 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
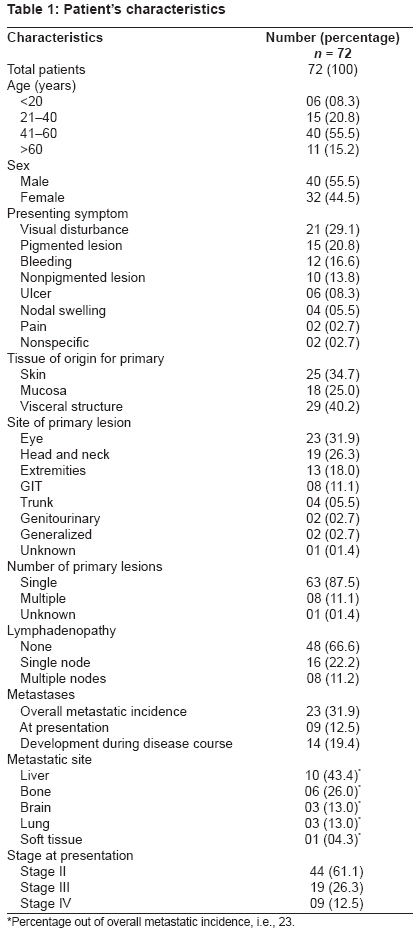
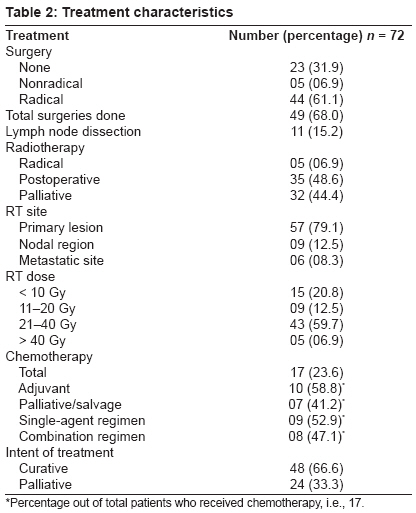
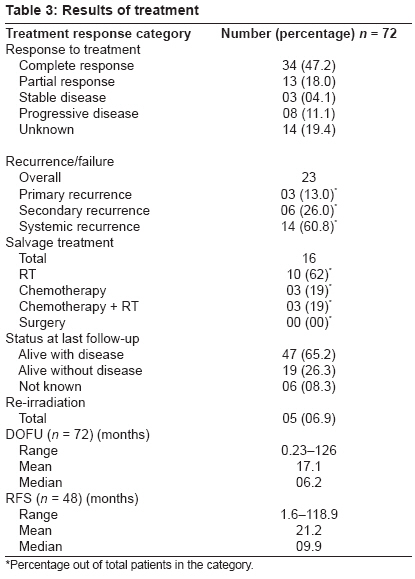
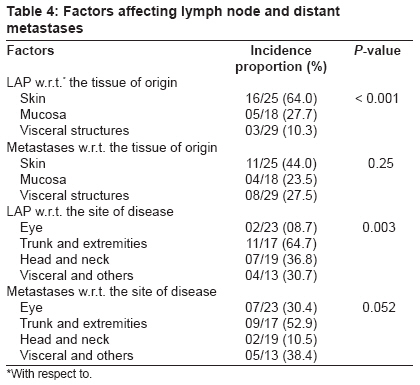
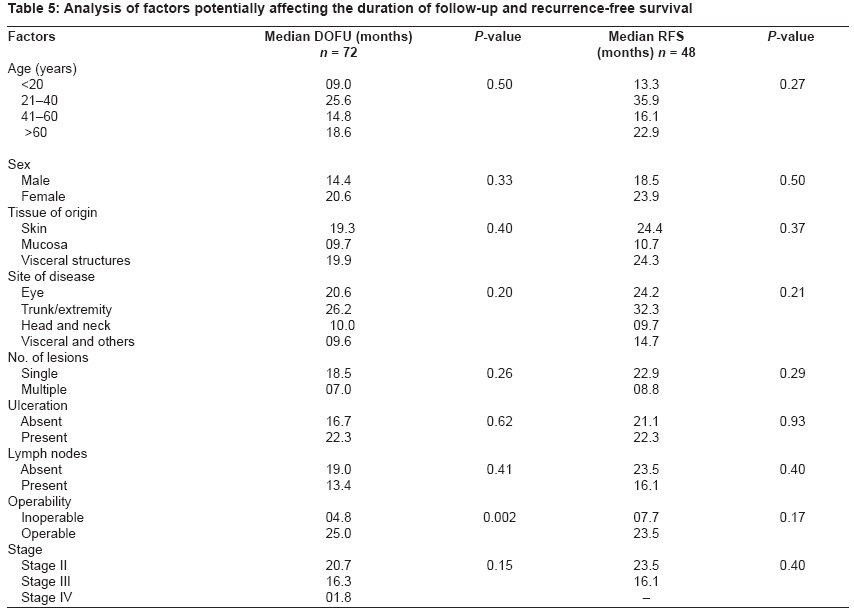
Journal of Cancer Research and Therapeutics, Vol. 5, No. 3, July-September, 2009, pp. 173-180 Original Article Malignant melanoma: A retrospective series from a regional cancer center in India Sharma Kuldeep, Mohanti BidhuK, Rath GauraK Department of Radiation Oncology, Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi Code Number: cr09044 PMID: 19841558 DOI: 10.4103/0973-1482.57122 Abstract Purpose : To present our experience in treating malignant melanoma patients.Methods and Materials : All melanoma patients treated at the Department of Radiotherapy, All India Institute of Medical Sciences, New Delhi, India, from 1995 to 2007 were studied retrospectively. The endpoints were loco-regional recurrence, distant recurrence, recurrence-free survival (RFS), and duration of follow-up (DOFU). RFS and DOFU were analyzed with respect to the factors like age, sex, tissue of origin, site of disease, number of nodes, lymphadenopathy, ulceration, stage, and operability to find out any association. Results : Seventy-two patients were found evaluable with 40 males and 32 females (median age 46.5 years). Eye was the commonest primary site with visual disturbance as the commonest symptom. Overall, 87% of the lesions were single, with most of the nonocular lesions presenting in the advanced stage. During the disease course, regional lymphadenopathy and distant metastases were seen in 33% and 32% of cases, respectively. Highest incidence of lymphadenopathy was seen in skin lesions and in primaries from trunk and extremities. Of all treated patients, 47% achieved complete response, 18% partial response, and others had either stable or progressive disease. The median DOFU was 6.2 months. RFS was studied only in curatively treated cases with a median of 10 months. Operability at presentation was the only prognostic factor influencing DOFU. Conclusion : Malignant melanoma is an uncommon disease in India carrying a lot of morbidity due to late presentation. Its management is still not clear regarding the optimum use and schedule of treatment modalities. More prospective studies in the future are required to come to a definite conclusion. Keywords: India, management, melanoma, radiotherapy, results Introduction Among the common skin cancers, melanoma is the most lethal. Although, it comprises only 3% of all skin cancers diagnosed each year, it accounts for approximately 75% of all skin cancer-related deaths. [1] Whereas both incidence and mortality are decreasing or leveling off in the younger population, rates are still increasing in the older age groups. [2] The rate of increasing incidence varies geographically with "high incidence regions" like Australia, "moderate incidence regions" like Canada and USA, and "low incidence regions" like Scotland and India. [3] Presentation differs between genders. The commonest site in males is the trunk followed by head and neck, whereas in females it is the lower limb. [2],[3] Males usually present at an older age and with a later stage of disease. [2] Melanoma in children and adolescents is rare and remains understudied. It accounts for less than 3% of all childhood neoplasms. Spitzoit melanomas is a subtype, typically seen in children, with majority of them not confirming to the "ABCD rule" for melanoma (asymmetry, border irregularity, color variation, and diameter> 6 mm). [4] Most melanomas have two phases of growth, an initial radial (horizontal) and a later vertical growth phase. The radial phase is not associated with spread, but once vertical phase supervenes, it gives rise to cell population that can metastasize. [5] The rate of distant spread is closely related to the number of involved nodes, whereas the risk of regional (in-basin) recurrence is related to the extra-capsular extension of the nodal disease. [6] Whereas the overall prognosis of an earlier diagnosed thin tumor is excellent, once metastasized it becomes an incurable disease with high mortality. [7] The overall prognosis is dependent on