 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
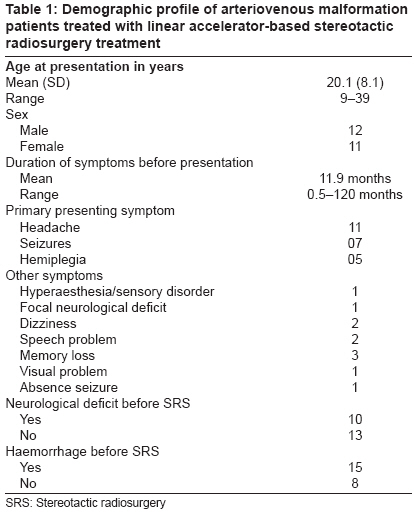
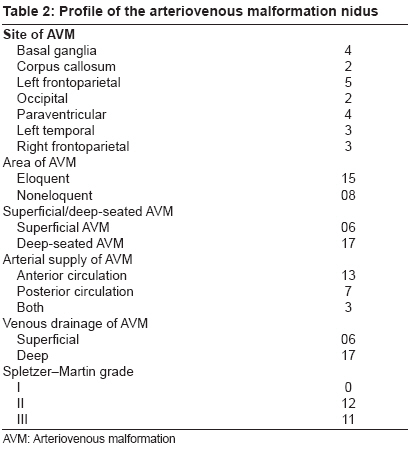
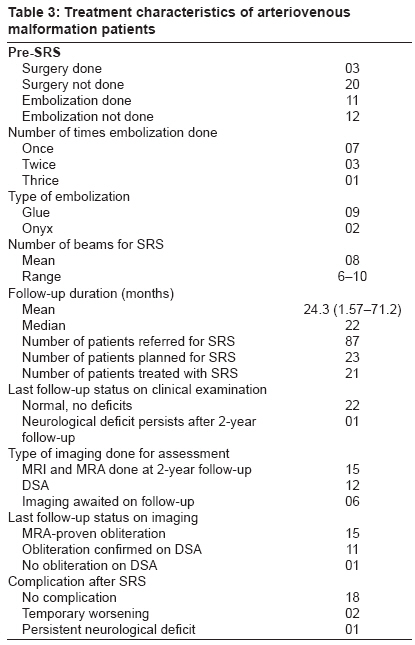
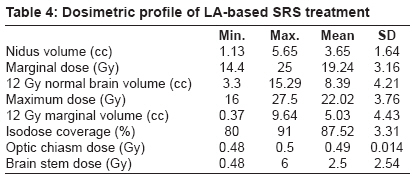
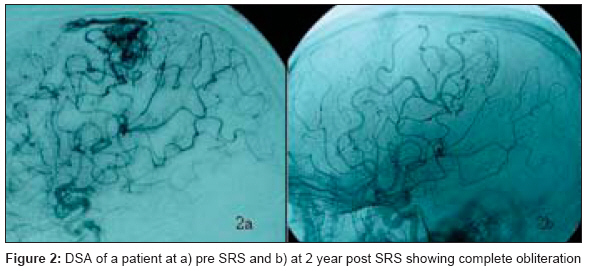
Journal of Cancer Research and Therapeutics, Vol. 5, No. 3, July-September, 2009, pp. 186-191 Original Article Micromultileaf collimator-based stereotactic radiosurgery for selected arteriovenous malformations: Technique and preliminary experience Jalali Rakesh, Dutta Debnarayan, Srinivas C, Munshi Anusheel, Limaye Uday, Goel A, Deshpande Deepak, Sarin Rajiv Department of Radiation Oncology, Tata Memorial Hospital, Mumbai Code Number: cr09046 PMID: 19841560 DOI: 10.4103/0973-1482.57124 Abstract Purpose : To report our experience of stereotactic radiosurgery (SRS) in consecutively treated patients with arteriovenous malformations (AVMs).Materials and Methods : Of the 87 patients, 23 patients qualified and were treated with SRS as per predefined protocol according to AVM size, location, neurological status, prior bleeding, and the AVM score. All had Spletzer-Martin grade II/III and AVM scores <2.5. Patients underwent SRS using micromultileaf collimators delivering multiple noncoplanar fixed fields. Doses were prescribed using the Flickinger model. Patients were followed up with magnetic resonance angiography (MRA) and digitally subtracted angiography (DSA). Results : The mean nidus volume was 3.65 cc. The mean prescribed maximum dose was 22 Gy and the marginal dose was 19.24 Gy; 12 Gy normal brain volume was 8.39 cc and 12 Gy marginal volume was 5.03 cc. Mean dose to brain stem, pituitary hypothalamic axis, and optic chiasm was 2.5, 0.72, and 0.49 Gy, respectively. At a median follow-up of 22 months (range 1.5-71.2 months), 7 of 10 patients presenting with a neurological deficit showed significant improvement. All 15 patients who underwent MRA 1.5-2 years after SRS had no residual nidus yielding an MRA complete obliteration rate of 100%. Twelve patients also underwent a check DSA, which confirmed obliteration in 11 of them resulting in an accuracy of MRA of 92%. One patient after SRS had transient deterioration of motor power, which resolved completely after a short course of steroids and another had mild worsening of the hemiparesis. All patients are able to lead an active functional life. Conclusions : Careful selection of cases suitable for SRS provides optimum obliteration rates with low toxicity. Keywords: Arteriovenous malformation, linear accelerator, micromultileaf collimator, radiosurgery Introduction Linear accelerator (LA)-based stereotactic radiosurgery (SRS) is a single-fraction radiotherapeutic technique using a combination of a stereotactic apparatus and narrow multiple beams delivered through noncoplanar fields. [1] LA-based SRS with micromultileaf collimator (mMLC) has physical, geometrical, and dosimetric advantages over the standard cone-based system especially for medium-sized irregular targets. [2] Computer-controlled mMLC allows efficient and flexible design of individually shaped static or dynamic fields, which takes the shape of a three-dimensional projection of irregular planning target volumes providing superior dose conformity. Success of SRS in arteriovenous malformations (AVMs) depends upon appropriate selection of patients. Obliteration rates of AVMs depend upon the marginal dose delivered. [3],[4] However, treatment-induced symptomatic postradiosurgery sequelae also depend upon the dose delivered to the normal brain. [5] Thus, a smaller nidus in noneloquent areas where higher dose can be delivered to the nidus has the highest probability of obliteration with minimum toxicity. In this present retrospective analysis, we describe the dosimetric and clinical outcomes of an initial cohort of consecutively treated cases of AVM patients at our centre. Materials and Methods From 2001 to 2007, 87 digital subtraction angiography (DSA)-proven AVMs were referred for SRS. Initial assessment was done for suitability for SRS in relation to location of the nidus, size of the nidus, arterial supply, and medical suitability for DSA. All cases were evaluated by neuroradiologists, neurosurgeons, and radiation oncologists prior to treatment. Patients selected for SRS had AVMs of < 3 cm nidus, located in eloquent/critical area of the brain with