 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
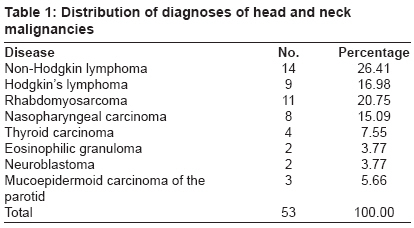
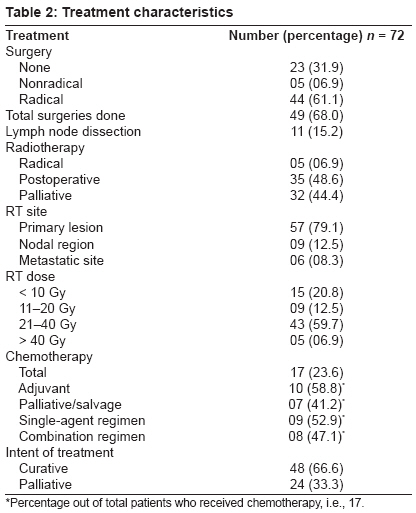
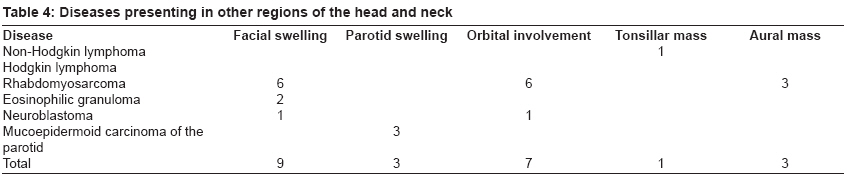
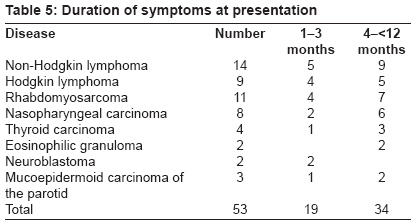
Journal of Cancer Research and Therapeutics, Vol. 5, No. 3, July-September, 2009, pp. 181-185 Original Article Clinicopathological correlates of pediatric head and neck cancer Sengupta Subhabrata, Pal Ranabir Department of Community Medicine, Sikkim-Manipal Institute of Medical Sciences and Central Referral Hospital, Sikkim Code Number: cr09045 PMID: 19841559 DOI: 10.4103/0973-1482.57123 Abstract Background : The spectrum of head and neck tumors in children continues to be the cause of diverse, diagnostically challenging issues.Aims : To demonstrate and compare the unique clinicopathological features in our study population and their correlations with the final histopathological diagnosis. Methods : Fifty-three children with head and neck cancer were examined thoroughly at the Otorhinolaryngology department in a tertiary care teaching hospital followed by histopathological studies. Results : Lymphomas were the most common malignant lesions seen followed by rhabdomyosarcomas, nasopharyngeal carcinomas, and others like thyroid carcinomas and eosinophilic granulomas. In the neck, the commonest cause of primary malignant disease was lymphoma; however, the most frequent lesion was reactive lymphadenitis. In the sinonasal region, the commonest malignancy was rhabdomyosarcoma, which often had extension to the orbit and the face. Recurrent epistaxis was found universally in the malignant cases of this region. In the facial region, disfiguring swelling with proptosis was mainly caused by rhabdomyosarcoma. The only case of tonsillar malignancy was due to non-Hodgkin lymphoma. The duration of disease was less than 1 year. Conclusion : The most common manifestation of the malignant lesions in the pediatric age group was with a history of an enlarging, painless neck swelling. Still, an insignificant lump in the neck or recurrent bleeding from nose may be the manifestation of an underlying cancer. Keywords: Clinical presentation, pediatric head and neck tumor Introduction Most of the head and neck masses which occur in childhood are benign in nature. However, neoplasms of the head and neck account for approximately 5% of all childhood malignancies. A diagnosis of malignancy may represent a primary tumor or metastatic foci to cervical nodes. [1] The otorhinolaryngologist who treats children must have knowledge of the neoplasms that can occur in childhood as neck masses often present a diagnostic challenge to the primary care provider. We attempted to analyze various clinical modes of presentation of pediatric head and neck cancers, and their correlation with final histopathological diagnosis, and to identify those features which separate them from various other benign conditions. Materials and Methods The study period was of 3 years (2001-2004). This cross-sectional study was carried out at a tertiary care teaching hospital at Calcutta with a study population of 161 children below 12 years with head and neck tumors. Primary intracranial, intraorbital tumors and inflammatory swellings mimicking neoplasms were excluded from the study. Nonneoplastic swellings presenting as tumor-like conditions were however included in the study. Reactive cervical lymphadenitis, the most common cause of neck swelling in children, was not included in the study, but their number was noted for comparing their frequency with other primary and secondary neck swellings in children. Data collection procedure Institutional ethical committee approved the study. All the caregivers of the patients were explained about the purpose of the study and were ensured strict confidentiality. Written informed consents were taken from each of the caregivers of the children prior to the study. The participants and their caregivers were given the options not to participate in the study if they wanted. The principal investigator thoroughly examined all the children at the ENT department precisely by taking a detailed history, general examination along with a system-based otorhinolaryngological assessment. Endoscopic procedures, investigations like X-Ray, CT scans and MRI of the head and neck region, FNAC, and a biopsy for the histopathological study were done as required to arrive at the diagnosis. All the cases were histopathologically confirmed followed by evidence-based interventions according to the international clinical