 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
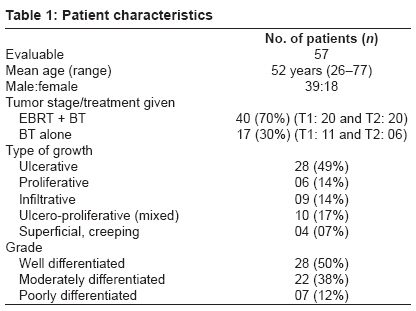
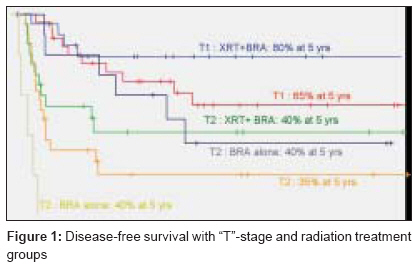
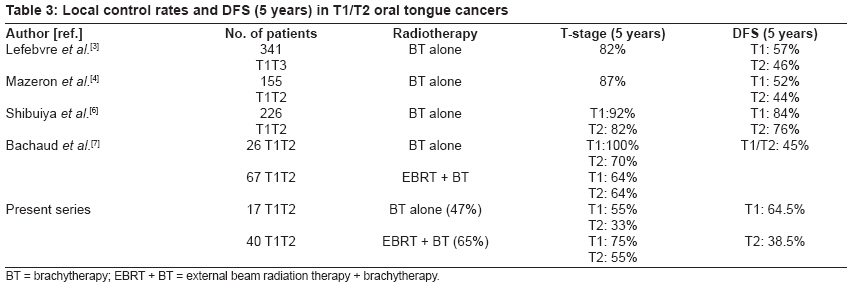
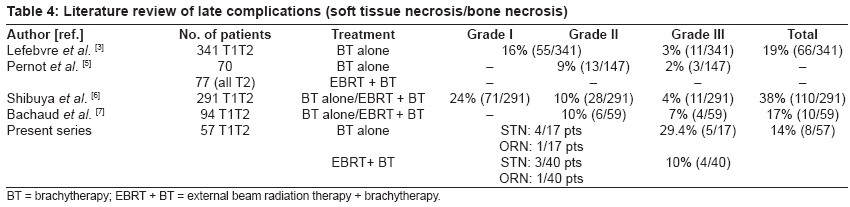
Journal of Cancer Research and Therapeutics, Vol. 5, No. 3, July-September, 2009, pp. 192-197 Original Article Treatment outcome with low-dose-rate interstitial brachytherapy in early-stage oral tongue cancers Bhalavat Rajendra I, Mahantshetty Umesh M, Tole Sanjay, Jamema Swamidas V Department of Radiation Oncology, Tata Memorial Hospital, Mumbai Code Number: cr09047 PMID: 19841561 DOI: 10.4103/0973-1482.57125 Abstract Purpose : Although radical radiotherapy is known to be equally effective for early-stage oral tongue cancers (T1-2 N0) with the added advantage of organ and function preservation, surgery remains the preferred treatment. We present outcome of patients treated with brachytherapy (BT) either radical or boost.Materials and Methods : Fifty-seven patients (T1/T2 31/26) were studied. Seventeen patients (30%) were treated with radical BT (50-67 Gy) while 40 (70%) with external beam radiation therapy (EBRT) + BT (36-56 Gy + 15-38 Gy]. Low-dose-rate (LDR) BT was delivered with 192 Ir wires, using plastic bead technique with varied dose rates (<60 cGy/h in 29 patients, 60-90 cGy/h in 17, and >90 cGy/h in 11). Results : The overall local control (LCR) was achieved in 59.7% (34/57) patients. LCR for T1 and T2 was 67.8% and 50%, respectively. A total of 23 patients had failures [local: 20 (T1: 8; T2: 12 patients), node: 5 (T1:2; T2: 3), and local + nodal: 3]. Overall 5-year disease-free survival and overall survival (OAS) were 51% and 67%, respectively and those for T1 and T2 was 64.5/77.4% and 38.5/54% respectively (P = 0.002). All 16 patients were salvaged. Median survival after salvage treatment was 13.5 months (6-100 months). Soft tissue necrosis was observed in 12.3% (7/57) and osteoradionecrosis in two patients. Conclusion : BT, as an integral part of radical radiation therapy in early-stage tongue cancers, appears to be an effective alternative treatment modality with preservation of the organ and function without jeopardizing the outcome. Keywords: Oral tongue cancers, low-dose-rate brachytherapy, osteoradionecrosis, soft tissue necrosis Introduction Partial glossectomy with or without neck dissection has been the standard approach for early-stage mobile tongue cancers. Radiation therapy has been used as an alternative treatment although disease control rates with surgery or radical radiation therapy in early-stage squamous cell carcinoma of oral tongue are equal. [1],[2] Surgery is associated with the impaired speech, deglutition and increased morbidity, and cosmetic defect resulting from neck dissection. Radiation therapy has evolved over the last two to three decades with better therapeutic index and organ and function preservation strategies. One such advance has been the use of brachytherapy (BT). BT in oral tongue has the advantages of delivering high doses with reduction in doses to surrounding critical structures, thereby reducing the toxicities of external radiation alone. However, BT has not yet made a positive impact in the management of early-stage oral tongue cancers. [3],[4],[5],[6],[7] Radiation-induced xerostomia and osteoradionecrosis (ORN) are cited reasons in favor of surgery. At the Tata Memorial Hospital, Mumbai, India, head and neck cancers account for 26% (approximately 4000 cases) of all cases registered, of which oral tongue cancers constitute < 10%. The hospital is surgically oriented hence most cases are preferentially treated by surgery. In an attempt to evaluate the impact of BT on locoregional control, survivals, and complications, we undertook this retrospective analysis of patients with early-stage mobile tongue cancers, treated with BT (radical or boost). Materials and Methods Between January 1988 and December 2002, 57 T1/T2 N0-1 oral tongue cancer patients with biopsy-proven squamous cell carcinoma treated with BT either alone or in combination with moderate dose EBRT were analyzed. Patient characteristics were as shown in [Table - 1]. Radiotherapy Details