a high probability of a neurological deficit in the event of bleeding and with surgical interventions. Prior history of bleeding/neurological deficit was considered in the decision-making process as well. After an informed consent, patients were taken up for SRS, where a planning magnetic resonance imaging (MRI) scan was initially done in all cases 1-2 days prior to SRS with a three-dimensional fast spoiled gradient echo (3D-FSPGR) sequence in which axial postcontrast MRI sections were obtained with 1.5 mm slice thickness with no interslice gap at the equal-size matrix (256 Χ 256) and transferred to SRS planning workstation for future fusion. On the day of SRS procedure, a stereotactic rigid frame was fixed over the skull bone after application of local anesthesia at the site of appropriate pins [Figure - 1]. The target localizer box with embedded multiple fiducial rods to establish stereotactic co-ordinates was attached to the SRS frame. The use of frame and localizer box established a rigid relationship between the patient′s cranial anatomy and stereotactic co-ordinate system. After that, a DSA, usually from the femoral arterial route was performed on the patient with the stereotactic frame and localizer box on. The nidus with its feeding arteries was identified in the filling phase and marked as the target. A lot of time and effort was spent on consultation with the interventional radiologists for identifying the target for the nidus, and all sets of DSA and imaging were reviewed in detail. A computerized tomography (CT) scan was done with a target localizer box attached with the frame. Treatment planning was done with a stereotactic system (BrainLAB, Germany), which provided 26 pairs of mMLC leaves. The projected leaf width at the isocentre ranges from 3 to 5 mm giving field sizes ranging from 0 Χ 0 cm 2 to 10 Χ 10 cm 2 . In the BrainLAB workstation CT scan, MRI and DSA images were fused manually. DSA images were fused with the help of coordinates in the localizer box. The accuracy of fusion was verified before planning. The nidus and organs at risk (OARs) such as pituitary hypothalamic axis (PHA), brain stem, temporal lobes, eye, lens, optic apparatus, and normal brain were contoured. Site of the nidus, nidus volume, nidus shape, and proximity to critical structures was considered while planning. The plan and prescription dose were finalized by using the Flickinger′s model of probability of normal tissue toxicity. [5] Location of the nidus and 12 Gy normal brain volumes were considered for dose prescription. Highest possible dose was prescribed keeping the risk of normal tissue toxicity probability below 5%. Marginal dose, which covers the entire nidus volume, was given maximum importance while approving the plan. Usually, 8-10 isocentric noncoplanar beams were used for planning. A strict quality assurance program was implemented prior to SRS including Lutz′s test for isocentric accuracy before starting treatment. [6] Results Stereotactic frame was fixed, and DSA was performed in all 23 patients of AVM planned for SRS. In two patients, no clear-cut nidus was located on the DSA and thus further procedure was not carried on. Mean age was 20.1 years (range 9-39 years); 12 patients were male and 11 female [Table - 1]. The mean duration of symptoms was 11.9 months. Nine (39%) cases had headache as a presenting symptom, while 21.7% (5) had generalized seizures, and an equal number presented with hemiplegia. History of a neurological deficit before SRS was present in 43.5% (10) patients. A CT scan showed hemorrhage in 65% (15) of cases. In a majority, the nidus of AVM was seen in the cerebral cortex (56.5%; 13 cases). In 56.5% (13) of cases, the nidus had arterial supply from anterior circulation [Table - 2]. A total of 74% (17) of AVMs drained into deep circulation, while only 26% (6) had superficial venous drainage. All cases were Spletzer-Martin grade II/III and AVM scores < 2.5. [AVM score= (0.1 Χ AVM volume in ml + 0.02 Χ age in years + 0.3 Χ AVM location); AVM location: 0 = frontal/temporal; 1 = parietal/occipital/intraventricular/cerebellar/callosal; 2 = basal ganglia, thalamus, brain stem]. [7] Pre-SRS embolization was done in 47.8% (11) cases while 52.2% (12) had no prior embolization [Table - 3]. Embolization was done once in seven patients, twice in three patients, and three times in one patient. Most