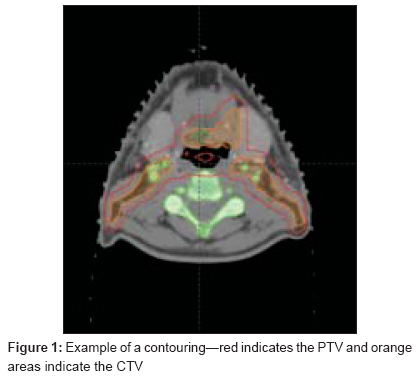
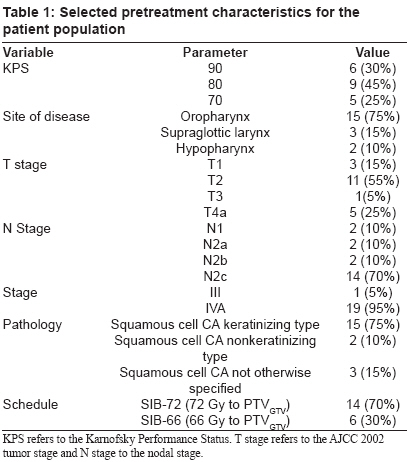
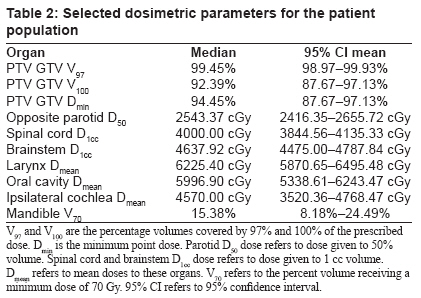
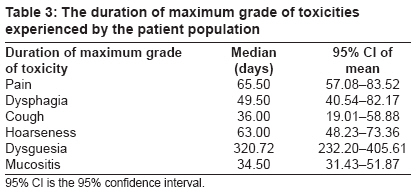
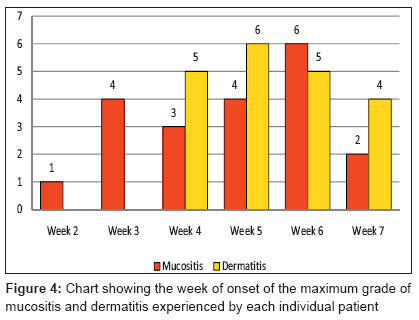
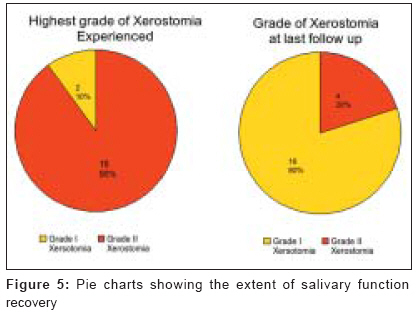
Journal of Cancer Research and Therapeutics, Vol. 5, No. 3, July-September, 2009, pp. 165-172 Original Article Preliminary results of SIB-IMRT in head and neck cancers: Report from a regional cancer center in northern India Chakraborty Santam, Ghoshal Sushmita, Patil VijayM, Oinam ArunS, Sharma SureshC Department of Radiotherapy and Oncology, Regional Cancer Center, PGIMER, Chandigarh, Chandigarh UT Code Number: cr09043 PMID: 19841557 DOI: 10.4103/0973-1482.57121 Abstract Background : Intensity-modulated radiotherapy using simultaneous integrated boost (SIB-IMRT) is an attractive method for the treatment of head and neck cancers with sparing of the salivary function.Aims : To assess the feasibility, toxicity, and tumor control using SIB-IMRT in locally advanced head and neck cancers in the Indian setting. Settings and Design : The study was conducted in a regional cancer center in northern India. A review of the treatment result of the first 20 patients is presented. Methods and Materials : SIB-IMRT was planned for 20 patients-14 patients were treated with the SIB-72 schedule delivering a dose of 72 Gy, 66 Gy, and 57 Gy to the PTV GTV , PTV CTV1 , and PTV CTV2 in 33 fractions. Six patients were treated with the SIB-66 schedule delivering 66 Gy, 60 Gy, and 54 Gy to the above-mentioned volumes in 30 fractions. Patients were monitored for toxicity using the CTCAE v 3.0 criteria. Descriptive analysis of toxicity and actuarial estimates of the loco-regional control and survival are presented. Results : Grade III mucositis was seen in 65% patients. None of the patients had Grade III dermatitis. The projected 2-year overall survival was 95%. Conclusion : SIB-IMRT schedules evaluated were found to be safe and effective and are being subjected to further prospective studies. Keywords: Dose painting IMRT, head and neck cancer, intensity-modulated radiotherapy, parotid, simultaneous integrated boost, salivary sparing Introduction Cancers of the head and neck are one of the most common types of cancer in India, accounting for 20% of all cancers in males in some of the Indian cancer registries. [1],[2] Treatment of these cancers involves the use of radiation therapy in most of the patients at one point of the time or other. Intensity-modulated radiotherapy (IMRT) offers several advantages in the treatment of head and neck cancer notable amongst which are the ability to conform the high-dose region accurately to the target volume with the best sparing of critical structures. In addition, the treating oncologist has the ability to selectively increase the dose per fraction to selected subvolumes of the target where more radioresistant clones are anticipated to be present-an approach known as dose painting IMRT or simultaneous integrated boost IMRT (SIB-IMRT). [3] The conformity however comes with a price that the treatment is invariably longer and requires a greater degree of accuracy for its proper execution. In addition, the multiple beams chosen often lead to unwanted dose deposition in the anteriorly placed critical structures like the larynx and oral cavity which can lead to unanticipated toxicities. [4],[5] The tangential nature of entry of beams can lead to excess dose deposition in the skin with an attendant increase in actinic complications also. [6] As with any new technology, the question of a learning curve exists and this is more in conformal techniques like IMRT where one has to rethink and relearn the entire paradigm of treatment. It has been noted that in several institutions, in the initial implementation phase of conformal techniques, there has been an increase in acute and late toxicity due to aggressive target delineation. [7],[8] In this respect, we decided to analyze the data of the first 20 patients treated with IMRT in our institution with regard to toxicities encountered and the control achieved. Materials and Methods Between January 2005 and March 2007, 20 patients with head and neck cancers were