Out of 57 evaluable patients, 17 (T1: 11 and T2: 6 patients) underwent radical BT and 40 (T1: 20 and T2: 20 patients) patients EBRT + BT. Patients with relatively small lesions, proliferative, and limited to the lateral border irrespective of T1/T2 were treated with radical BT. In the initial period, T2 patients were selected for radical BT but with passage of time and better understanding of the disease, radical BT was restricted to T1 only. The BT procedure involved insertion of plastic tube catheters in the desired area under general anesthesia. The technique used has been described and published elsewhere. [8] The technique used is a modified one and uses plastic bead/s with two slits (instead of buttons) at the surface end. One of the ends is sealed with plastic tube and through the other passes a crossing tube, brought forward from posterior line/s, to cross all anterior tubes in each plane. [8] Double-plane or volume implant was done depending upon the T-stage and extent of the disease. Lengths of the wires to be loaded were determined from orthogonal films. Generally, loading from lower end is done 5-10 mm away from skin, so as to reduce skin and subcutaneous doses. Computer dosimetry was done using orthogonal anterolateral simulation films with radio-opaque dummies. Dose/dose rate was prescribed according to the rules of the Paris system. [9] 192 Iridium wires of uniform activity ranging from 0.5 to 1.33 mCi/cm were used to deliver LDR BT in 2-7 days. BT was delivered with 192 Ir LDR system with a mean dose rate of 65 cGy/h (30-130 cGy/h). Corresponding biological equivalent dose, i.e., BED was calculated for each group and stage. In the radical BT group (17 patients), a mean dose of 58.1 Gy 50-67 Gy was delivered in 3-7.5 days (mean 5 days). None of the patients in this group underwent neck dissection to address the nodes. A double-plane implant was carried out in 11 (T1: 8 and T2: 3) patients and remaining 6 (3 each for T1 and T2) had a volume implant. The mean total dose in BT alone group for T1 and T2 was 58 50-67.5 and 58.25 51-67.3 Gy, respectively. The mean total BED dose was 64.5 Gy median: 64.8 Gy; range: 53.7-77.8 In the EBRT + BT group, patients initially received external radiation followed by BT boost. EBRT was delivered using 60 Co -unit to the target volume that included the primary with adequate margin (clinical target volume I) and upper neck to include level II/III nodes (clinical target volume II) by either bilateral or ipsilateral anterolateral standard ports. Usual external radiation and BT dose intended for T1 was 46 Gy ± 4 Gy plus 25 Gy ± 5 and for T2 was 50 Gy ± 4 Gy plus 35 Gy ± 5 respectively or its equivalent using different fractionation/dose rates matched for a biologically equivalent dose. Twenty-nine patients were treated with bilateral ports while the remaining 11 with ipsilateral anterolateral ports. The spinal cord was spared after 44 Gy. Twelve patients received an EBRT dose of < 40 Gy, 21 patients 40-50 Gy, and 7 received more than 50 Gy with mean: 46 Gy (30-60 Gy) @ 2 Gy/# 26-37 days. BT boost after external radiation therapy was performed after a median gap of 21 days (4-46 days). BT boost using the double-plane implant was given in 25 cases (T1: 10 and T2: 15) while 15 patients were treated with the volume implant (T1: 10 and T2: 5). BT boost was given as described above and the dose decision was made in relation to the T-stage, EBRT dose, post-EBRT residual disease and dosimetry (specific activity and relevant dose rate on the day of implant) keeping the total dose (EBRT + BT) as 75 Gy ± 3 (mean dose 71) for T1 and 85 Gy ± 3 (mean dose 72.74) for T2. Of these 40 patients treated with BT boost, 28 patients received 20-30 Gy, 6 patients 30-40 Gy, and 6 patients less than 20 Gy. The mean dose was 27 Gy (1540 Gy). The dose rate was different on the day of implant, and depended upon the specific activity (0.5-1.33 mCi), so -22 patients were treated with a dose rate of < 60 cGy/h, 13 with 60-90 cGy/h, and remaining 5 with> 90 cGy/h. The mean total equivalent BED for T1 and T2 was 76.4 and 80.9 Gy range: 57-93 and 53.5-97.2, respectively. Statistics Survival rates were computed