 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
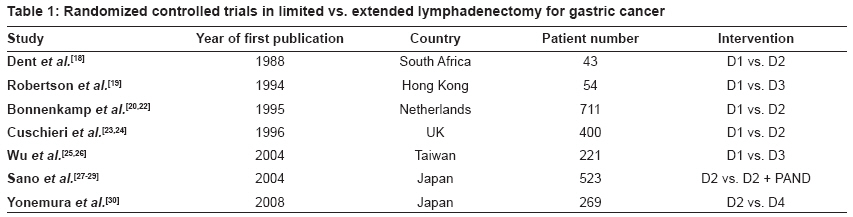
Journal of Cancer Research and Therapeutics, Vol. 5, No. 4, October-December, 2009, pp. 225-231 Review Article Surgery for gastric cancer: An evidence-based perspective D'souza MelroyA, Singh Kailash, Shrikhande ShaileshV Department of GI and HPB Surgical Oncology, Tata Memorial Hospital, Parel, Mumbai Code Number: cr09058 PMID: 20160354 DOI: 10.4103/0973-1482.59891 Abstract Despite a decreasing incidence, stomach cancer is the second leading cause of cancer mortality worldwide. Surgical resection offers the only chance for cure in this aggressive cancer. The surgical management of gastric cancer has witnessed numerous debates in the past decades. These include the extent of lymphadenectomy, extent of surgery, role of laparoscopic gastrectomy, and the impact of high volume of centers, on the outcome of surgery. This review attempts to address these controversies with an evidence-based perspective. A literature search in MEDLINE (www.pubmed.org) has been performed with the relevant key words and corresponding MeSH terms. The search has been limited to English publications on human subjects. A manual search of the bibliographies has also been carried out, to identify the relevant publications for possible inclusion.Keywords: Gastric cancer, gastrectomy, lymphadenectomy, subtotal gastrectomy, total gastrectomy, laparoscopic gastrectomy Background While the incidence of gastric cancer has declined worldwide including in India, it remains the second leading cause of cancer mortality globally. [1],[2],[3] In India, the stomach was estimated to be the fifth leading cancer site in males and seventh in females. [4] Gastric cancer is an aggressive disease. While localized disease has a better prognosis, the overall five-year survival rate for resectable gastric cancer is usually 20 - 30%. [5],[6],[7] The majority of patients who have undergone a curative resection develop recurrences in the stomach bed, the anastomosis, the regional lymph nodes or systemic metastases. [7],[8],[9] This has led to the establishment of many effective neo-adjuvant and adjuvant approaches in the multi-modality treatment of gastric cancer. [10],[11],[12] Even so, radical surgery is the cornerstone of treatment and offers the only chance for cure. A radical resection comprises of a gastrectomy and a lymph node dissection. What constitutes an ′adequate cancer surgery′ has been extensively debated in the past decades and management differs in different parts of the world. Numerous controversies still exist regarding various aspects of the surgical management of gastric cancer, such as, the extent of surgery, the extent of lymphadenectomy, the role of laparoscopic gastrectomy, and the impact of high volume centers. This review attempts to address these controversies with an evidence-based perspective. Methods A literature search in MEDLINE ( www.pubmed.org ) was performed with the key words Gastric cancer, gastrectomy, lymphadenectomy, subtotal gastrectomy, total gastrectomy, laparoscopic gastrectomy, and the corresponding MeSH terms. The search was limited to English language publications on human subjects and randomized controlled trials (RCTs). The key words, limits applied, and the numbers of publications retrieved for the issues being addressed are shown in [Figure - 1] (as of 29 August, 2009). Of the 101 publications retrieved, a total of 23 were found suitable for inclusion, while 78 were found not to be directly relevant to the issues at hand [Figure - 1]. A manual cross-reference search of the bibliographies of the retrieved publications and a further search for studies with regard to the impact of hospital volume was carried out, to identify the relevant studies for possible inclusion and yielded the further publications referenced in this review. Extent of Lymphadenectomy [Table 1]The lymph node status is a major prognostic indicator in gastric cancer. The extent of lymph node dissection during gastrectomy has been a matter of debate, ever since extended lymphadenectomy (D2) was introduced by Japanese surgeons in the 1960s. A D1 dissection involves removal of the perigastric nodes around the right and left of the cardia, the lesser and greater curvature, and the supra and infra-pyloric regions. A D2 dissection, in addition, involves removal of the nodes along the left gastric artery, common hepatic artery, celiac axis, splenic artery, and the splenic hilum. Thus a D2 dissection may often involve a splenectomy and distal pancreatectomy as well. Super-extended lymphadenectomy or D3 (also known as D2+ or D4) dissection involves in addition to the D2 resection, the removal of hepatoduodenal ligament nodes, posterior pancreatic nodes, mesenteric root nodes, mesocolic nodes, and para-aortic nodes. [13] The extent of lymphadenectomy in the treatment of gastric cancer is still a matter of debate globally. While Japanese surgeons routinely perform a D2 dissection, many western surgeons perform more limited (D1) lymph node dissection. The