treated with external beam radiation therapy using two simultaneous integrated boost IMRT (SIB-IMRT) schedules in our institute. Patients were considered eligible, if they had pathologically confirmed squamous cell carcinomas of the oropharynx, supraglottic larynx, and hypopharynx. The selection criteria used included age > 20 years, clinical stages III-IVA, Karnofsky Performance Status (KPS) of ≥ 70, and absence of serious uncontrolled comorbidities. All patients signed a written informed consent prior to participation in the study. Ethical clearance for the conduction of the study was obtained from the institutional ethics committee prior to the inception of the study. Baseline workup included a chest x-ray, complete hemogram, and assessment of kidney and liver function tests within 2 weeks of starting treatment. Patients were treated in the supine position with a custom-made thermoplastic cast (Efficast; -five-point head and neck precut with profiles-Orfit Industries) which covered the head and neck region. A customized bite block was prepared and attached to the thermoplastic cast in all dentulous patients. All patients had a contrast-enhanced CT scan of the neck from the base of the skull to the thoracic inlet following injection of 50-60 ml of nonionic contrast after a separate written informed consent. A helical scan with 2.5 mm slice thickness was taken at 120 KVp and 250-300 mA, while wearing the custom-made thermoplastic mask with the fiducial markers. CT scans acquired were pushed to the Eclipse; Treatment Planning System (7.3.10) through the local area network, VARIS; . Target volume delineation [Figure - 1] was done on the contrast CT scan slices and for each patient, three target volumes with their respective planning target volumes were defined as per ICRU 62 [9] guidelines. GTV (gross tumor volume) included all clinically and radiologically demonstrable tumors including the involved nodes. Positive lymph nodes were defined as any lymph nodes ≥ 1 cm or nodes with a necrotic center. Two CTVs were defined, CTV1 which encompassed the areas considered to be at high risk of subclinical disease extension including the nodal basins considered to be at high risk of harboring metastatic disease. CTV 2 included the nodal drainage areas considered to be at low risk for having nodal involvement. Margins of 1.5-2 cm from the GTV were taken to arrive at CTV1 which was subsequently edited manually to conform to natural boundaries to spread. Contours of the GTV, CTV1, and CTV2 were expanded isotropically by 5 mm to generate their respective planning target volumes (PTV GTV , PTV CTV1 , and PTV CTV2 respectively). The PTVs were cropped so that they were restricted to 5 mm below the contoured body surface except in areas where the skin was considered to be a part of the CTV. In the latter situations, a customized wax build-up bolus of a suitable thickness was placed over the thermoplastic cast over the area outlined so that the PTV could extend outside the skin. In addition, the PTV receiving lower dose was cropped from the overlapping higher dose PTV to facilitate optimization. A set of organs at risk (OARs) was delineated for each patient which included spinal cord, brainstem, brain, contralateral parotid, larynx, inferior constrictor, and the oral cavity. The contours of the spinal cord and brainstem were expanded isotropically by 5 mm to arrive at the respective planning organ at risk volumes (PORVs). No PORVs were delineated for the parotid glands. Oral cavity was defined to include the buccal mucosa and the portion of the oral cavity outside the planning target volume. However, for the purposes of this study, the dose volume reporting for the oral cavity was done after contouring the entire oral cavity from the hard palate to the floor of the mouth as a single solid structure. Larynx was contoured from the tip of the epiglottis to the lower border of the cricoid cartilage. The constrictor muscles were contoured as a single structure from the level of the first cervical vertebrae to the level of the lower border of the cricoid cartilage around the pharynx using a 3-mm brush. IMRT planning was done using seven photon beams (6 MV) coplanar at