from the date of starting radiation therapy (external radiation or brachytherapy whichever first) using SPPS software, version 10. Nontime events were compared using the chi-square test. Survival curves were obtained using the Kaplan-Meier method with the log-rank test for statistical significance for comparison. [10] Results With a mean follow-up of 93 months (median: 64 months; 3-136 months) for the whole group, 93 months (median: 68 months; 3.5-136 months) for the EBRT + BT group, and 69 months (median: 60 months; 3-96 months) for the BT group, 20 patients had local failure (T1: 8; T2: 12 patients), 5 only nodal (T1: 2; T2: 3 patients), and 3 local + nodal failures (T1: 2; T2: 1 patient). One (T1 lesion) patient treated with EBRT + BRT developed metachronous 2 nd cancer in the penis. [Table - 2] shows the details of patients with recurrence according to the stage and treatment given. Eleven out of the 23 patients with a component of local failure had persistent disease while the remaining 12 developed recurrences within 7-154 months (seven patients (4/3, T1/T2) had recurrences within 12 months while the remaining five developed recurrences at 34, 46, 50, 57, and 154 months of completion of treatment). The overall local control rate (LCR) at 5 years was 59.7% 34 / 57. Similarly, it was 67.8% (21/31) and 50% 13/26 at 5 years for T1 and T2 lesions, respectively. LCR in the EBRT + BT group for T1 versus T2 was 75% 15/20 versus 55% (11/20) (whole group: 65%) and the same in the BT alone group was 55% (6/11) versus 33% (2/6) (whole group: 47%), respectively. The median duration for locoregional failures was 26 months (range of 2-154 months). Salvage Therapy Out of 28 failures, 21 underwent salvage surgery, 2 reirradiation (1 each in the BT and EBRT + BT group), 1 surgery plus implant, 1 underwent palliative chemotherapy, and 10 patients were lost to the follow-up (3 patients after recurrence and 7 patients after salvage treatment within 6 months). Three of five nodal failures underwent salvage radical neck dissection (RND) (T1: 2; T2: 1) with two receiving postoperative radiation later. All the three patients with local + nodal failures underwent salvage surgery (T1: 2; T2: 1 patient) were salvaged, of whom 1 patient with T1 lesion developed lymphangitis carcinomatosis and bony metastasis and died 28 months after surgery. The patient with metachronous 2 nd cancer in the penis underwent partial amputation and was controlled at the last follow-up of 100 months. Median survival after salvage therapy was 13.5 months (6-100 months). Out of 25 undergoing salvage therapy, only 16 patients had favorable outcome, were salvaged (8 of 12 in the T1 group, with 5 patients surviving > 3 years and 8 of 16 in T2, with only 3 patients surviving > 3 years). Complications were graded according to the RTOG toxicity criteria retrospectively. [11] There were no BT-procedure-related complications reported. After the completion of BT treatment, one patient had profuse bleeding (blood loss of 200 ml) during implant removal, which was controlled by simple bidigital compression and conservative treatment. In the EBRT + BT group, acute grade II radiation skin toxicity (in the form of extensive pigmentation, dry desquamation) and mucositis (in the form of moderate fibrinous mucositis) were seen in 60% (24/40) patients, while the acute grade III radiation skin toxicity and mucositis were seen in 10% (4/40) following external radiation and took longer time (6-12 weeks) to subside. Although there was no skin toxicity (except at the puncture site) in the BT alone group, patchy fibrinous mucosal reaction (grade I/II) was seen in nearly all patients, and grade III mucositis in 47% (8/17) patients, which took almost 6-10 weeks to subside with routine conservative management. Late cutaneous and subcutaneous fibrosis in the submental region and neck was seen in 14% 8/57 patients. Soft tissue necrosis (STN) was observed in 12.3% 7/57 (5 for T1 and 2 for T2) patients with 4 in the radical BT and 3 in the EBRT + BT treatment group. Three in the combination group received total a BED of> 80 (80, 83, and 91) whereas four from the BT alone group received a BED