protocol. Information on pediatric oncology was disseminated in health education sessions to complement the findings of study. Statistical analysis used The data collected were thoroughly cleaned and entered into MS-Excel spread sheets, and analysis was carried out. The procedures involved were transcription, preliminary data inspection, content analysis, and interpretation. Percentages were used in this study to analyze epidemiological variables. Results Fifty-three children below 12 years of age were diagnosed having head and neck cancer from a pediatric population of 21,216 (0.25%) attending the Otorhinolaryngology department during our study period. In our series, the lymphomas were the most common (43.39%) malignant lesions diagnosed. This was followed by the rhabdomyosarcoma (20.75%) and nasopharyngeal carcinoma (15.09%). Of the lymphomas, the non-Hodgkin lymphoma was predominant (26.41%) [Table - 1]. Neuroblastoma and eosinophilic granuloma were mostly seen in infancy. Overall, all the other malignant lesions were more common in the age group above 5 years (69.81%), and maximum in the age group of 10-12 years (47.17%). The overall sex ratio was 1.78:1 in favor of the males, except in thyroid carcinoma and neuroblastoma where the ratio was equal. Eosinophilic granuloma was found only in two male kids. In the neck region, the commonest malignancy was lymphoma, which was often associated with constitutional symptoms like fever. Metastatic secondaries in the neck were most commonly associated with nasopharyngeal carcinoma and few cases of metastatic thyroid and carcinoma of the parotid. Other symptoms like dysphagia, hoarseness, and stridor were associated with thyroid malignancies [Table - 2]. In the sinonasal region, most common malignancy was rhabdomyosarcoma, which often had extension to the orbit and the face. Multiple cranial nerve palsies along with neck secondaries were usually seen in the cases of nasopharyngeal carcinoma. Recurrent epistaxis was found universally [Table - 3]. In the facial region, disfiguring swelling with proptosis was mainly caused by rhabdomyosarcoma, and there was only one case of neuroblastoma. Eosinophilic granuloma was found in the forehead and the postaural region. The only case of tonsillar malignancy was due to non-Hodgkin lymphoma [Table - 4]. The duration of illness ranged from 1 month to 1 year; maximum patients had duration of illness between 4 and 12 months (39.13%) [Table - 5]. Discussion The study included all the pediatric patients with head and neck masses attending the Department of Otorhinolaryngology. We did not have a pediatric head and neck oncology unit, so all the cases having head and neck lesions were referred to us, as a result of which this study included all the cases of pediatric head and neck cancers from our hospital. To analyze the modes of presentation of different malignant lesions, the entities were broadly divided into three main categories according to the site of involvement in the head and neck. They were grouped as (i) those primarily involving the neck; (ii) those involving the nasopharynx and sinonasal region; and (iii) other areas of the head and neck like the face, orbit, ears, etc. Majority of our patients presented with a painless neck mass. We got 106 patients who had neck swelling, including the cases of secondary metastasis. The world literature states that the most common etiology for cervical adenopathy in children is reactive lymphadenopathy following a viral or bacterial illness. Persistent adenopathy raises more concerns, especially enlarged lymph nodes within the posterior triangle or supraclavicular space, nodes that are painless, firm, and not mobile, or a single dominant node that persists for more than 6 weeks should all heighten concern for malignancy. [2] In our series also the commonest cause of neck lump was the reactive lymph nodes. They were soft, freely mobile, often tender and usually disappeared after a course of an antibiotic. A single lymph node or a group firm to hard in consistency, barely mobile or fixed, and associated with other symptoms like persistent fever or night sweats ultimately came out to be malignant for lymphoma. Midline neck swelling with dysphagia and stridor in such age group was due to a cancer in the thyroid. Hard metastatic secondaries were also easily diagnosed. Neck swellings with these features and a short history always pointed to a diagnosis of malignancy. Benign lesions could be easily differentiated from them, as they lack these typical pathognomonic features of