 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
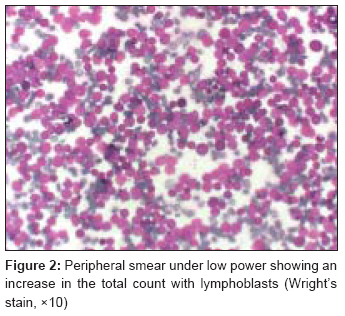
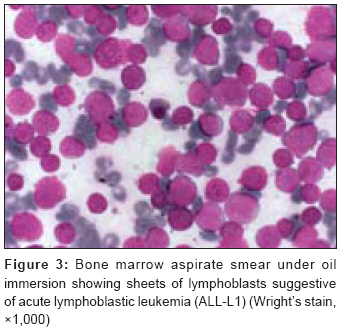
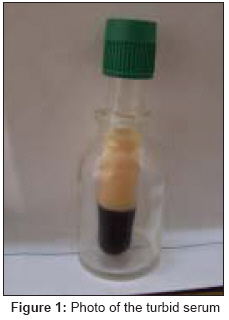
Journal of Cancer Research and Therapeutics, Vol. 5, No. 3, July-September, 2009, pp. 219-220 Letter to the Editor Turbid serum in a patient of acute lymphoblastic leukemia on treatment-What to look for? Singh Tejinder, Satheesh CT, Madhumathi DS, Goyal Mukul, Rajeev LK, Lakshmaiah KC, Suresh TM, Babu KGovind Department of Medical Oncology, Kidwai Memorial Institute of Oncology, Bangalore Code Number: cr09055 PMID: 19841569 DOI: 10.4103/0973-1482.57133 Sir, A 42-year-old male patient presented with a 1-month history of dyspnea and neck swelling. On examination, he was normotensive and had bilateral cervical lymphadenopathy with distension of neck veins suggestive of superior vena cava syndrome. An abdominal examination revealed hepatosplenomegaly. Computed tomography (CT) of the thorax and abdomen showed a large mediastinal tumor, thoracic and abdominal lymphadenopathy, and hepatosplenomegaly. Biopsy of the mediastinal tumor revealed a T-cell lymphoblastic lymphoma. The results of bone marrow aspiration were suggestive of acute lymphoblastic leukemia (ALL) [Figure - 2] and [Figure - 3], and a lumbar puncture was normal. His hemogram revealed Hb 12.4 gm/dL, WBC 8,000 u/L, and a platelet count 200,000 u/L. Serum biochemistry including random blood sugar and lipid profile was normal. The family history was negative for dyslipidemia or premature coronary heart disease. Remission induction therapy according to the GMALL protocol was initiated. [1] The patient was started on vincristine, daunomycin on days 1, 8, 15, and 22, and prednisolone on days 1-28. l-asparaginase was administered at a dose of 6,000 IU/m 2 for days 15-28 on every other day. The patient also received CNS prophylaxis with intrathecal methotrexate on day 1. He tolerated chemotherapy well, and laboratory parameters like hemogram and of biochemistry were determined during the remission induction therapy regularly. On day 28, prednisolone was tapered and on day 30, he started complaining of headache, bodyache, and fever. Random blood sugar was 120 mg/dL. In view of turbid blood, lipid profile was done. Serum triglyceride level was very high (>13,000 mg/dl). In addition, an increased level of cholesterol of 1200 mg/dL and elevated liver function parameters (bilirubin 1.4 mg/dL, alkaline phosphatase 670 mg/dL, aspartate aminotransferase 85 U/L, alanine aminotransferase 110 U/L, γ-glutamyltransferase 940 U/L, and lactate dehydrogenase 700 U/L) were detected. The serum values of pancreatic enzymes (amylase and lipase) were within the normal ranges. Fundi did not show lipemia retinalis. Ultrasound of the abdomen showed no fatty infiltration of liver. A lipolytic therapy with insulin (continuous infusion for 6 days) and atorvastatin 20 mg was initiated and resulted in a prompt and continuous decrease in the liver function test results and serum lipid levels. The patient was discharged from the hospital on day 52 and his serum cholesterol and triglycerides were normal. L-asparaginase has been associated with hypertriglyceridemia and hypercholesterolemia. Effect of L-asparaginase on hyperlipidemia is related to an increase in the endogenous synthesis of VLDL (very low density lipoprotein), a decrease in lipoprotein lipase activity and/or exogenous chylomicrons. [2],[3] L-asparaginase especially when used in combination with corticosteroids results in an increase in triglycerides in 10% of children. L-asparaginase associated with hypertriglyceridemia has been commonly reported in children, [4],[5] and few case reports are available concerning this toxicity in adults. In conclusion, our case report suggests that the turbid sample in adult ALL on L-asparaginase should make us check lipid levels. Routine laboratory monitoring should therefore include triglyceride and cholesterol levels in all patients (children and adults) receiving L-asparaginase.[Figure - 1] References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09055f2.jpg] [cr09055f1.jpg] [cr09055f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}