certain other parameters like sex, anatomic location, size, level of invasion, thickness, type of the primary, ulceration, and number and status of regional nodes. [5] According to the American Joint Committee on Cancer (AJCC), the 5-year survival for stage I melanoma exceeds 90%, but falls precipitously with nodal involvement and increasing thickness. [1] Regarding the prognostic importance of various factors, the anatomical site of stage IV tumors correlates with survival, with metastasis to brain and visceral sites having the worst prognosis. [8] Treatment of melanoma involves multimodality approach involving surgery, radiotherapy (RT), chemotherapy, and immuno-/biotherapy. Surgery includes resection of the primary, lymph node dissection (LND), sentinel lymph node biopsy (SLNB), and resection of metastases in selected cases. Optimum resection of the primary is the initial step in treating early-stage disease. Lymph node dissection, which may be therapeutic or elective, is an important step in melanoma surgery. At many institutions, SLNB has replaced elective LND and is done as a supplement to local excision to prognosticate the patients. [9],[10] Usually, patients with negative SLNBs are observed, whereas patients with positive SLNBs undergo completion lymphadenectomies, but routine application of this policy still remains controversial. [11] Metastasectomy has a role in the management of stage IV melanoma and confers survival advantage in selected cases. [8] Radiotherapy as a primary treatment for melanoma is rarely indicated but its role in adjuvant, elective and palliative treatment is well established. [9] Extensive facial lentigo maligna melanoma is an exception, where primary RT is an acceptable alternative. [12] Adjuvant RT has been advocated in the presence of high-risk features that predict for loco-regional failure but its exact role and schedule remains controversial. [1],[2],[9],[10] The efficacy and safety of RT has remained an important issue among caregivers for decades. An earlier prospective trial by Creagan et al., assessing adjuvant RT did not show its benefit in loco-regional control but a recent review by Bastiaannet et al. recommended adjuvant irradiation after LND in order to improve regional control but not survival. [13],[14] Elective irradiation can be a viable alternative to elective LND and SLNB in patients for whom dissection and systemic therapy are not the best therapeutic options. [9] An extensive literature exists regarding the use of RT in metastatic melanoma cases with approximately two-thirds of such patients experiencing overall response. [15] Delaney et al. estimated that 23% of all melanoma patients should receive at least one course of irradiation in their lifetime. [16] Yet, it appears that the utilization of RT in the management of melanoma is less than optimum. [2] Based on the historical data, many clinicians still believe that melanoma is a radio-resistant disease and this is one important reason for the underutilization of RT in melanoma patients. [17] Although earlier retrospective data suggested less sensitivity of melanoma to radiation delivered at a low dose per fraction, it is now well documented that regardless of the fractionation schedule, melanoma cells are radioresponsive if adequate total doses are delivered. [18],[19],[20] The role of chemotherapy in the treatment of melanoma remains controversial, with only few drugs showing an in vivo activity. Dacarbazine and its active metabolite temozolamide remain the most active single agents showing overall response in 15-20% of patients and complete response in 3-5% with a median response duration of 4-6 months. [8] Interleukin-2 (IL-2) is the only biological drug approved by the U.S. Food and Drug Administration for stage IV melanoma. [8] The combined use of biologic agents and chemotherapeutic drugs can produce response rates of 40-60% with an approximately 10% complete response rate. [21] Various studies have reported the treatment results of malignant melanoma. Following LND alone, nodal basin failures have been reported in as high as 50% cases. However, with postoperative RT to the tumor bed, basin failure was seen in less than 20% cases. [22] Patients with multiple nodal