 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
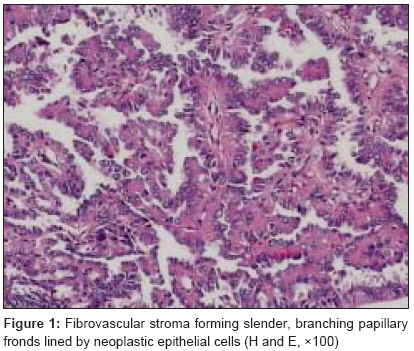
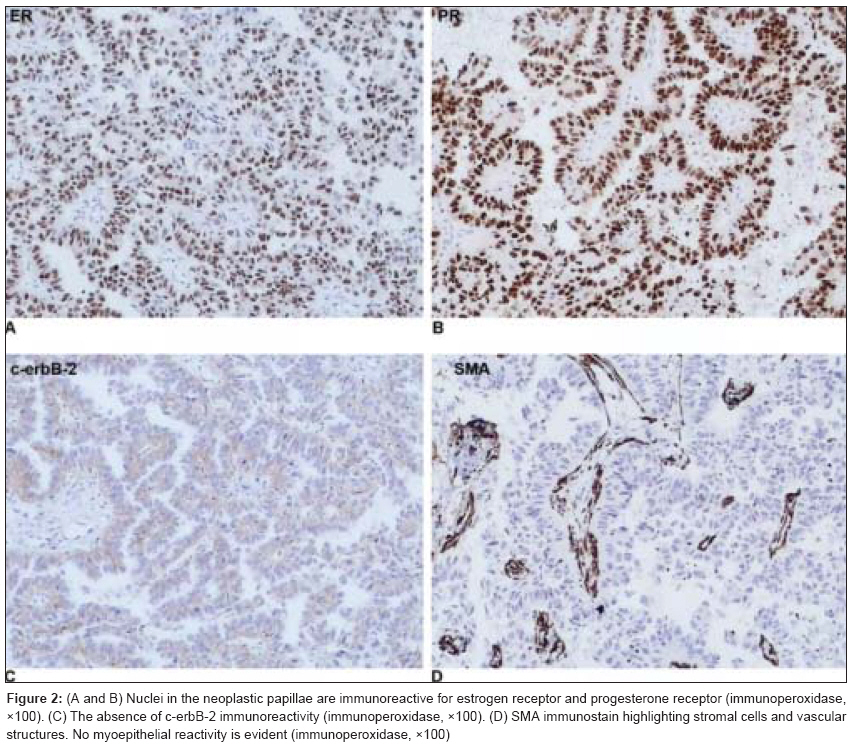
Journal of Cancer Research and Therapeutics, Vol. 5, No. 3, July-September, 2009, pp. 216-218 Case Report Invasive papillary carcinoma of the male breast: Report of a rare case and review of the literature Pant Ishita, Joshi SanjeevChandra Department of Pathology and Clinical Oncology, Advanced Medical and Dental Institute, Universiti Sains Malaysia, Pulau Pinang Code Number: cr09054 PMID: 19841568 DOI: 10.4103/0973-1482.57132 Abstract Breast masses occur in men far less commonly than women. Papillary lesions of the male breast are rare and comprise a spectrum of lesions ranging from benign intraductal papilloma to intraductal papillary carcinoma and invasive papillary carcinoma. In this case report, a 78-year-old man presented with a subareolar painless mass. Fine needle aspiration cytology (FNAC) was performed. Cytologic examination revealed a cellular aspirate. A diagnosis of papillary lesion favoring papillary carcinoma was rendered. The patient underwent modified radical mastectomy, which showed invasive papillary carcinoma. As far as we know, only a few cases of invasive papillary carcinoma of the male breast have been published in the literature. To the best of our knowledge, this is the first case report of invasive papillary carcinoma of male breast in Malaysia. In this purview, we discuss papillary carcinoma of male breast with review of the relevant literature.Keywords: Breast neoplasm, invasive papillary carcinoma, male Introduction Papillary carcinoma of the male breast is an extremely rare tumor (≤1%) [1] with an incidence definitely lower than that of its female counterpart. The clinical presentation of papillary carcinoma in males is generally a painless, firm, subareolar mass. Grossly and microscopically, it is similar to its female counterpart and can be in situ or invasive. As to prognostic features, there are different opinions concerning the biological behavior of male papillary breast carcinoma. Some authors have observed an aggressive biological behavior despite its bland microscopic features, while others report an excellent prognosis. As far as we are aware, only a few cases of invasive papillary carcinoma of the male breast have been published in the literature. Through a pubmed search, this is the first reported case of invasive papillary carcinoma of male breast in Malaysia. Case Report A 78-year-old male presented with a painless subareolar mass in the left breast, of 1 year duration. The mass had gradually increased in size. The patient had a positive family history of breast cancer. On clinical examination, a firm and well-circumscribed mass was palpable in the subareolar region of the left breast. A moderate degree of depression was noted in the nipple without ulceration or discharge. Mammogram showed a mass in the subareolar portion of the left breast. Fine needle aspiration cytology (FNAC) was performed. Aspiration yielded abundant hemorrhagic material. Cytological examination revealed a cellular aspirate, comprising of epithelial cells arranged in papillae, with few loosely cohesive sheets as well as intact single cells. The cells showed pleomorphic, hyperchromatic nuclei with scant-to-moderate amount of cytoplasm. The smear background varied from cystic to necrotic type. A cytological diagnosis of papillary lesion favoring papillary carcinoma was rendered. Surgical excision was recommended. The patient subsequently underwent modified radical mastectomy of the left breast with a complete dissection of the lymph nodes in the left axilla. On gross examination, the mastectomy specimen measured 13 x 13 x 5 cm. The nipple was partially retracted and the skin of the areola was wrinkled. Cut surface showed a well-circumscribed solid cystic granular mass measuring 5 x 4 x 4 cm with areas of hemorrhage, occupying almost the whole breast and surrounded by fibrous tissue. Representative samples were fixed in 10% neutral buffered formalin, dehydrated and embedded in paraffin. Sections were stained with hematoxylin and eosin. In addition, immunohistochemical studies were performed with peroxidase-antiperoxidase (PAP) technique using estrogen receptor (ER) protein, progesterone receptor (PR) protein, c-erb-B2 protein and smooth muscle actin (SMA) antibodies (all from DAKO Cytomation, Carpinteria, C, USA). Microscopically, the tumor showed an invasive papillary carcinoma, composed of numerous delicate, branching papillary fronds lined by epithelial cells [Figure - 1]. These cells exhibited moderate pleomorphism and hyperchromatic nuclei with a high nuclear cytoplasmic ratio. Mitotic figures were variably present. Myoepithelial cells were not seen [Figure - 2]D. The adjacent area showed inflamed fibrous granulation tissue infiltrated by hemosiderin-laden macrophages. The nipple was free from tumor infiltration. Tumor cells were immunopositive for ER and PR [Figure - 2]A, B but negative for c-erb-B2 and SMA [Figure - 2]C, D. Based on the above findings, a final diagnosis of moderately differentiated invasive papillary carcinoma was made. Discussion Breast carcinoma is rarely observed in males, the average incidence of which is 1% of all mammary carcinomas, and less than 1% of all carcinomas in men. [2] Unlike female breast cancer, in which incidence rates are rising throughout the world, for unknown reasons, the comparative incidence of male breast cancer has remained relatively stable in most countries. [3] The incidence of male breast cancer varies by geographical location. [4] It is more frequent in African Americans than in White Americans. The Japanese have a lower incidence rate compared to the Chinese, African, Egyptian, and Jewish population. These geographic variations may be due to definable factors, such as hyperestrogenism and chronic liver diseases secondary to cancers or parasites. The prevalence of male breast cancer increases with age. The etiology of male breast cancer remains poorly understood, but an imbalance in the estrogen-testosterone ratio is definitely implicated. Hormonal alterations due to testicular disease, Klinefelter′s syndrome, mumps orchitis, undescended testis, testicular injury, cirrhosis of the liver and exogenous estrogens are the proven risk factors. [5] Obesity as another risk factor may act by affecting estrogen levels by peripheral aromatization of androgens. Environmental factors include men employed in steel mills, blast furnaces and rolling mills, probably chronic heat exposure, which can suppress testicular function. [6] Other etiological factors include radiation exposure, drugs, head trauma (by increasing prolactin production), local chest trauma, and smoking. [7] A positive family history and mutation of BRCA2 gene show definite linkage to breast cancer. [8] The most common clinical finding in 75-90% of patients is a painless mass, which is centrally located 70-90% of the time. In collective reviews, the disease has a slight predilection for the left breast same as observed in this case report. The duration of symptoms before diagnosis is declining. Earlier series reported a mean of 14-21 months but recent series report a mean of 1-8 months. This may be due to increased public awareness of breast cancer in men. Virtually all known histological types of breast cancer have been identified in men. ER and PR immunopositivity is observed in 65-85% of cases as was noted in this case report. The high positivity of both the receptors in male breast cancer may be due to low levels of these hormones leaving the receptors available for binding, and is probably responsible for a good hormonal response. Other receptors like androgen receptors and glucocorticoid receptors have also been found to be positive in 50% of the cases though their clinical relevance is yet to be determined. [9] Epidermal growth factor receptor (EGFR) was rarely positive in one study, but was found in 76% of tumors analyzed in other study. [10] Its prognostic significance in men is yet unknown, whereas in women, it indicates poor prognosis. Regarding the prognosis, the stage and axillary node status are the most important prognostic indicators in male breast cancer. DNA ploidy, EGFR expression, HER-2 oncogene expression, and ER status have not been shown to be predictive of disease-free survival, although the S-phase fraction may have some significance, according to one study. The c-erb-B2 oncoprotein is a potentially useful prognostic marker in female breast cancer but scarce data is available on c-erb-B2 expression in men. In a recent study, the expression of the oncoprotein was lower (17%) in male patients than in female patients (33%), whereas in another study none of the male breast carcinomas studied expressed c-erb-B2. This case report also showed the absence of c-erbB-2 expression. Similarly, little is known regarding p53 gene alterations in male breast carcinomas, and so far no correlation between survival and p53 expression has been observed. To conclude, invasive papillary breast carcinoma of males remains an uncommon disease. Most of our current knowledge regarding its biology has been derived from its female counterpart. Much research is needed to characterize further the molecular and biological properties of male breast carcinomas and their prognostic significance so as to devise optimal treatment strategies. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09054f1.jpg] [cr09054f2.jpg] |
| |||||||||

{kind=link}
{kind=link}