intervals of 51. Plan optimization was done by inverse planning technique using Helios, IMRT software, with the help of the DVO algorithm, version 7.3.10. Sliding leaf movement technique was used for the delivery of IMRT. Two schedules of SIB-IMRT were used-SIB-72 and SIB-66. Patients in the SIB-72 schedule were planned so that a dose of 72 Gy, 66 Gy, and 57 Gy was delivered to the PTV GTV , PTV CTV1 , and PTV CTV2 respectively in 33 fractions (one fraction per day) over 45 days (6.5 weeks). In the SIB-66 schedule, patients were planned to a dose of 66 Gy, 60 Gy, and 54 Gy in 30 fractions (one fraction per day) over a planned course of 42 days (6 weeks). Patients were not treated on weekends and institutional holidays. No chemotherapy was given at any point of the treatment. Patients with disease involving the larynx/hypopharynx and those with a relatively poorer KPS (70) or more advanced age (> 60 years) were treated with the SIB-66 schedule in order to avoid the risk of long-term dysphagia. These selection criteria were prespecified in the protocol and the main emphasis was to ensure that chances of long-term dysphagia were minimized. Plans generated were reviewed using cumulative dose volume histograms [Figure - 2] and a slice-by-slice review of dose color wash displays. Plans were iteratively optimized till desired objectives were met prior to starting the treatment. Plans were deemed acceptable if 100% of the prescribed dose covered ≥ 95% of the respective PTVs and no more than 20% of the PTV received ≥ 107% of the prescribed dose. Overdose to areas of body outside the PTV was constrained so that dose to ≥ 5% volume did not exceed 105% of the prescribed dose. Quality assurance of all accepted plans included absolute dosimetry to check the absolute point dose at the isocenter and relative dosimetry to check the planar dose profile on a coronal plane perpendicular to the collimator axis of the gantry (gantry angle = 0) produced in a regular phantom at 5-cm depth due to modulated photon fluence from a linear accelerator in an isocentric setup. The absolute dosimetry was done using 0.6 cc farmer-type ionization chamber, PTW-Unidos; dosimeter (type of chamber: 30013) from PTW-Freiburg, Germany, and the relative dosimetry was done using film dosimetry with EDR-2; films in solid-water IMRT Phantom; (Scanditronix Wellhofer, Germany) with the help of Omni-Pro IMRT; software, version 1.5. Absolute dose variations within 2% were accepted for the treatment if the isocenter was defined inside the target and 3% elsewhere. All IMRT fields were delivered with dynamic multileaf collimation (40-pair MLC) on a Varian linear accelerator Clinac DHX (2300 CD)(Varian Medical Systems, Palo Alto, CA, USA). Electronic portal images were acquired in two orthogonal projections prior to treatment delivery. Subsequent electronic portal images were acquired on a biweekly basis and off-line corrections were done when setup error ≥ 3 mm was noted in any direction. Toxicities experienced by the patients during and after treatment were evaluated using the Common Terminology Criteria for Adverse Events version 3.0 (CTCAE v 3.0) system developed by the NCI. [10] Patients were asked to report on the subjective symptoms experienced using a questionnaire in the vernacular language. For the illiterate patients, grading was done by the radiation oncologists with good command over the vernacular language. No specialized questionnaire was used for detailing the salivary toxicity, and the CTCAE grading scheme was utilized for the assessment of salivary and other toxicities encountered. In this scheme, dryness of the mouth without a significant dietary alteration is graded as grade I xerostomia, severe and symptomatic dietary alterations (which include intake of copious water, other lubricants, or diet limited to purees and/or soft, moist foods) are graded as grade II, and symptoms leading to inability to adequately aliment orally graded as grade III toxicity. In addition, by quantitative assessment, an unstimulated salivary flow more than 0.2 ml per min is graded as grade I toxicity, 0.1-0.2 ml per min as grade II, and less than 0.1 ml per min as grade III toxicity. At the time of initiation