of the embolizations were done with glue (81%, 9 cases), while only two cases (19%) had onyx embolization. Patients at the time of SRS had definite residual AVMs after embolizations. The mean number of beams used was 8 (range 6-10). The mean nidus volume was 3.65 cc (SD 1.64; range 1.13-5.65 cc) [Table - 4]. The mean prescribed maximum dose was 22 Gy (SD 3.76; range 16-27.5 Gy) while the mean marginal dose was 19.24 Gy (SD 3.16; range 14.4-25 Gy). Mean 12 Gy normal brain volume was 8.39 cc (SD 4.21; range 3.3-15.29 cc) and mean 12 Gy marginal volume was 5.03 cc (SD 4.43; range 0.37-9.64 cc). The mean 87.5% isodose (range 80-91%) corresponded with the mean marginal dose. Mean dose to brain stem, PHA, and optic chiasm was 2.5 Gy (range 0.48-6 Gy), 0.72 Gy, and 0.49 Gy (range 0.48-0.5 Gy), respectively. The median follow-up was 22 months (range 1.5-71.2 months) [Table - 3]. At the last follow-up, 20 patients had no neurological deficit and 3 had a residual neurological deficit. Eighteen patients completed 1.5 years of follow-up and underwent a check MRA. All of them showed complete obliteration yielding an MRA obliteration rate of 100%. Twelve patients out of 18 also underwent DSA to confirm the MRA findings [Figure - 2]. Among the 12 cases, 11 patients had DSA-documented complete obliteration of the AVM nidus and one patient had a persistent small, residual nidus on DSA. Thus, the accuracy of MRA in detecting obliteration of AVM was 92% (compared to DSA which is considered the gold standard). Six patients are due for DSA at 2 years. One patient immediately after SRS had a mild headache, which completely resolved with conservative management. One patient after SRS had a transient deterioration of motor power 6 months after SRS, which resolved completely after a short course of steroids. Another patient had a mild deterioration of the residual hemiparesis, which however stabilized after an intense rehabilitation regimen. No other patients had permanent symptomatic sequelae related to SRS. All patients are leading an active, functional life. Discussion AVMs are developmental malformation of the arteriovenous system. They are usually asymptomatic but when symptomatic present with intermittent episodes of headache and seizures. Major complication of AVMs because of their fragile walls is bleeding and its consequent effects. The aim of treatment is to prevent bleeding. The lifetime risk of hemorrhage from AVMs is 40% while the annual rate of hemorrhage is 2-4%. [8],[9],[10] After the first episode of bleeding, there is a higher risk of subsequent bleeding up to 6%. [11] Interestingly, smaller AVMs bleed more often than larger ones due to higher turbulence in their blood flow. [11] However, smaller AVMs may have spontaneous regression. [11] Treatments with surgery, embolization, or SRS are also not devoid of complications. [12],[13],[14] There is a controversy whether to treat AVMs and accept risk of any treatment or to observe and treat them only in the case of bleeding. In consensus, AVMs with a prior history of bleeding are always treated with suitable modality. AVMs in critical areas of brain with a higher probability of a neurological deficit are treated even if asymptomatic while asymptomatic AVMs in "safe" region are observed. [12] Management of AVMs should be multimodal involving specialties of neurosurgery, neuroradiology, interventional radiology, and radiation oncology. Success of AVM treatment has to be carefully analyzed and patients need to be followed up meticulously. Data should be presented in a consecutively treated patients fashion in order to avoid selection biases. That the risk of bleeding, the chief endpoint of success/failure is small even in an untreated AVM mandates analysis of all treated patients over a period of time with clear outcome measures such as neurological status and check imaging procedures. In the last 7 years at our center, 87 AVMs unsuitable for surgery or those failed to obliterate after embolization were referred for SRS. Each case was discussed at the joint meeting with consultations from neuroradiologists, interventional radiologists, and neurosurgeons. Cases were selected for SRS after a detailed review and fulfilling the predefined criteria. In all selected SRS cases, AVMs had a diameter < 3 cm and were located in a critical site making them unsuitable for surgery. The