malignancy. Similarly, in patients presenting with epistaxis and nasal mass, the main differentiating feature between a malignant and benign swelling was the extension to the adjoining areas like the face and the orbit. A simple bleeding mass in the nose without any extension to the orbit and face was usually benign. The only benign lesion which can have such extensions was angiofibroma which could be easily differentiated by a CT scan and endoscopy. A sinonasal mass with cranial nerve palsy and cervical nodes always raised a strong suspicion for cancer. Disfiguring facial swelling for a relatively short period with proptosis and impaired vision in most of the cases would turn out to be a malignant one in this age group. Most common pathology was a sarcoma or neuroblastoma. Parotid swelling with facial palsy was also such a combination which always raised the suspicion of malignancy. Lymphomas were the commonest cause of malignant neck swelling and non-Hodgkin lymphoma was more common. The most common mode of presentation of Hodgkin′s lymphoma was painless neck mass, while the children with non-Hodgkin lymphoma mostly had painful neck lymphadenopathy. Extra-nodal involvement in the head and neck was more common with non-Hodgkin lymphoma than Hodgkin′s lymphoma. Our peers also found that the cervical lymphadenopathy was the most common mode of presentation of both non-Hodgkin lymphoma and Hodgkin′s lymphoma; however, the involvement of extralymphatic head and neck sites was mostly due to non-Hodgkin lymphoma rather than Hodgkin′s lymphoma. [3] In our series, most of the patients of non-Hodgkin lymphoma presented with a mass in the neck but orbital and sinonasal involvement was also seen. One case had primary origin in the tonsil which is the commonest extranodal site of involvement for non-Hodgkin lymphoma. [4] All the cases of Hodgkin′s lymphoma presented with neck mass and constitutional symptoms like fever, night sweats, and weight loss. Apart from cervical lymphadenopathy, mediastinal, axillary, and abdominal nodal involvement was also found in both the diseases. Hodgkin′s lymphoma involved the mediastinal nodes more while the abdominal and axillary lymph node involvement was more commonly seen in non-Hodgkin lymphoma. Similar findings have been seen by Urquhart et al. whose study reveals that associated mediastinal adenopathy was more common with Hodgkin′s lymphoma, and abdominal adenopathy with non-Hodgkin lymphoma. Constitutional symptoms were more common with Hodgkin′s lymphoma. [5] Head and neck rhabdomyosarcoma usually manifests as a localized painless mass and has a high frequency of lymphatic and distant metastasis. [6] In one study by Hicks et al., it was found that primary tumor sites in the head and neck in the decreasing order of frequency were face (18%), orbit/periorbital (16%), nasal cavity/nose (14%), lymph nodes (12%), paranasal sinuses (10%), parameningeal (10%), parotid gland (6%), neck (6%), infratemporal fossa/zygoma (2%), buccal mucosa (2%), palate (2%), and larynx (2%). Metastatic disease at diagnosis (33% of all cases) occurred in the bone marrow (11%), cerebrospinal fluid (6%), peritoneal fluid (6%), lung (4%), parietal pleura (2%), pleural fluid (2%), and pericardial fluid (2%). [7] In our series, we encountered 11 cases, most commonly involving the facio-orbital region, followed by sinonasal and the nasopharyngeal region. In the orbit, they presented as rapidly developing proptosis and were diagnosed early, while in the soft tissue of the head and neck, they arose as a painless enlarging mass. We got two cases in the ear and one in the postaural region involving the temporal bone, presenting with hearing impairment and facial palsy. The world literature has records of disease involvement of temporal bone along with seventh and eighth cranial nerves and the inner ear. [8] All the eight cases of nasopharyngeal carcinoma in our series presented with cervical metastases. Other symptoms like blood-tinged nasal discharge, nasal blockage, secretory otitis media, etc., were also found. Cases of cranial nerve involvement with absent gag reflex were also noted. The world literature states that nasopharyngeal carcinoma most commonly heralds with asymptomatic cervical lymphadenopathy, nasal blockage, or epistaxis. Unilateral serous otitis media [9] or cranial nerve involvement in extensive tumors eroding the skull base is also seen in the course of the disease. [10] In a recent study from Mumbai, it was found that 91% of the patients presented with nodal metastasis. Of them, 37% had lymph