 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
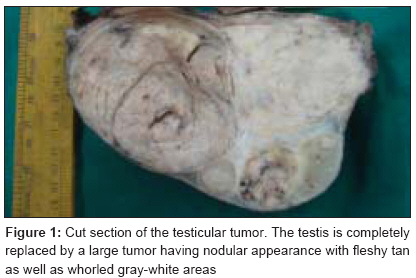
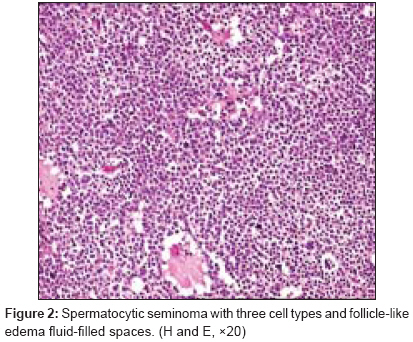
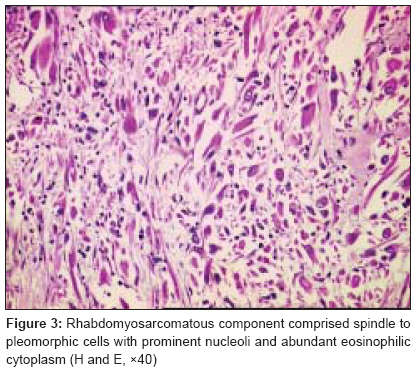
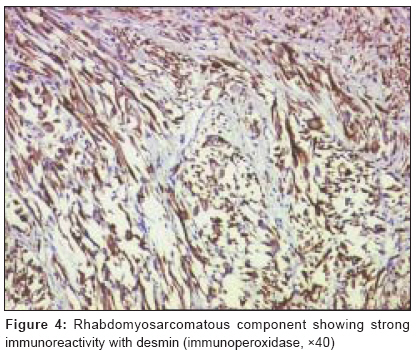
Journal of Cancer Research and Therapeutics, Vol. 5, No. 3, July-September, 2009, pp. 213-215 Case Report Spermatocytic seminoma with rhabdomyosarcomatous differentiation: A case report with a review of the literature Menon Santosh, Karpate Arti, Desai Sangeeta Department of Pathology, Tata Memorial Hospital, Parel, Mumbai-400 012 Code Number: cr09053 PMID: 19841567 DOI: 10.4103/0973-1482.57131 Abstract Spermatocytic seminoma is an uncommon testicular germ cell tumor associated with a favorable outcome. Sarcomatous transformation in a spermatocytic seminoma is extremely rare with only 13 cases being reported in English literature. The presence of a sarcomatous component is associated with an aggressive behavior, metastasis, and poor prognosis. We present a case of a spermatocytic seminoma with rhabdomyosarcomatous transformation in a long-standing testicular swelling in a 55-year-old male.Keywords: Spermatocytic seminoma, rhabdomyosarcomatous differentiation Introduction Spermatocytic seminoma is an uncommon germ cell neoplasm that accounts for 1-2% of all testicular tumors and usually arises in older men with a mean age of 53.6 years (range 19-72 year). [1],[2],[3] Spermatocytic seminoma is an indolent neoplasm characterized by a long duration of symptoms, early stage at presentation, and absence of metastasis. Rarely, its biological course is complicated by sarcomatous transformation [4],[5] which is clinically characterized by a rapid increase in the size of the tumor and propensity to metastasize. [6] Hence, the awareness of this rare occurrence is of utmost importance in planning further patient management. We present a case of rhabdomyosarcomatous transformation in a spermatocytic seminoma in a patient with a testicular mass. To the best of our knowledge, this is the first reported case from India and the 14 th in the literature. [4] Case Report A 55-year-old man had a history of a slowly enlarging, painless right scrotal swelling of 10-year duration. However, since the last 7 months, a progressive increase in its size was noted for which he underwent orchidectomy elsewhere. Clinically, the preoperative diagnosis was of a secondary hydrocele with an underlying testicular tumor. Preoperative radiological investigations and tumor marker evaluation were not done. Postsurgery, he was referred to the genitourinary surgical oncology unit of our institute for further management. Macroscopic findings The right high inguinal orchidectomy specimen submitted at our institute consisted of an enlarged testis, measuring 15.0 Χ 9.5 Χ 8.0 cm. The testicular shape was maintained. On cut surface, the normal testicular parenchyma was completely replaced by a solid tumor composed of varying-sized nodules separated by fibrous septae. Most of the nodules were fleshy, tan colored with foci of hemorrhage and gelatinous change. However, some of the nodules were grayish-white with a whorled appearance and were firm in consistency [Figure - 1]. Light microscopy The tumor was composed of two distinct histologic elements. The predominant component was formed of cellular sheets and nodules of tumor cells with little intervening stroma comprising fine connective tissue strands and edema fluid forming follicle-like spaces and small cystic pools [Figure - 2]. A tripartite cell population of a variable size with small lymphocyte-like, intermediate-sized and large cells, characteristic of a spermatocytic seminoma, were appreciated on closer inspection. The intermediate cells formed the predominant population. The large cells either had a single large nucleus or were multinucleated. The other contingent of the tumor had a sarcomatous appearance characterized by spindle cells dispersed in irregular nodules. The spindle cells closely arranged in short fascicles had an undifferentiated "blue appearance" at places