involvement and/or extra-capsular extension have a high incidence of regional failure. Although, most melanoma patients die as a consequence of distant metastases, which usually manifest within 2 years of treatment, loco-regional recurrence causes substantial morbidity to them. [23] The median survival in most series of treated melanoma ranges from 2 to 4 years. The 5-year overall survival is 20-45% with a disease-free survival of 30% or less. [1],[2],[6],[9],[19],[21] It is highly discouraging that the survival in these patients has not improved appreciably despite decades of investigations for novel treatment agents. [21] The purpose of this paper is to present the experience in the management of malignant melanoma of all types referred for RT at a single institution. Materials and Methods It is a retrospective study involving all malignant melanoma patients registered from January 1995 to April 2007, in the Department of Radiotherapy, All India Institute of Medical Sciences, New Delhi, India, which is a regional cancer center under the National Cancer Control Program of Government of India for patient care, academics, and cancer research. This is a referral center with an apex ophthalmology center situated in the same premises. Patients with malignant melanoma involving all sites were included in this analysis. Patients′ data were obtained from the patients′ individual record files. Only those patients whose records with reasonable details could be traced were evaluated at the end. The following information was retrieved in each case: age at diagnosis, gender, main symptom and its duration, location of the primary, disease extent, treatment details and its outcome, status at last follow-up, and follow-up duration. At presentation, all patients underwent full history, physical examination, routine blood tests, chest radiography, and other relevant investigations. Histopathologic diagnosis was confirmed by a pathology review at our own institute. During analysis, all patients were restaged retrospectively according to the 2002 AJCC staging system to have uniformity. The evaluation of treatment response was based on standard World Health Organization (WHO) criteria: CR = complete response (100% tumor remission); PR = partial response (< 100 unto 50% remission); SD = stable disease (< 50% remission unto 25% tumor progression); PD = progressive disease (>25% tumor progression). Endpoints for this study were in-field or loco-regional recurrence, distant metastases, death, or last follow-up. Duration of the follow-up (DOFU) was defined as the date of last follow-up or death minus the date of diagnosis and it was used as a surrogate parameter to estimate overall survival of the patient since data regarding the patient′s death were not available in cases that were lost to follow-up. Although, not ideal, DOFU can be the best indicator of overall survival in certain situations where follow-up and death information is not up to the optimum. Recurrence-free survival (RFS) was defined as the time interval from the date of diagnosis till the date of recurrence. The date was censored at the date of last follow-up when there was no recurrence. RFS was analyzed only in those patients who were treated with a radical intent. DOFU and RFS were analyzed with respect to the factors like age, sex, tissue of origin, site of disease, lymphadenopathy, number of lesions, ulceration of lesion at presentation, stage, and operability to derive the relationship between DOFU or RFS and these factors. The data were entered into Excel format and were analyzed using the Statistical Package for Social Sciences (SPSS), version 15.0, software. The statistical technique applied was descriptive statistics like mean, median, standard deviation, etc; the chi-square test was used for qualitative variables. The comparison between the two groups, in continuous variables, was made by applying the t-test or the Mann-Whitney test. For more than two groups, comparison was made by one-way ANOVA or the Kruskal-Wallis test. The log transformation was applied to RFS and DOFU to make them normal. Statistical significance was taken as a P-value < 0.05. Results Patient, tumor and treatment characteristics Out of the total 78 patients registered