rationale for D2 resection is that the orderly centrifugal pattern of lymphatic tumor dissemination from the stomach allows for the prediction of the risk of metastasis to specific nodal groups. [14] Based on retrospective studies and reports from the Gastric Cancer Registry, radical gastrectomy with D2 lymphadenectomy is now the standard of care for resectable gastric cancer in Japan. [15],[16],[17] However, western investigators have not found a survival advantage with extensive lymphadenopathy when compared with a D1 dissection. The first randomized study to compare D1 and D2 gastrectomies was by Dent et al., [18] in which 43 patients were randomized to either D1 or D2 dissections. In this trial D2 lymphadenectomy was associated with greater blood transfusion requirement, increased morbidity, and a longer hospital stay, while there was no survival advantage. The authors concluded that this procedure should not be performed outside of controlled clinical trials. In a prospective randomized study by Robertson et al., [19] patients with adenocarcinoma of the gastric antrum were randomized to either D1 subtotal gastrectomy (n = 25) with omentectomy or D3 total gastrectomy (n = 30) with omentectomy, splenectomy, distal pancreatectomy, lymphatic clearance of the celiac axis, and skeletonization of vessels in the porta hepatis. Morbidity was significantly greater in the D3 group, as 14 patients developed subphrenic abscesses. The D3 group also had a significantly longer operating time, greater transfusion requirements, and a longer hospital stay as compared to the D1 group. Overall survival was significantly better in the D1 group (median survival of 1511 vs. 922 days, p < 0.05). The authors concluded that while D3 total gastrectomy could be performed with a low mortality, it had a high morbidity because of intra-abdominal sepsis and they therefore did not support the routine use of D3 total gastrectomy for the treatment of patients with antral cancer. The first large multicenter randomized study to compare D 1 and D 2 dissection was from the Netherlands by the Dutch Gastric Cancer Group (DGCG). [20],[21] This trial involved 80 hospitals, and randomized 1078 with gastric adenocarcinoma to undergo either D1 or D2 dissection. A total of 711 patients underwent a curative resection (380 in the D1group and 331 in the D2 group). Morbidity (25 vs. 43%) and mortality (4 vs. 10%) were higher for D 2 dissection. The postoperative hospital stay was also longer for the D2 group. Five-year survival rates were similar in the two groups: 45% for the D1 group and 47% for the D2 group. In the most recent update, after 11 years of follow-up, there was no overall difference in survival (30 vs. 35%; P = 0.53) between the two groups. [22] The authors identified splenectomy, pancreatectomy, and age older than 70 years as contributing risk factors for increased morbidity and mortality. Improved survival was seen in patients with N2 cancer, who underwent extended lymph node dissection, but unfortunately it remains difficult to identify patients with N2 disease . The overall results of this trial, therefore, did not support the routine use of D2 lymph node dissection in patients with gastric cancer. They thus concluded that extended lymph node dissections could be beneficial if morbidity and mortality could be avoided. A second large randomized multicenter trial was conducted by the British Medical Research Council (MRC), comparing D1 dissection with D2 dissection. [23] Of 737 registered patients with gastric adenocarcinoma, 400 were randomly assigned to treatment (200 to D1 dissection and 200 to D2 dissection). The results showed that the D2 group had greater postoperative hospital mortality (13 vs. 6.5%; p = 0.04) and higher overall postoperative morbidity (46 % vs. 28%; p < 0.001); and their postoperative stay was also longer. The excess postoperative morbidity and mortality in the D2 group was attributable to distal pancreaticosplenectomy and splenectomy. In the article reporting the long-term survival of patients in this trial, the five-year survival rates were 35% for D1 resection and 33% for D2 resection. [24] There was no difference in the overall five-year survival rates between the two arms. Multivariate analysis revealed that clinical stages II and III, old age, male gender, and removal of spleen and pancreas were independently associated with poor survival. The authors concluded that while D2 resection offered no survival advantage over D1 surgery, the possibility that D2 resection without pancreaticosplenectomy could be better than the standard D1 resection could not be dismissed by the results of the trial. The only randomized study demonstrating a survival benefit from extended lymphadenectomy (D3) was from a single institution study from Taiwan published by Wu et al. [25] Of a total of 221 eligible patients, 110 were randomly assigned to D1 surgery and 111 patients to D3 surgery. The morbidity rate was higher after D3 than after D1 resection (17.1 vs. 7.3%). This difference was largely due to abdominal