of the protocol, quantitative salivary gland scintigraphy was not being performed at our institution; hence, the same was not included as a protocol requirement. Saliometry was not performed due to time-related constraints. Treatments were interrupted in the event of rapidly progressive toxicity or poor symptom control despite adequate medical treatment. The decision for stopping treatment was taken after review by the consultant radiation oncologists and after proper discussion and counselling of the patients. Response assessment was done at -4-6 weeks, clinically and radiologically as indicated. Follow-up of the patients was done at 2 weeks after completion of treatment and then every 2 months subsequently for 1 year. Further follow-up was done every 3 months for 1 year and 4 months subsequently. At each follow-up visit, a complete physical examination was combined with an assessment of the toxicity using the CTCAE system. Descriptive analysis for the variables is provided and 95% confidence intervals have been provided for continuous variables. As the study was not designed to answer questions regarding the superiority of one treatment schedule over the other, such analysis was not performed. Survival was analysed using the Kaplan-Meier method and the log rank test was used to calculate the difference between the major pretreatment variables. All statistical tests were performed using SPSS version 12.0 software. Results The first 20 consecutive patients treated with SIB-IMRT are analyzed. There were 16 males (80%) and four females (20%). The median age for the group was 58.5 years (95% CI of mean 51.26-61.74 years). Most of the patients were literate (n = 16; 80%). Eleven patients (55%) complained of local pain at the chief presenting complaint, while 6 (30%) complained of local foreign body sensation. The median duration of symptoms prior to diagnosis was 3.5 months (95% CI 2.9-9.3 months). A total of 13 patients (65%) gave a history of substance abuse, most commonly tobacco, while 6 patients (30%) had history of comorbidities, most commonly hypertension. The median beedi pack-years was 7 years prior to diagnosis. The median delay in the institution of radiation after diagnosis was 35.5 days. Other salient pretreatment characteristics are tabulated in [Table - 1]. All but one patient in the SIB-66 schedule had laryngopharyngeal primaries and the singular patient with oropharyngeal primary treated with the SIB-66 schedule had tumor extending into the hypopharynx and larynx. The median actual overall treatment time as calculated from the date of start of treatment to the date of end of treatment was 48 days (95% CI 47.33-51.56 days). The median delay in the completion of treatment over the planned treatment course was 2 days (95% CI 1- 4.7 days). Out of the 20 patients, 1 could not complete the planned course of treatment due to severe persistent pain associated with mucositis. This patient had her treatment stopped after 30 fractions had been delivered. A treatment gap was required in four patients, all of whom had grade III mucositis. All these patients were treated with the SIB A schedule. The mean gap duration for the patients who had been given a gap was 7 days (95% CI of mean 1-13.23 days). One patient each had required a gap in the second and third week of treatment respectively while two patients needed a gap in the sixth week of treatment. The median tumor volume was 30.49 cc (95% CI of mean 23.21-45.69) while the median nodal volume was 3.42 cc (95% CI of mean 3.10-7.96). [Table - 2] gives the some of the representative dosimetric parameters for the patient population in the study. During the treatment, the median weight loss was 2.72 kg and the mean weight lost was 2.89 kg (95% CI of mean 1.28-4.45 kg). Grade II or higher weight loss was seen in six (30%) patients. All patients had experienced some degree of pain during the course of treatment. The maximum grade of pain experienced was grade II in four patients (20%) and grade III in 16 (80%) patients. Pain was controlled with weak opiates in all but one patient who had treatment stopped due to pain. Amongst the other subjective symptoms grade II cough was seen in 7 (35%) patients