in the department during the study period, 72 patients were found evaluable (patients whose records with reasonable details could be traced) with 40 males and 32 females. The median age at presentation was 46.5 years (45 in males and 47 in females) with a range of 13-82 years. The most common presenting symptom was visual disturbance (29.1%) followed by pigmented swelling, bleeding, ulceration, nodal mass, and others. The median duration of symptoms was 5 months (range 1-60 months). Eye was the most common primary site followed by the head and neck region (disease characteristics are presented in [Table - 1]). Majority of the lesions, i.e., 87% were single. Overall, regional lymphadenopathy was present in 33% while systemic disease was seen in 32% of cases at some point during the disease course. Except for ocular melanoma patients, who presented at an early stage, most other patients presented with an advanced disease (stage III or IV). Amongst males, 42% presented with an advanced disease as compared to 34% females. In 19 (26.3%) patients, some long-standing pre-existing lesion was present at the site of malignant melanoma. Family history of malignancy was positive in only one patient. History of exposure to agents like tobacco, alcohol, occupational fumes, gases, etc., was found in 20 patients. Forty-eight (66.6%) patients were treated with curative intent while remaining 24 were treated for palliation [Table - 2]. Among the radically treated patients, primary radical surgery was done in 44 (91.6%) patients while RT as the primary modality was used in five patients. Patients treated with radical RT had their primary lesions in the mucosa of the head and neck region in three patients and cervix and vulva in one each. Five patients underwent nonradical or salvage surgery. One patient underwent radical surgery initially but developed brain metastasis within 6 weeks and the intent was converted to the palliative one. Eleven of the 49 surgically treated patients underwent LND as a part of their surgical procedure. Prophylactic LND was not performed in patients without nodal disease at presentation. Likewise, SLNB was also not performed in any of our patients. All the 72 patients received RT in one of the three forms, i.e., radical in 5, postoperative adjuvant in 35, and palliative in 32 patients. Thus, the maximum number of patients (48.6%) were treated with surgery followed by postoperative RT, which was given for indications like residual disease, close or positive margins, disease recurrence, and regional node metastases. In 79% cases, RT was given to the primary lesion while in others, radiation was delivered to either the nodal or the metastatic site. The prescription dose in cases of radical or adjuvant RT was generally 40 Gray (Gy) in 10 fractions or 32 Gy in 8 fractions delivered as alternate day regimen (Monday, Wednesday, and Friday). In one patient of melanoma of the cervix, 50 Gy in 25 fractions was given by external beam RT, followed by 35 Gy (LDR equivalent) by brachytherapy, adding up to a total dose of 85 Gy. In palliative cases, RT was given as 20 Gy in 5 fractions or a single fraction of 8 Gy. Overall, the dose range varied from 8 Gy to 85 Gy with maximum number of patients, i.e., 43 (59.7%) receiving a dose between 20 and 40 Gy. Radiation portal varied depending on the location of disease, but in general, encompassed the entire tumor bed and regional lymph nodes when judged to be at high risk. Systemic therapy was prescribed to 17 patients and the prescription was entirely on the discretion of the medical oncologist. Ten patients received adjuvant chemotherapy, while seven patients received chemotherapy as palliative or salvage treatment. Nine patients received a single agent while others were given combination regimens. Chemotherapeutic agents used were dacarbazine, cisplatin, vinblastine, tamoxifen, and interferon in various combinations. The number of cycles ranged from 1 to 8 (average 3). Patient survival and disease outcome Out of the total 72 patients, 34 patients (47.2%) achieved CR after their primary course of treatment, 13 patients (18%) achieved PR whereas 3 patients had stable disease and 8 patients had progressive disease [Table - 3]. The treatment