abscess. Patients who had D3 resection had longer operating times, greater blood loss and transfusion requirements, greater postoperative drain outputs, and longer hospital stays. There was no death in either group. In their subsequent publication examining survival they found that the overall five-year survival was significantly higher in patients in the D3 group as compared to the D1 group (59.5 vs. 53.6%; p = 0.041). [26] They concluded that D3 nodal dissection as compared to D1, offers a survival benefit for patients with gastric cancer, when done by experienced surgeons. Even at five years the recurrence rates were 50.6% for D1 surgery and 40.3% for D3 surgery. However, this difference (p = 0.197) was not statistically significant. Thus this did not clearly explain the improvement in overall survival seen in patients who underwent D3 dissection. In a prospective randomized trial conducted in Japan in 24 hospitals, D2 lymphadenectomy alone (n = 263) was compared with D2 lymphadenectomy plus para-aortic nodal dissection (PAND) (n = 260), in patients undergoing gastrectomy for curable gastric cancer. [27-29] The surgical morbidity rate was 20.9% among patients assigned to D2 lymphadenectomy alone and 28.1% in those assigned to D2 lymphadenectomy plus PAND (P = 0.07). The five-year overall survival rate was 69.2% for the group assigned to D2 lymphadenectomy alone and 70.3% for the group assigned to D2 lymphadenectomy plus PAND; the hazard ratio for death was 1.03 (95% CI, 0.77 to 1.37; P = 0.85). There were no significant differences in recurrence-free survival between the two groups; the hazard ratio for recurrence was 1.08 (95% CI, 0.83 to 1.42; P = 0.56). This trial thus concluded that D2 lymphadenectomy plus PAND did not improve the survival in patients with curable gastric cancer. In another Japanese multi-institutional randomized trial of D2 (n = 135) versus D4 gastrectomy (n = 134) there was no significant difference in survival between the D2 and D4 groups (52.6% after D2 surgery and 55.0% after D4 gastrectomy; p = 0.801). Hospital death occurred in one patient in the D2 group and five in the D4 group. Seven patients (5.2%) in the D2 and 15 (11.2%) in the D4 group died of causes other than gastric cancer recurrence. The authors found that D4 gastrectomy was a more risky surgery than D2 dissection and concluded that prophylactic D4 dissection could not be recommended for patients with potentially curable advanced gastric cancer. [30] A meta-analysis published in 2005 analyzed two randomized and two non-randomized comparisons of limited (D1) versus extended (D2) node dissection and 11 reports of one dissection type. [31] For D2 dissection the randomized trials showed no overall survival benefit and an increased postoperative mortality. A trend toward survival benefit for D2 gastrectomy was observed for T3+ tumors. Non-randomized comparisons found no survival benefit from D2 gastrectomy, but decreased postoperative mortality. Nine observational studies on D2 lymphadenectomy reported better results than two studies on D1 surgery, but in very different settings. They concluded that the evidence for D2 dissection was inconclusive and that there was no overall survival advantage. They attributed operative mortality to pancreaticosplenectomy, low case volume, and lack of specialist training. In a recent meta-analysis published in 2009, 14 RCTs (3,432 patients) were reviewed. [32] Operative mortality and postoperative morbidity were higher in the D2 group than in the D1 group, and the three- and five-year survival rates were not statistically different. Also the operative times were shorter in D1 compared to D2. Operative mortality, morbidity, operative duration, and hospital stay were not significantly different between the D2 and D3 groups. Thus it was concluded that D2 and D3 dissection did not offer any specific advantages and instead could adversely affect patient outcomes. Maruyama has compiled a computer-based database with pathological data of 3040 patients. [33] With the knowledge of tumor size, position, and depth of invasion, the probability of lymph node metastases in the different lymph node stations can be calculated. Thus, with this program, the Maruyama Index (MI) can be calculated to identify the nodal stations at risk for metastases either pre- or intraoperatively. This information can be used to customize lymphadenectomy. This type of surgery is associated with increased survival. The applicability of the Maruyama program has been shown in a retrospective study by Peeters et al.