 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
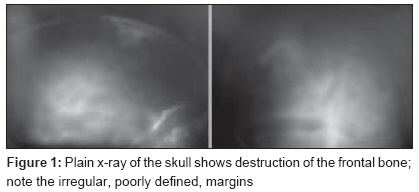
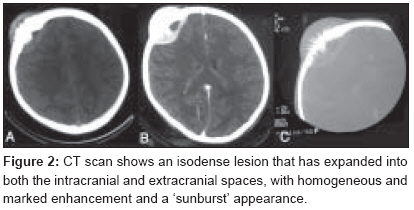
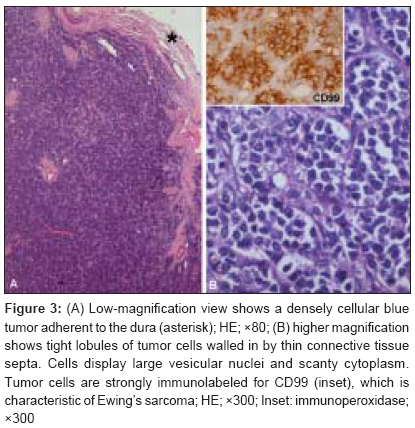
Journal of Cancer Research and Therapeutics, Vol. 5, No. 3, July-September, 2009, pp. 208-209 Case Report Primary Ewing's sarcoma of the frontal bone with intracranial extension Agrawal Amit, Dulani Rajesh, Mahadevan Anitha, Vagaha SJ, Vagha Jayant, Shankar SK Department of Surgery, Datta Meghe Institute of Medical Sciences, Sawangi (Meghe), Wardha Code Number: cr09051 PMID: 19841565 DOI: 10.4103/0973-1482.57129 Abstract Primary Ewing's sarcoma arising from the skull is extremely rare. We report a case of an 11-year-old male child with primary Ewing's sarcoma of the frontal bone with intracranial extension. We also discuss the imaging and intraoperative findings and describe our use of a split calvarial graft in the present case.Keywords: Cranium, calvarial graft, cranioplasty, Ewing′s sarcoma, frontal bone, intracranial Introduction Primary Ewing′s sarcoma arising from the skull is an extremely rare lesion. [1],[2],[3],[4],[5] We report a case of primary Ewing′s sarcoma in a child that involved the frontal bone and had intracranial extension. We also present a review of the relevant literature. Case Report An 11-year-old male child presented with progressively increasing and painful swelling over the right frontal region of 3 months′ duration. The mass was detected incidentally after he had a fall. There was no history of headache, fever, vomiting, seizures, or any focal deficits. Local examination revealed a hard and tender right frontal mass with prominent vascular markings and healthy overlying skin. His general, systemic, and neurological status were normal. Blood investigations were normal. X-ray skull showed an ill-defined lytic lesion with irregular margins involving the right frontal bone [Figure - 1]. CT scan showed an isodense lesion with bony spicule formation (′sunburst′ appearance); there was intra- and extracranial extension and the lesion enhanced well after contrast administration [Figure - 2]. The patient was planned for wide excision of the lesion. A bicornal incision was made and the tumor, with prominent vascular markings over it, was exposed. A 1-cm bone margin was defined all around the tumor and the bone flap was removed. There was infiltration of the dura. The dura was widely excised, and the dural defect was reconstructed with a pericranial graft. A bone flap of the same size was removed from the left frontal region of the skull and the outer and inner tables were split and used to reconstruct the defect on right side. The tumor was well defined, elastic hard, and involved the bone as well as the dura. The tumor that was infiltrating the brain was also excised. Histological examination of the surgical specimen after hematoxylin-eosin and immunostaining showed a homogeneous population of closely packed small neoplastic cells, with abundant fibrovascular stroma; the cells contained round to oval nuclei and a scanty amount of cytoplasm. There was involvement of bone, dura, and extending intracranially with focal parenchymal invasion [Figure - 3]. The tumor cells were arranged haphazardly without neural or Homer-Wright rosettes. Postoperatively, a course of radiotherapy was given, followed by chemotherapy with a four-drug regimen (vincristine, adriamycin, cyclophosphamide, and actinomycin-D). [6] The child is doing well at 12 months′ follow-up with no recurrence of tumor. Discussion Ewing′s sarcoma usually occurs in the first or second decades of life. There is no predilection for either sex. Involvement of the skull occurs in less than 1% of cases. [1],[2],[4],[6] As in the present case, Ewing′s sarcoma most commonly presents as a painful swelling that enlarges rapidly over a period of a few weeks to a few months. [1],[2],[3],[4] When there is intracranial extension or involvement of neural structures there may be features of raised intracranial pressure as well as focal neurological deficits. [1],[4] On plain x-ray, many patients may show areas of bone destruction with irregular, poorly defined margins. [1],[2],[3] The most common CT finding is an isodense lesion, with marked and heterogeneous enhancement. In contrast to plain x-ray, CT scan can also show the intracranial or extracranial extension of the tumor as well as even slight bone destruction. [7],[8],[9] As in the present case, there may sometimes be spiculated new bone formation, a distinct feature of Ewing′s sarcoma. [7],[8] Magnetic resonance imaging (MRI) will show marked heterogenous signal intensity, with areas of hemorrhage and necrosis. Because of its multiplanar capabilities it will also demonstrate the extent of tumor, which is of great help in surgical planning. [10] CT attenuation and MRI signal characteristics reflects and correlates well with the sheets of densely packed cells as seen in Ewing′s sarcoma. [10],[11] Early diagnosis and radical excision followed by modern chemotherapy and radiotherapy is recommended for the best results. [1],[2],[3],[5],[7] A course of radiotherapy to the residual tumor followed by a four-drug regimen (vincristine, adriamycin, cyclophosphamide, and actinomycin-D) is described to be superior to a three-drug regimen (vincristine, adriamycin, and cyclophosphamide). [6],[12],[13],[14],[15] In summary, a multidisciplinary approach, with a combination of different modalities of treatment (wide surgical excision, radiotherapy, and chemotherapy), has improved the prognosis of Ewing′s sarcoma. This case also illustrates a novel surgical approach to the resection of a frontal Ewing′s sarcoma; we used a split calvarial graft to reconstruct the bone defect, thus avoiding the added cost of an implant. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09051f2.jpg] [cr09051f3.jpg] [cr09051f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}