response was not recorded adequately in files of 14, i.e., 19.4% cases. Till the time of manuscript preparation, 23 (31.9%) patients had relapsed. Three patients developed local failure, 6 developed regional failure, and 14 developed distant metastases. Liver was the commonest site of metastases followed by bones. Out of the total 23 patients who relapsed, 16 patients (69.5%) received salvage treatment in some form. Ten patients received RT, three patients received chemotherapy, and three patients were treated with combined RT and chemotherapy. Overall, five patients received re-irradiation. Surgery was not used as a salvage treatment in any case. At the last follow-up, 47 (65.2%) patients were alive with residual or progressive disease while 19 (26.3%) were alive free from disease. In six cases, disease status was unknown at the last follow-up. Recurrence-free survival in 48 radically treated patients ranged from 1.6 to 119 months, with a median of 10 months. The overall DOFU for the 72 patients till the last follow-up ranged from 0.23 to 126 months, with a median of 6.2 months. Analyses of relationship between the tissue of origin of the primary and the incidence of lymphadenopathy and distant metastases revealed the highest incidence of lymphadenopathy in skin lesions followed by mucosal and visceral lesions. The difference was found to be highly significant (P < 0.001) [Table - 4]. The metastatic incidence was also seen most frequently in skin lesions followed by visceral and mucosal lesions but the difference was not statistically significant. Likewise, analyses of the relationship between the site of disease and the incidence of lymph node and distant metastases showed highest incidence of lymphadenopathy in lesions of the trunk and extremities with lowest incidence in lesions of the eye. This difference was also statistically significant (P = 0.003). The incidence of metastases was also highest in trunk and extremity lesions with the incidence lowest in head and neck lesions; the difference approached near the limit of significance (P = 0.052). Analyses of DOFU with various factors showed that it was significantly longer in patients presenting with operable lesions as compared to those presenting with inoperable lesions (P = 0.002) [Table - 5]. Longer DOFU was also seen in the age group of 21-40 years as compared to others but the difference was not statistically significant. Likewise, patients presenting with a single primary lesion had longer DOFU as compared to those with multiple lesions but again the difference was insignificant. Other factors like sex, tissue of origin, site of disease, ulceration of primary lesion, and lymphadenopathy were not found to affect DOFU. Likewise, RFS was also independent of all the above factors. Discussion Melanoma is a relatively uncommon skin cancer in geographical locations like India. Its highest incidence is seen in sixth decade as observed in our series. [1],[8],[9],[12] Unlike the literature, no difference was seen in the median age of presentation among males and females. The slight male predominance in our series is consistent with reports from other studies. [1],[6],[24] Wanebo et al. reported a slight female preponderance in their small series. [25] Although skin is the commonest tissue of origin for melanomas, the mucosal and visceral sites are not uncommon. Ocular melanomas were seen more frequently in the present study as compared to their general prevalence. [5] The reason for this could be the center being an apex referral cancer institute and also a large number of cases being referred from the apex ophthalmology center situated in the same premises. In a number of cases, the frank melanotic lesion is preceded by a long-standing indolent lesion at the same site. In our study, such lesions were seen in 26% cases. Thus, the presence of such lesions should prompt the patient and the physician to immediately investigate such benign-looking lesions. Although family history was not found related to the occurrence of these lesions, the possibility should not be ruled out, since more robust data and extensive studies are required to establish such relationships. Several studies have identified that the utilization of radiation