[34] Data from the Dutch D1-D2 Lymphadenectomy Trial was analyzed in this study. The MI was calculated for 648 of the original 711 patients. Survival was assessed by log-rank and multivariate Cox regression analysis. The MI proved to be a strong predictor of survival by both univariate and multivariate analysis. The MI was an independent predictor for both overall survival and relapse risk. In 2009, the risks and possible benefits of extended lymphadenectomy for gastric cancer should both be still considered as unproven. Current evidence is compatible, with no benefit from D2 resection, but also with substantial benefit in a subgroup of patients. Opinion still remains divided between the Japanese and the western world; at our tertiary referral center, we routinely perform a modified D2 gastrectomy that is now standardized to avoid a pancreatectomy and splenectomy. [35],[36] Our series of 159 D2 gastrectomies documented very low morbidity and mortality. However, a further large randomized trial of D1 versus modified D2 surgery (distal pancreas and spleen preserving) needs to be carried out to settle the issue once and for all. Extent of Surgical Resection The extent of surgery, that is, total or subtotal gastrectomy depends on the size and extent of the tumor, its location within the stomach, and the ability to achieve tumor-free margins. A 5-cm distance from the tumor to the closest resection line in the intestinal-type and 10-cm margins in diffuse-type tumors is essential. [37],[38] For distal gastric cancers, subtotal gastrectomy has been shown to have an equivalent oncological outcome and lesser morbidity when compared to total gastrectomy. In the multicenter Italian trial conducted by the Italian Gastrointestinal Tumor Study Group, 618 patients with cancer of distal stomach were randomized during surgery to subtotal gastrectomy (n = 315) or total gastrectomy (n = 303). [39] The morbidity and mortality rates were 9 and 1% in the subtotal gastrectomy patients and 13 and 2% in the total gastrectomy patients, respectively. Thus, both procedures had similar complication rates and surgical outcomes. Multivariate analysis showed that splenectomy or resection of adjacent organs was associated with a two-fold risk of postoperative complications. In a subsequent publication, the five-year survival probability was 65.3% for subtotal gastrectomy and 62.4% for total gastrectomy. [40] Tumor site, tumor spread within the gastric wall, extent of resection, splenectomy, resection of neighbouring organs, and lymph node metastases, together had an impact on survival. The authors concluded that subtotal gastrectomy should be the procedure of choice, provided the proximal margin of resection was free of tumor. Subtotal gastrectomy was also associated with a better nutritional status and quality of life. For tumors confined to the proximal third of the stomach, total gastrectomy is the usual procedure of choice. It is debatable whether proximal gastrectomy is associated with poor functional outcome of the distal gastric remnant compared to total gastrectomy. Harrison et al., [41] in a retrospective review, demonstrated that patients with proximal gastric cancer who underwent total gastrectomy or proximal gastrectomy had similar overall survival times and recurrence rates and both procedures could be accomplished safely. In a retrospective analysis of 125 patients who underwent proximal gastric resection or total gastrectomy for cancer of the cardia, the five-year survival rate was 18 and 17%, respectively. [42] It was concluded that the extent of resection did not influence survival in adenocarcinoma of the gastroesophageal junction. Role of Laparoscopic Gastrectomy The first laparoscopic gastrectomy with a Billroth II construction for cancer was performed by Kitano and published in 1994. [43] Since then, several authors have reported successful laparoscopic subtotal or total gastrectomy, demonstrating the important postoperative advantages of this procedure. [44],[45],[46],[47] However, the role of laparoscopic surgery in the treatment of gastric cancer has not yet been defined, and doubts remain about its ability to satisfy all the oncological criteria that are met with during conventional, open surgery. In prospective randomized studies of open versus laparoscopy-assisted distal gastrectomy (LADG) for early gastric cancer, interim results showed that LADG had several advantages over open surgery. [48],[49],[50] These included early recoveries, less postoperative pain and better postoperative pulmonary functions, while yet maintaining the radicality of surgery. In a prospective randomized trial by Huscher et al., [51] 29 of 59 patients were randomized to undergo open subtotal gastrectomy, while 30 patients were randomized to the laparoscopic group. The lymph node yield and morbidity and mortality rates were comparable, with no significant differences between the two groups. The five-year overall and disease-free survival rates were 55.7 and 54.8% and 58.9 and 57.3% in the open and the laparoscopic groups, respectively, showing no significant difference. The authors thus concluded that both laparoscopic radical subtotal gastrectomy and the open approach were comparable in terms of feasibility, safety, and oncological radicality, with similar short- and long-term results. In addition, the laparoscopic procedure was associated with reduced blood loss, shorter time to resumption of oral intake, and earlier discharge. In Japan, early-stage gastric cancer (T1/T2, N0) is considered the only indication for laparoscopic