of 57, 66, 69, and 71, respectively. Two of the 57 developed ORN, 1 in the BT alone and 1 in the combination group. One patient in the BT alone group who also showed STN received a BED dose of 71 and one in the EBRT + BT group received 48 + 30 (E + B) equivalent of a total BDE of 79.7. Incidentally, 2/7 STN and 2/2 ORN (one with STN + ORN) received 15-20 % higher doses. This was due to boost to overcome peripheral underdose at lateral margin of tongue and higher dose rate of 100 cGy/hr. The additional 15-20% extra dose delivery to compensate for lateral underdosage was at the discretion of the treating physician and on individual case basis. Moreover, in our series, majority of our patients (88%) had lateral border tongue lesions while the remaining had lesions on the dorsum of the tongue. Perhaps this (correction overdose) might have also contributed to STN/ORN. A patient with ORN/STN (10 months post-BT) was salvaged by marginal mandibulectomy, and is alive and disease free at 6 years. Another patient with ORN underwent debridment sequestrectomy. Six of the seven with STN were no evidence of disease and alive while one died of other cause. While 4 of 17 (24%) of the BT alone group showed STN and/or ORN, only 4 of 40 (10%) showed STN in the EBRT + BT group. Noteworthy, the higher dose improved LCRs but was associated with an increased risk of STN/ORN, suggesting a need for an optimum implant geometry and dose prescription to avoid hot/cold dose regions. Although the mucosa looked moist during follow-up, xerostomia of mild-to-moderate degree was observed in 17.5% 10/57 patients. Survivals The 5-year disease-free survival (DFS) and overall survival (OAS) for the whole group were 51% and 67%, respectively. Local DFS was significantly better for T1, 64.5% versus 38.5% for T2 at 5 years (P = 0.002). Local DFS was significantly better with EBRT + BT than BRT alone irrespective of the T-stage with P = 0.000 [Figure - 1]. Other prognostic factors like grade, type of lesion, dose rate, and dose had no significant bearing on the DFS. Median survival after salvage for T1 in both the groups (BT and EBRT + BT) was 25 months (6-80 months) and the same for T2 was 6 months (3 -60 months), respectively. Discussion Partial glossectomy or hemiglossectomy (HG) with or without neck dissection has been the standard approach for early-stage mobile tongue cancers. Radiation therapy has been used as an alternative treatment although disease control rates with either therapy in early-stage mobile tongue cancers (T1/T2) are equal. The choice of treatment depends on the availability of the particular expertise required and of the surgeon or radiation oncologist, and the functional and cosmetic results of treatment for each individual patient. [1],[2] Both surgery and radiotherapy treatments have advantages and disadvantages. Surgery has high local control rates but poor nodal control rates while radiotherapy has higher nodal control rates but lower local control rates. Radical surgery is associated with morbidity of the cosmetic defect of face/neck, removal of organ, and need for general anesthesia, often twice. Radiotherapy has the advantage of organ preservation but it is not preferred, because of late toxicity in terms of xerostomia and its consequences. BT in oral tongue cancers has the advantages of delivering high doses with reduction in doses to surrounding critical structures (i.e., salivary gland), thereby reducing the toxicities of external radiation alone. In an attempt to evaluate the role of BT in early-stage oral tongue cancers, we undertook this retrospective analysis. Local control is a reflection of "T"-size / stage of the primary tumors. Wide excision is replaced by partial glossectomy or HG for better LCRs. In the present series, LCRs at 5 years were 47% for the BT alone (T1 vs. T2: 55% vs. 33%) and 65% for the EBRT + BT T1 vs. T2: 75% vs. 55% group. With surgery, LCRs vary from 75% to 90% and DFS ranges from 62% to 95% depending upon the tumor site and size. [1],[2] Fakih et al. reported 1-year LCRs of 52% for HG (T1 vs. T2: 64% vs. 46%) and 63% for HG + RND (T1 vs. T2: 70% vs. 60%). [2] In the present series, the results