AVM score was calculated for each case and SRS was considered only if the AVM score was less than 2.5. After SRS, patients were regularly followed up and check imaging was done after 1.5-2 years of follow-up. We performed a relatively non-invasive procedure of MRA initially to check the obliteration of AVMs. Encouragingly, all 15 patients who completed the initial MRA at 1.5-2 years showed no evidence of AVMs yielding a complete MRA obliteration rate of 100%. However, the gold standard of success of SRS "cure" is determined by a DSA and therefore DSA was part of the protocol for all such patients. Out of 12 patients who agreed to undergo DSA, 11 confirmed complete obliteration yielding DSA complete "cure" of 92.5%. The accuracy of MRA to predict the AVM nidus has been estimated to be between 80 and 100% and our figure of 93% corroborates with these findings. The only patient who did not show complete obliteration had a nidus in the region of basal ganglia with a volume of 2.93 cm. In view of relative proximity to a critical location, a marginal dose of 14.4 Gy and maximum dose of 16 Gy was delivered. The patient was considered for SRS as the lesion was unresectable and had a history of bleed with a neurological deficit before SRS. This patient received a relatively less marginal dose, and possibly explains the failure. While MRA revealed complete obliteration, there was a small residual on DSA, although reduced in size as compared to the original pre-SRS volume. We have therefore taken this case as a failure at this point of time, as she still harbors a risk of hemorrhage. She may well show further response in future and will have a repeat imaging after 1 year. Six patients in our SRS-treated series have yet to complete an initial phase of 1.5-2 years before they will be eligible for a check MRA with DSA confirmation. All our patients tolerated the procedure very well. The senior author (RJ) fixed the frame in all patients, including children. Patients were discharged the following day and there were no immediate complications and no patient received corticosteroids routinely. Only one patient had a mild headache a few days after SRS, which resolved with conservative management. Seven out of 10 patients, who presented with a neurological deficit showed complete recovery on follow-up. Many of these patients had a deficit in view of hemorrhage, and the recovery of the deficit could well be due to resolution of the bleeding. All these patients were put on an intensive rehabilitation program in our unit overseen by our occupational therapist. That they did not show any deterioration following the SRS was encouraging. Only one 27-year-old male patient had a mild deterioration of a neurological deficit in the form of slight worsening of his existing hemiplegia. He had a residual AVM nidus postpartial excision in the right frontoparietal region. After SRS, this patient had gradual aggravation of the neurological deficit. The marginal dose was 20 Gy and the maximum prescribed dose was 22.2 Gy. The patient is on a rehabilitative regimen and has not shown any further progression of his hemiparesis. Patients in our series not qualifying for the SRS protocol were referred for surgical resection if AVMs were found in a noneloquent area and deemed to be safely resectable. Patients with large AVMs, especially in eloquent areas and carrying a high risk of post-SRS morbidity were either observed or reconsidered for embolization/surgery. Complete excision of a cerebral AVM eliminates any future risk of hemorrhage and is curative. [13] For small and medium AVMs, even those deeply situated or adjacent to critical areas and larger AVMs located in silent areas, the mortality of surgery is about 10%. In a series considering only microsurgical resection of small AVMs (< 3 cm in diameter), the rates of morbidity and mortality were as low as 1.5% and 0%, respectively. [13],[14] The chief advantage of surgery is that patient is cured instantly. However, in large AVMs with deep extension, located in or adjacent to critical areas, the rate of serious morbidity may reach as high as 50%. [13] Such a morbidity rate is considered unacceptable and surgery in these cases should be considered only in carefully selected cases. In our case series as well, many patients, after discussion in the Joint NeuroOncology meeting, having an AVM amenable