whereas in other areas, they merged imperceptibly with strap-like cells with abundant eosinophilic cytoplasm, round nucleus, and prominent nucleolus consistent with rhabdomyosarcomatous differentiation [Figure - 3]. Intimately admixed pleomorphic cells with irregular hyperchromatic nuclei were also identified. As in usual spermatocytic seminomas, no areas of intratubular germ cell neoplasia (IGCN) or other associated germ cell components were identified. The seminomatous component was largely circumscribed but the rhabdomyosarcomatous component was seen involving and destroying the rete testis and the epididymis. The tunica albuginea was, however, not infiltrated. Lymphovascular emboli were not seen. Immunohistochemically, the spermatocytic component was negative for CD30, smooth muscle actin, c-kit, placental alkaline phosphatase, and alpha-fetoprotein. The rhabdomyosarcomatous element was strongly positive for desmin [Figure - 4] and weakly for myoglobin. The undifferentiated spindle cell component was positive only for vimentin. Discussion Spermatocytic seminoma is a relatively rare but well-defined pathologic entity, first described by Masson. [7] The usual age at diagnosis in the case of spermatocytic seminoma is 50 years in comparison to 30-40 years age of presentation of classical seminoma. Clinical presentation is usually in the form of a painless testicular swelling or long-standing hydrocele. The duration of symptoms as documented in the literature ranges from few months to 4 years. [3] Bilaterality, mostly asynchronous seminoma may be seen in 10% of cases. [1] Recently, a case of synchronous bilateral spermatocytic seminoma has been described for the first time in the literature in a 77-year-old man. Spermatocytic seminoma is an indolent neoplasm characterized by a long duration of symptoms, early stage at presentation, and absence of metastasis. However, in a small fraction of cases (approximately 6%), it may undergo sarcomatous transformation. [10] The sarcomatous component is usually rhabdomyosarcoma or undifferentiated, high-grade sarcoma. [5] In the present case, the patient had a neglected, slowly enlarging testicular swelling which gained a rapid and alarming increase in size over a 7-month duration. The seminomatous component was well circumscribed but the rhabdomyosarcomatous component was seen destroying the rete testis and the epididymis. It is important to recognize the epithelial structures of rete testis and epididymis so as not to mistake them for an epithelial component of a mixed nonseminomatous germ cell tumor. A minor sarcomatous component was undifferentiated and did not label with any myogenic antibody. The sarcomatous dedifferentiation in the spermatocytic seminoma is associated with aggressive behavior, presence of metastasis, and poor outcome. [4],[5],[9] The treatment of choice in spermatocytic seminoma is orchidectomy, followed by surveillance to detect a contralateral testicular tumor. However, in the presence of a sarcomatous component, adjuvant chemotherapy and radiotherapy may be beneficial. As risk of metastasis is increased with the presence of a sarcomatous component, close follow-up is essential. [9],[10] The prognosis for spermatocytic seminoma with sarcomatous transformation remains poor despite aggressive multimodality approach. In the present case, in view of the sarcomatous component a chemotherapy regimen was planned for the patient. However, he was noncompliant for further treatment, and no further outcome is available. In conclusion, the present case highlights that although indolent in its behavior, a spermatocytic seminoma can rarely undergo sarcomatous dedifferentiation, especially in long-standing cases. Orchidectomy is the treatment of choice for spermatocytic seminomas whereas in tumors with sarcomatous differentiation, in addition, chemotherapy and radiotherapy may be beneficial. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09053f4.jpg] [cr09053f3.jpg] [cr09053f2.jpg] [cr09053f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}