of EBRT + BT (combination RT) are comparable to "HG + RND" for T1 and T2 tumors, i.e., the LCR, DFS, and OAS are similar. However, the same is not true for the BT alone group. Although the use of BT alone seems to be the best treatment option for the preservation of organ/anatomy and even function (since it prevents or lessens radiation to salivary gland/s), the LCRs 55% (6/11) for T1 and 33% (2/6) for T2 in this group are inferior to those for surgery. The reasons for the poor outcome with BT alone have been addressed subsequently. It should be emphasized here that the radiation oncologist has to rely on clinical staging, which is subjective. Moreover, in the present series, decision of choosing BT alone or external radiation and BT boost was solely a clinical evaluation without considering newer imaging modalities. Nodal disease and its control is also an important prognostic factor in the outcome of early-stage tongue cancers. [1] The nodal incidence rate (occult) for T1/T2 lesions which is 6-46% is not only dependent upon the T-size but also on tumor thickness (TT) (a reflection of the depth of infiltration and tumor volume). Higher the TT, greater the nodal failure (irrespective of its size), with the nodal failure 50% or more when TT> 4 mm. [2],[12],[13] Similarly, in another series, the nodal failure rates were significantly (P = 0.007) higher (8% vs. 51% when TT> 5 mm. [14] Thus, following surgery, the exact pathological stage, local tumor details, like thickness, extent of mucosal and soft tissue involvement, and the accurate assessment of the level, extent, and number of regional lymph nodes, which are important prognostic factors are available to surgeons. All this information remains obscured for the treating radiation oncologist. Neck relapse thus remains the main hurdle after HG or wide excision alone, despite high LCRs. [2],[7] Nodal failure, a problem with surgical treatment, is not seen when treated by radiotherapy. A growing need for nodal dissection, either RND or modified neck dissection (simultaneous or subsequent) as a part of radical treatment (to achieve greater DFS), has made HG + ILRND [(ipsilateral RND (sequential or simultaneous)] a gold standard, while dealing with surgical management (of course with increase in morbidity and poor cosmesis) depending upon the depth of invasion. [2] Addressing the neck with simultaneous/sequential RND although lowers the ipsilateral neck relapse, but is countered by an increased risk of neck relapse in the contralateral neck [2] (i.e., supraradical treatment has also limitations). On the other hand, external radiation therapy (combination group), has the advantage of treating the neck nodes, lymphatics along with the primary without much added morbidity. The nodal control rate for N0/N1 disease with radiation is reported to be between 90 and 96% and in the present series, it is 92.5% (37/40 patients) [even with a moderate-dose EBRT (median 46 Gy; range 36-54 Gy)]. [15] Moreover, one of the three patients with nodal failures received 40 Gy/20# (1/12, i.e., 12.3%) only, while other two received a dose of 54 and 56 Gy (2/28, i.e.,7.1%). It may be worth noting that patient who received 40 Gy and had nodal failure, had a poorly differentiated tumor. He later developed lymphangiocarcinomatosis and bone metastasis and succumbed to the disease at 28 months. Thus, the external dose used for the combination treatment is large enough to sterilize N0 and, for that matter, even N1 disease in the neck. All the nodal failures were seen in patients treated with bilateral portals (29 patients) and none in those treated with anterolateral portals (11 patients), either on the same or on the contralateral side. A total of 7 out of 11 (16/29) were NED/controlled when last seen. Two other nodal failures were seen in the BT alone group, one each in T1 and T2. The results of EBRT + BT are as good (if not better) as HG + ILRND but with an added advantage of organ and function preservation and better cosmesis. Also, HG + ILRND have not translated into better survival rates because of higher subsequent contralateral nodal relapse (up to 25%). Contralateral neck nodal failure, seen