nodes> 6 cm, and 56% had bilateral nodes at presentation. [11] Four cases of thyroid carcinoma were found in our study. Out of them three were papillary carcinoma with cervical lymph node metastasis, and one was follicular variant of papillary carcinoma. These findings are corroborative with the world literature which clearly states that nonmedullary thyroid carcinomas are rare malignancies in pediatric ages. The vast majority of them are papillary carcinomas while follicular carcinomas, poorly differentiated, and anaplastic carcinomas are exceptional. [12] A similar frequency distribution has been noted by Arici et al. who also found multiple lymph node metastases and even pulmonary metastasis. [13] However, we did not encounter such distant metastasis. Eosinophilic granuloma is the most frequent and most benign form of the Langerhans cells′ histiocytosis, typically affecting children of 5-15 years of age. [14] The world literature reveals case reports of eosinophilic granuloma, causing destructive bony lesions of the cervical spine in children, [14] both upper and lower jaws, [15] and frontal, zygomatic, and maxillary bones of the orbital wall. [16] Eosinophilic granuloma of the temporal bone is also well documented; the frequency varies between 15 and 60%. [17] We found two cases of eosinophilic granuloma, one presenting as a single swelling in the postaural region involving the temporal bone and the other over the frontal bone. Both presented as a soft tissue mass with a typical well-circumscribed lytic lesion in the underlying bone, with classic bevelled edge appearance in radiology. Of the two cases of neuroblastomas found in our series, one involved the orbit causing proptosis, periorbital ecchymosis, opthalmoplegia, and facial swelling. The other presented as a neck swelling in the parapharyngeal space. The world literature reveals that neuroblastic tumors are the third most common cause of solid tumors in early childhood. Cervical tumors account for only 5% of cases. Presenting signs may be solitary cervical mass, respiratory distress, cranial nerve palsy, and orbital involvement in association with Horner′s syndrome. [18] In our series, we got three cases of mucoepidermoid carcinoma of the parotid and six cases of pleomorphic adenoma, four in the parotid and two in the submandibular gland. Other studies show that the major salivary glands are the main site of tumor occurrence (79% in parotid glands), and the most common salivary tumors were pleomorphic adenomas, followed by mucoepidermoid carcinomas. [19] Head and neck cancers in children display diverse patterns of biological behavior and a considerable variation in the geographical distribution. This study presented an analysis of head and neck cancer in a tertiary healthcare center in eastern India. Further prospective population-based studies are needed to elucidate the national incidence and to identify the risk factors for head and neck cancer in the Indian children. The percentages were apparent only among all the children within this referral center. Analyzing the findings in the present study, it can be concluded that the head and neck cancers in children present in a variety of way. The treating physician has to search for those clinical features which raise the suspicion of malignancy. Commonly, the patients presented with nasal mass, epistaxis, or orbitofacial swelling. However, the most common manifestation of the disease was an enlarging, painless neck mass. Lesions in the face and neck were noticed early and brought to treatment whereas those located deep inside the nose or nasopharynx were brought late. We need a uniform definition of head and neck cancer so as to permit a comparison of international studies. We have to make people aware of these facts and motivate them, so that more and more head and neck cancers in children are brought to treatment before it is too late. It is suggested that Behavior Change Communication (BCC) programs aimed at common people are to be augmented for early detection and treatment of pediatric head and neck cancers in children. An insignificant lump in the neck or recurrent bleeding from the nose may be the manifestation of an underlying cancer. We have to make people aware of these facts and motivate them, so that more and more head and neck cancers in children are brought to treatment before it is too late. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09045t5.jpg] [cr09045t4.jpg] [cr09045t3.jpg] [cr09045t2.jpg] [cr09045t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}