for surgical resection were referred back. The goal of endovascular embolization is complete occlusion of AVMs. [15] Occlusion rate of endovascular embolization as the sole treatment modality has been reported to be ranging from 0 to 20%, with an average of only 5%. [15],[16] In incompletely obliterated AVMs, late recurrences are reported with a higher probability of bleeding. True recanalization may even occur weeks to months after complete occlusion. An AVM after embolization is considered completely obliterated only if obliteration is documented 1 year after the procedure. [15] SRS has always been considered as a valid treatment modality for AVMs. Though SRS is said to be a "non-invasive" procedure, single-fraction high-dose radiation may cause similar damage to the normal brain as occurs in invasive neurosurgery, and hence many consider SRS as an invasive procedure. [1] Outcome of radiosurgery for cerebral AVMs has always been assessed after a 2-year follow-up with repeat DSA. In smaller AVMs (< 3 cm diameter), the obliteration rate is between 80 and 100%, with a marginal dose of 20-25 Gy. Morbidity rates are between 2 and 4%, and the mortality rate between 0 and 1%. [14] However, in larger AVMs (>3 cm diameter), the obliteration rate ranges from 30 to 60%, with a dose of 15-20 Gy and a long-term complication probability of 20-30%. [17] A higher obliteration rate could be obtained with a higher radiation dose (25-45 Gy), but with a higher complication rate (~50%). [17] In the Pittsburg series, 944 AVM patients treated with SRS, symptomatic, postradiosurgery sequelae were observed in 85 (9%) cases of which in 38 (4%) cases, a temporary neurological deficit was seen, while a permanent neurological deficit was seen in 47 (5%) cases. [5] However, this series had a heterogeneous patient population with larger AVMs and only a small percentage was situated near critical structures like brain stem and thalamus. It is the late effect of radiation that is responsible for the obliteration of the nidus. Thus, there is a latency period of 1.5-2 years between SRS procedure and obliteration of the nidus. During this period of latency before complete obliteration, the rate of hemorrhage is identical to the natural history (3-4% per year). [1] Thus, SRS has no protective effect before complete obliteration of the AVM. Though rare, spontaneous resolution of AVMs may be seen if there is a sufficient gap between the diagnostic DSA and pretreatment DSA. In our series, two DSA-proven residual AVMs obliterated spontaneously on pretreatment DSA. Thus with SRS, obliteration of the malformation takes time, it is not always successful, carries a risk of hemorrhage during the period of latency, there is a risk of late radiation-induced brain injury, and the obliteration rate is entirely dependent upon proper selection of cases. [18] There are mature data regarding both the obliteration rate and complication. [5],[14],[18] However, there are very few publications from India regarding the outcome of AVMs treated with SRS. [19],[20] Since a detailed, prospective analysis of AVMs treated with SRS is lacking from this part of the world, our report may well be among the first few detailing outcome data. We are conscious of the fact that our data are based on a relatively small number of patients. However, all patients in this analyzed cohort have shown an excellent response so far in terms of obliteration, tolerance, and favorable toxicity profile. Our initial experience has justified the robustness of the carefully defined pre- and posttreatment protocols and a multidisciplinary decision-making process and management approach and will continue to accrue patients on this protocol for more mature results in a larger patient population. Conclusions In summary, SRS is a viable and safe option in the management of small AVMs. Stringent case selection provides acceptable obliteration rates with minimal long-term toxicity. Acknowldgments We are grateful to all colleagues in the Departments of Radiation Oncology, Medical Physics, and Radiology in TMH and Departments of Neurosurgery and Interventional Radiology for patient care and supporting this work. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09046f1.jpg] [cr09046t4.jpg] [cr09046f2.jpg] [cr09046t3.jpg] [cr09046t2.jpg] [cr09046t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}