and grade II or higher dysphagia was seen in 13 (65%) patients. All the patients had experienced grade II dysguesia during the treatment. Ryle′s tube feeding was needed in 3 (15%) patients and 16 (80%) patients needed oral nutritional supplementation during treatment. Grade II mucositis was seen in 6 (30%) patients while grade III mucositis was seen in 13 (65%) patients. One patient had only grade I mucositis during the course of treatment. Four (66.7%) in the SIB-66 schedule and nine (64.28%) patients in the SIB-72 schedule had grade III mucositis at any point of treatment. Grade II dermatitis was seen in 18 patients during the course of treatment. None of the patients had grade III dermatitis during treatment. The median duration of persistence of the maximum grade of subjective and objective toxicities is shown in [Table - 3]. As seen in [Figure - 3], majority of the patients had experienced their maximum grade of pain during the first 3 weeks of treatment. Similarly, maximum grade of cough experienced by the patients was mainly seen in the first 2 weeks of treatment. Most of the patients had complete loss of taste sensation at the end of the third week of their treatment. Five (25%) patients had their severest grade of mucositis by the third week of treatment only [Figure - 4]. Most of these patients had mucositis in the anterior aspects of the mouth in the oral cavity particularly in the region of the buccal mucosa. The anteriorly situated mucositis was seen in other patients also and often turned to confluent mucositis at the end of treatment. This mucositis was mostly located in the side where the tumor was located. It is also noteworthy that in several patients, there was no increase in the grade of mucositis in the later weeks of treatment. All patients had complete response at the end of treatment at both the local and nodal disease site. The median duration of local and nodal response at the time of analysis was 592.50 days (95% CI 537.89-689.00 days). The median follow-up for the population was 19 months (95% CI 17.24-22.15 months. One patient was lost to follow-up at the end of 3 months and could not be contacted any further. He was taken to have died of disease at the last documented follow-up date for the purpose of this analysis. All remaining 19 (95%) patients were disease free at the end of the last follow-up period. None of the patients had distant metastasis. As only one patient was considered to have died of disease at the end of the last follow-up, Kaplan-Meier curves could not be plotted. The median disease-free survival and overall survival for the patient population were not reached at the time of analysis. The projected 2-year disease-free and overall survival was 95%. In view of the lack of failure-related events, univariate or multivariate analysis for predictors of failure was not attempted. Grade II xerostomia was seen in 18 (90%) patients during and immediately after treatment. However, most of the patients had a significant relief from xerostomia at the end of 1 year and could eat dry food with occasional sips of water only. At the end of the last follow-up, 14 of 18 patients had recovered salivary function to the extent that they had only grade I xerostomia [Figure - 5]. The maximum grade of dysphagia seen at any point post radiation was grade I. This was seen in 11 (55%) patients. None of the patients experienced grade II dysphagia during follow-up and all patients who had Ryle′s tube insertions were able to maintain their nutrition per orally 2 months after the completion of treatment. At the end of the last follow-up, only six patients had grade I dysphagia. Aspiration during food intake was noted in one patient during follow-up who also had grade I dysphagia. It resolved at 6 months of follow-up without therapeutic intervention. None of the patients had appreciable hoarseness of voice at the last follow-up. Four (20%) patients had failed to regain the baseline weight till the end of the last follow-up. None of the patients had evidence of neurological toxicity at the end of treatment. Grade I hyperpigmentation was noted in seven (35%) patients during the follow-up but at the end of the last follow-up, hyperpigmentation