facility in melanoma treatment can vary according to factors unrelated to disease such as age, socioeconomic status, infrastructure available, or proximity to a cancer center. [2],[9],[26] Ideally, the use of RT should be independent of these factors. All the patients in our study received RT as a part of their treatment as this study utilized the data of only those patients, who were referred for RT to our department. Usually, as a policy, the patients who do not require RT are not registered in the radiotherapy department. The dose and fractionation of RT in melanoma treatment remain controversial for decades and different regimens are being practiced. Higher dose per fraction has been used because of patients′ convenience, a positive experience in various trials and a continued belief that some melanoma cells are more sensitive to large dose per fraction. [12],[27] A radiobiologic study by Overgaard demonstrated that a conventional fraction of 2 Gy is inadequate and a dose of 4 Gy per fraction is needed. [18] The average dose fractionation regimens used by French et al. for a different treatment intent were 20.2 Gy in 5 fractions for palliative, 40.2 Gy in 14 fractions for radical, and 40.4 Gy in 15 fractions for adjuvant treatment. [2] In studies from the M. D. Anderson Cancer Center, the most commonly followed regimen for adjuvant irradiation is 30 Gy at 6 Gy per fraction delivered twice weekly over 2.5 weeks. [6],[9],[27] In RTOG 83-05 study, no difference could be detected in partial or complete response between 2.5 Gy delivered 5 days a week and 8.0 Gy delivered once weekly for 4 weeks. [20] Unfortunately, the duration of response was not analyzed in that study; thus, the radioresponsiveness to each schedule could not be determined. The dose of RT varied widely between patients in our study due to the heterogeneous group of patients. A potential disadvantage of higher dose per fraction is that small-dose heterogeneity in fraction size and total dose can result in profound changes in late normal tissue responses. Therefore, meticulous attention in treatment delivery is required, because minor field variations which are clinically insignificant when conventional 25-30 fractions are delivered can result in meaningful under- or overdosage during a course of only 5-10 fractions. [28] Thus, if the disease is lying adjacent to a critical structure or require a large radiation field, conventional fractionation is preferred. [1] The recommended dose would be 20 Gy in 4 fractions and 40 Gy in 10 fractions (2-3 fractions per week) for palliative and radical intent respectively. The postoperative adjuvant dose would be 48 Gy in 20 fractions over 4 weeks. [2],[9],[17],[18],[28] In our study no conclusion could be made regarding chemotherapy due to small number and limited follow-up of the patients of advanced stage melanomas who were offered chemotherapy. The optimal management of regional nodes from melanoma is not well defined. The rate of regional nodal recurrence after local excision of primary ranges from 20 to 60%. [9] Bonnen et al. found the median time to the development of loco-regional recurrence as 17 months (range, 2-53 months) in patients of cutaneous melanoma of head and neck. [9] In our study, overall nodal failure was seen in 13% of radically treated patients. This is lower in comparison to the incidence reported in the literature. The presumable reason may be the patients seeking alternative treatment after recurrence, which is a common practice in India, that results in underreporting of the actual events. Recurrence pattern varies from series to series. Christopher et al. in a series of head and neck cases observed local recurrence in 13% and distant recurrence in 26% of cases. The incidence of distant metastases increased with the presence of positive nodes and increasing tumor thickness. [24] Bonnen et al. observed local recurrence, nodal recurrence, and distant metastases in 6%, 10%, and 36% cases, respectively, in head and neck melanomas managed with excision of the primary and elective neck irradiation. [9] Ballo et al. observed local failure in 2.5%, regional failure in 9%, and systemic failure in 51% cases managed with surgery and RT and followed for a median period