following surgery, is less often seen with EBRT + BT, possibly because external radiation is usually given with bilateral portals which invariably sterilize contralateral neck nodes too. [2] An anterolateral portal with wedges is planned for a small and well-lateralized lesion and the anterior portal in such cases extends beyond the midline and covers whole oral tongue, and as a result whole submental region of the neck receives full dose. In our series of the EBRT + BT group, none of the patients had contralateral neck nodal failure (treated with the bilateral and antero-lateral portal: 29 and 11). The literature has reported DFS and LCRs of 62-95% and 75-90%, respectively, with surgery. [1],[2],[12] Overall DFS reported by Fakih et al. was 52% at 3 years for HG (T1 vs. T2 was 64% vs. 46%) and 63% for HG + RND (T1 vs. T2 was 70% vs. 60%). [2] Fakih et al. have also reported a high incidence of contralateral neck relapse (25%) in patients who have undergone ipsilateral neck dissection as primary treatment, ultimately leading to decreased OAS survivals. In our series, DFS in the EBRT + BT group at 5 years for T1 vs. T2 was 75% versus 55% which is comparable to that reported in the literature (for surgery or external radiotherapy). Similarly, DFS for the BT alone group in the present series was 55% versus 33% at 5 years for T1 and T2 respectively which is inferior to that reported in the literature [Table - 3]. [3],[4],[6],[7] This could be explained by the fact of all these patients being clinically staged, no imaging done for staging, and personal bias in the decision-making process of radical BT. Acute complications during EBRT and post-BT are understandable and are well within acceptable limits. Late grade III complications of soft tissue/bone necrosis of 14% in our series is comparable to reported literature of 3-15% with radical BT. [4],[6],[7],[8] Despite the shortcomings detailed in the "Introduction," interstitial BT (radical or boost) has achieved comparable "local control rates" and "reduction in the morbidity." Also despite low LCRs, overall survival with radical radiation therapy is comparable with the world literature (surgery) with an added advantage of preservation of organ and function but at the expense of acceptable morbidity of STN and/or ORN. The present study with use of BT (radical or boost) for early lesions has reduced the overall complications of radiation, i.e., STN to 14% (10% (4/40) and 23% (4/17) respectively in the EBRT + BT group and the BT alone group)) and ORN to without compromising on the control and survival rates which is comparable to that reported in the literature [Table - 4]. [3],[5],[6],[7] An inverse planning with an ability to spare adjacent alveolus may be able to curtail the dose to bone and thereby reduce chances of ORN. The xerostomia of mild-to-moderate degree (mostly adjusted with routine activity with no complains as such) was seen in 17.5% on specific inquiry in those, on follow-up. There seems no argument with respect to salivary preservation when treated by radical BT but the question will be raised for combination treatment. There is recovery of salivary function if the dose to any salivary gland is limited to < 40 Gy. [16] At present, to overcome all the pitfalls mentioned earlier, we are working on the following areas to improve the therapeutic ratio:
Conclusion Although this is a personal experience and a retrospective study, these results are noteworthy, considering its long follow-up and the outcome both in terms of LCRs and toxicities. Addition of BT results in acceptable local, locoregional control and survival rates for T1 and T2 oral tongue cancers with advantages of organ preservation and reduction in complication rates, especially xerostomia associated with radical external radiation. Hence, we recommend a combination of external radiation and BT boost for early-stage, operable oral tongue cancers, and radical brachytherapy to be reserved only for very small proliferative lesions. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09047t2.jpg] [cr09047t1.jpg] [cr09047t4.jpg] [cr09047t3.jpg] [cr09047f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}