was noted in four (20%) patients only. None of the patients had social problems secondary to hyperpigmentation. Grade II lymphedema was noted in five (25%) patients during follow-up but at the end of the last follow-up, only two patients had residual grade II (10%) edema and fibrosis. Discussion The concept of SIB-IMRT was first proposed by Mohan et al. [3] SIB-IMRT gives the advantage of better target conformity with less dose spillage in critical organs. [11],[12] At the same time, it allows delivery of a higher dose of radiation to smaller subvolumes in the target in a shorter period of time. [13] SIB-IMRT has been evaluated in the clinic in several western institutions but experience in this treatment modality is less in developing countries like India. [7],[8],[14],[15] Even in the west, dose schedules that have been used have significant heterogeneity in terms of total dose, dose per fraction, and target selection. It is therefore not surprising that markedly different results in terms of toxicities have been reported. This is important as application of these schedules without proper evaluation may prove counterproductive in the Indian setting. Keeping this in mind, during the design of this study we attempted to limit our case selection to those patients who had a good general condition and comprehensive familial and socioeconomic support. This is attested to by the finding of 80% of our patients being literate and majority (75%) of them having KPS of more than 80. None of the patients in our study had received concurrent chemoradiation. This was a conscious choice by the radiation oncologists as we were not sure as to the tolerance of patients to the integration of chemotherapy with the accelerated schedule of SIB-IMRT. While concurrent chemoradiation has become the standard of care of locally advanced head and neck cancers, its routine application in the Indian setting still needs to be tempered with caution. [16] The observation that 65% patients in this study had grade III mucositis lends credence to our belief. This high incidence of mucositis in the present study should be contrasted against the incidence reported by Studer et al. (15% grade III mucositis despite the use of cisplatin-based chemotherapy in 67%). [15] Other western authors have also reported rates of grade III mucositis ranging from 37% to 55% in their series of patients treated with SIB-IMRT. [7],[8],[17],[18] This higher than expected rate of acute mucosal toxicity, may limit tolerance to aggressive chemoradiation schedules in our setting. However, we are aware that the target delineation done in the present study may be considered generous by some and that might have resulted in the higher mucositis rate. With more experience and better imaging, we hope to reduce our volumes with an expected decrease in acute toxicity. The overall treatment compliance was good, with only one patient failing to complete the prescribed treatment due to mucosal toxicity. Noteworthy is the fact that all patients who had required gaps during the course of treatment were treated with the SIB-72 schedule. In our experience, the patients treated with the SIB-72 schedule had often greater areas of the oral cavity involved with confluent mucositis but the lack of spatial information in the CTCAE grading scheme limits our ability to present factual data regarding this observation. Nonetheless, the higher mucosal damage produced in SIB-IMRT schedules employing doses more than 70 Gy or dose per fraction more than 2.2 Gy has been highlighted by Studer et al. who found that seven patients in their series had subacute mucosal ulcerations after the completion of treatment. [15] None of the patients in this population had grade III dermatitis during treatment. This is in contrast to the findings of Chao et al., in whose series almost 21% of the patients had experienced grade III dermatitis during treatment. [18] Lee et al. have highlighted the importance of the tangential nature of beam entry and the bolus effect produced by the thermoplastic casts in the production of this kind of dermal toxicity. [6] They have recommended the trimming of the PTV to a depth of 5 mm from the skin surface and