of 4.2 years. [6] We observed local recurrence in 6% cases, nodal recurrence in 12%, and distant metastasis in 29% of radically treated patients irrespective of the primary sites. Although our analysis has been done with a shorter DOFU and the cases are not stratified according to the primary site of disease, the frequencies of recurrence are consistent with those reported in the literature. Seegenschmiedt et al. in their study of advanced melanoma cases observed the distribution of metastatic sites as CNS (43%), lung (36%), bone (34%), liver (17%), and other organs (13%). [29] Ballo et al. in a retrospective study in 89 patients found that the mean time to the development of distant failure was 6.6 months and the first site of failure was lung (27%), brain (20%), skin (16%), bone (13%), and others (23%). [28] This distribution is different from that observed in our series [Table - 1]. This may be due to the difference in the distribution pattern of the primary lesions seen in Germany and Indian subcontinent. In metastatic disease, the aim of the treatment must be the improvement and maintenance of quality of life. James et al. showed that conventional RT (30 Gy/10 fractions/2 weeks) does this as well as any other RT scheme. [30] The small choroidal tumors have lower incidence of distant metastases, i.e., 3% in one series. [31] In our study, the metastatic incidence was higher (30%) that could be due to late presentation when tumor invades up to a deeper level. Patterns of failure vary by anatomic location, with lesions of head and neck failing locally along with metastasis, and anal, rectal, or gynecologic lesions (clubbed as visceral lesions in our study) failing predominantly by systemic spread. [32] Our results corroborate with these observations with systemic spread seen in 10.5% of head and neck cases in contrast to 38.4% of visceral primaries [Table - 4]. In the literature, factors like age, sex, and nodal size and stage found no association with disease-free survival or overall survival in patients presenting with advanced disease. [9,29] Similar observations have been made in our study where these factors did not affect DOFU or RFS. Balch et al. confirmed patient′s age as an independent prognostic variable, perhaps representing advanced age as a surrogate for declining host defense mechanism. Other studies have also demonstrated that older patients, especially those over 60 years, have a lower survival rate. [33] Mucosal melanoma of the anus, rectum, head and neck, vulva, and vagina are rare primary sites with generally poor overall survival as compared with cutaneous melanoma. [32] Our results have also shown an overall DOFU of 9.7 months for mucosal lesions as compared to 19.3 months for cutaneous lesions. Another factor associated with overall survival is lymphadenopathy. [22] Various series have shown primary tumor thickness, nodal status, and tumor ulceration to significantly reduce the overall survival. [24],[29],[33] Ulceration is one of the most reproducible histopathologic feature clearly associated with a greater capacity to metastasize. [29] No such correlation was observed in our series, which may be due to the less number of cases (8% only) presenting with ulceration. Operability of the primary lesion at presentation was one factor that influenced the overall survival in our series. These data must be viewed with caution because of the small number of patients in the present analysis and possible selection biases inherent in the retrospective studies. More randomized trials with strict guidelines are required to answer the controversial issues regarding optimum dose and fractionation, appropriate elective management of nodal areas in the absence of clinical nodal disease, adjuvant treatment after primary surgery and LND, management of local and regional recurrences, and significance of operability of lesions at presentation. New effective drugs are needed for the treatment of stage IV melanoma as no new drug has been sanctioned by the FDA since 1996, when interferon alfa 2b was approved. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09044t5.jpg] [cr09044t1.jpg] [cr09044t4.jpg] [cr09044t2.jpg] [cr09044t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}