gastrectomy. [52] There is evidence in the literature that the procedure is technically safe, recovery is faster, hospital stay is shorter, and there is less pain as compared to the open procedure. However, data on the oncological outcome of the laparoscopic gastrectomy is limited and high-level evidence is lacking. Good quality multicenter RCTs, comparing the outcomes after laparoscopic surgery versus open surgery are necessary in order to establish the role of laparoscopy in gastric cancer surgery. Laparoscopic gastrectomy has a steep learning curve, and credentialing for such procedures remains an unresolved issue. [53] With this background, new data, even from RCTs, will have to be interpreted with caution before laparoscopic gastrectomy can be firmly established as a procedure of choice. In a recently published retrospective study the technical feasibility, effectiveness, and safety of robot-assisted gastrectomy with lymphadenectomy was evaluated in a series of 100 consecutive patients. [54] The clinicopathological characteristics and surgical outcomes in this series were comparable to the open and laparoscopic gastrectomies, demonstrating the effectiveness and safety of this novel approach. Impact of Hospital Volume on Surgical Outcome Expertise improves the outcome for patients with curatively resected gastrointestinal cancer. Hospital procedure volume, as a proxy, has been shown to predict clinical outcome for complex surgical procedures. [55],[56] Few studies have examined the relationship between hospital procedure volume and survival after a curative resection of gastric cancer. [57-62] These reports have been based on cancer registry databases or administrative claims-based sources. In a Swedish population-based study by Hansson et al., the two-month postoperative mortality was superior for patients with gastric cancer operated at ′university′ (high-volume) centers as compared to ′local′ (low-volume) hospitals. [58] Studies have also shown a relationship between hospital volume and long-term survival. [59],[60] The study by Nomura et al. [59] examined the influence of hospital volume on long-term survival after curative resection of gastric cancer, as reported in the Osaka Cancer Registry. They noted that during the period of 1975 to 1979, overall survival was better in the high volume centers. This advantage, however, decreased with time and eventually disappeared between 1990 and 1994, except for the very-low-volume hospitals. The authors suggested that this diminishing difference between high- and low-volume hospitals, over time, could be the result of surgical standardization and the improvement of surgical techniques in the smaller institutions. In a study by Enzinger et al., [62] it was found that hospital surgical volume was not predictive of overall survival or disease-free survival. However, patients who underwent either a D1 or D2 dissection at a high- or moderate-volume center experienced a trend for improved outcome as compared with those patients resected at a low-volume hospital; these results were not statistically significant. The authors concluded that excluding the impact of perioperative mortality, hospital procedure volume had no overall effect on long-term gastric cancer survival. However, studies were required for the confirmation of the potential benefits of moderate- to high-volume centers for patients who underwent a D1 or D2 dissection. In a recent review it was found that the best treatment results were seen in high volume hospitals with experienced surgeons, even taking into account the extended surgical procedures. [63] Summary The management of gastric cancer has changed over the past decade mainly because of the evolution of new evidence. Evidence for the extent of lymphadenectomy in light of the publications analyzed is still divided and evolving. However, further trials comparing limited and extended resections are required, to answer this issue. On the basis of the present evidence, D2 gastrectomy, without pancreatectomy and splenectomy, can be considered as the procedure of choice, provided it can be performed with low morbidity and mortality. Regarding the extent of surgery, subtotal gastrectomy is better than total gastrectomy in distal gastric cancer, provided the proximal margin of the resection falls within the healthy tissue; however, the extent of surgery does not seem to influence survival in cancer of the gastroesophageal junction. Laparoscopic radical subtotal gastrectomy is a feasible and safe oncological procedure and has the additional benefit of less blood loss, shorter time to resumption of oral intake, and shorter hospital stay, but randomized controlled studies are needed. In gastric cancer patients, hospital procedure volume has a complex effect on the outcomes after surgery; however, the best treatment results are seen in high volume hospitals with experienced surgeons. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09058f1.jpg] [cr09058t1.jpg] |
| |||||||||


![[Figure - 1]](/showimage?cr/photo/cr09058f1.jpg){kind=link}
{kind=link}