giving separate constraints to the skin. In our experience, however, we have observed that giving constraints to the skin results in dose calculation errors. However, with the trimming of the PTV as is done in our institute, we have not experienced increased dermal toxicities in the acute or late phase. Recently, with the acquisition of a TLD system, we have started to monitor the skin doses during the course of treatment in our patients. Control rates in contemporary IMRT series using SIB-IMRT have been uniformly good. Selected results have been shown in [Table - 4]. [7],[8],[17],[18],[19] The loco-regional failure pattern and the disease-free survival in our patients are comparable to these excellent results reported in the western literature. Target delineation is an important component to the successful execution of SIB-IMRT. Traditionally, it has been felt that the use of highly conformal radiation techniques can lead to increased incidence of marginal failures. In this regard, it is noteworthy that marginal failures were reported to account for almost 40% of total loco-regional failures in some early series of SIB-IMRT. [7] However, contemporary series like that of Studer et al. have shown that marginal failures accounted for only 5.2% of all loco-regional failures. [19] The authors have reported that they used a margin of 1-1.5 cm for the PTV. In our study, the use of a 0.5-cm margin did not lead to an increase in the incidence of marginal failures. The use of a 1.5- to 2-cm CTV margin allowed us to customize the target volume according to the known natural pathways of spread of the disease and thereby led to a decrease in the volume of normal tissue irradiated, which would not have been possible with the use of isotropic PTV margins. The use of a 0.5-cm isotropic PTV margin seems appropriate in our setup using our immobilization technique and verification. Late toxicity was generally mild and tolerable in majority of the patients. Unlike several contemporary series of concurrent chemoradiation reporting a high incidence of laryngopharyngeal toxicity, we are yet to observe significant morbidity in this area. SIB-IMRT series using concurrent chemoradiation may lead to feeding tube requirement in 20-30% of the patients treated. [8],[15] The median time to the removal of PEG has ranged from 3 to 6 months in various series. De Arruda et al. have reported grade III pharyngeal reactions in 16% patients and three patients in their series had developed cervical esophageal stenosis. [8] Simmons et al. have also reported that dose to the pharyngeal constrictors and larynx correlate with the incidence of dysphagia and aspiration. [20] In contrast, in our series, significant dysphagia was not seen after treatment. Like other contemporary series of IMRT, we also had the opportunity to witness the heartening return of near normal salivary secretion in the spared parotid glands. [21],[22],[23] Noteworthy is the fact that despite the use of generous CTV margins and treatment of both sides of neck in all patients, at least one parotid could be spared with resultant grade 0 to I xerostomia in 80% patients. However, we do acknowledge that the lack of quantification of salivary gland function remains a drawback in the present study. With the availability of quantitative salivary scintigraphy in our institution, we are planning to obtain better quantification of the salivary gland function in future. Conclusion The use of IMRT has allowed sparing of salivary function in a significant proportion of patients. The SIB-IMRT schedule used in our setting is effective, clinically feasible, and results in satisfactory loco-regional control. However, the integration of chemotherapy remains to be investigated in future prospective studies prior to routine use. Acknowledgments Authors are thankful to Mrs. Ashma Awasthy, Mrs. Dipti Dhingra, Mr. Naresh Kumar, and other technical staff of the Department of Radiotherapy, PGIMER, Chandigarh. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09043t4.jpg] [cr09043t3.jpg] [cr09043f2.jpg] [cr09043f3.jpg] [cr09043t1.jpg] [cr09043f4.jpg] [cr09043f5.jpg] [cr09043f1.jpg] [cr09043t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}