 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
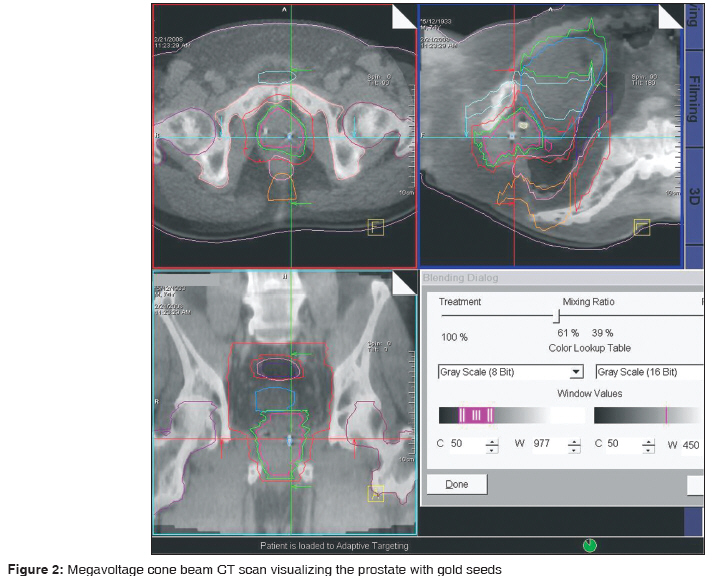
Journal of Cancer Research and Therapeutics, Vol. 5, No. 4, October-December, 2009, pp. 277-283 Original Article Dose escalation in image-guided, intensity-modulated radiotherapy of carcinoma prostate: Initial experience in India Swamy Kumara, Sathiya Narayanan VK, Basu Sumeet, Maiya Vikram, Achari Rimpa, Deshpande Shrikant, Bhangle Janhavi, Gupta KamleshKumar, Babu Nirmal, Pawar Surendra, Atre Ashish, Balachandra Kashyapi, Koppiker CB Department of Radiation Oncology, Ruby Hall Cancer Center, Ruby Hall Clinic, 40, Sassoon Road, Pune-411 001, Maharashtra Code Number: cr09066 PMID: 20160362 DOI: 10.4103/0973-1482.59909 Abstract Background : Increasing incidence and significant stage migration from distant metastases to a localized disease, due to screening application of PSA, is taking place in carcinoma prostate. Also, role of radiotherapy is increasing in carcinoma prostate due to rapid strides in technology.Aim : The present retrospective study, evaluates escalating the dose in the treatment of localized carcinoma prostate using integration of multiple advanced techniques. Settings and Design : The settings designed are: a) use of gold seed internal fiducial markers: b) clinical application of emerging Megavoltage Cone Beam Computed Tomography (MVCBCT) technology for Image Guided Radiotherapy (IGRT); c) Intensity Modulated Radiotherapy (IMRT); d) adopting biochemical method for follow-up. Methods and Material : Twelve consecutive, biopsy proven localized cancer of prostate patients, treated with dose escalation IMRT& IGRT protocol between August 2006 and January 2008, were analyzed. Gold seed markers in prostate were used for daily localization with MVCBCT or Electronic Portal Imaging (EPI). All patients underwent clinical and biochemical follow-up. Statistical Analysis& Results : Planned dose of 7740 cGy was delivered in 10 out of 12 patients (83%). While one patient had migration of maximum of 3 mm, two others had 1 mm migration of one seed during course of treatment. One patient (8%) developed Grade II proctitis at 12th month. During the mean follow-up duration of 12.2 months, 92% (11/12) had biochemical control within 3 months of treatment. Conclusions : IGRT technique using MVCBCT for implanted fiducial gold seed localization was feasible for IMRT dose escalation in carcinoma prostate with excellent results. Keywords: Dose escalation, gold seed markers, image guided intensity modulated radiotherapy, PSA. Introduction It is clear that a dose of radiation (>70 Gy) higher than conventionally used has been delivered to give long term bio-chemical relapse free survival in prostate adenocarcinoma. Kannan et al. have shown that a dose of 72 Gy by 3DCRT can be safely delivered to the prostate with excellent gastrointestinal tolerance. [1] Kupelian PA et al. demonstrate that dose escalation has led to improvement in the local, biochemical and distant control in a cohort of patients followed over a period of 14 years. [2] Once the radiation dose is escalated, there is a dire need to reduce dose to the normal tissues. Conformal radiotherapy has established its role in randomized trials with reduction in severity of side effects. [3] Zelefsky et al. demonstrated that IMRT, even with dose levels of 81 Gy, significantly reduced the risk of gastrointestinal (GI) toxicities compared to the patients treated with 3D-CRT (from13 to 5%). [4] Since dose escalation and consequent effect on the quality of life is related to the volume of normal tissue irradiated, reducing this volume becomes essential and this is now possible with image guidance. [5] MVCBCT, an IGRT system uses a digital linear accelerator treatment unit equipped with a flat panel detector to obtain a three-dimensional representation of the patient in treatment position. The use of MVCBCT for IGRT was proposed in 2003 and was clinically applied in 2005. In view of imperfect definition of the prostate for cone beam CT, surrogate internal gold seed markers are used as localizers. The present study is an evaluation of high dose IGRT-IMRT in localized adenocarcinoma of the prostate. Material and Methods Twelve consecutive patients with biopsy proven localized cancer of prostate, who were treated with Intensity Modulated Image Guided dose escalation radiotherapy protocol, from August 2006 to January 2008, were taken up for analysis. Although 13 patients fulfilled the criteria for recruitment for the study, one patient who did not follow the protocol of therapy in terms of schedule (and who in between opted for concurrent alternative therapy) was excluded from the study. All the patients underwent complete metastatic work-up, which included serum PSA levels, chest radiograph, bone scan, abdominal and pelvic Computed Tomography (CT) scan. In view of the intermediate and high-risk disease, three of the patients were started on concurrent goserelin, two patients were started on concurrent leuprolide depot, and two patients underwent orchidectomy. Patients fulfilling the protocol conditions were planned for insertion of fiducial gold markers after taking informed consent. All the patients were started on Tab. Norfloxacin and Tinizadole, a day, prior to the procedure and the same medications were continued for four days. On the day of the procedure, they were also started on Inj. Amikacin 500 mg half an hour before the procedure and subsequently 500 mg twice a day for three more days. Three fiducial gold markers preloaded in an 18 gauge needle, supplied by Medtech® , each of 1.2 mm diameter and 3 mm in length [Figure - 1], were inserted into the prostate under ultrasound guidance, transrectally, by an urologist. Care was taken that all the markers were placed within the prostate in 3 non-coplanar positions as far away from each other as possible. Markers were inserted one in each on the right and left lobes and one, slightly off midline (to avoid the urethra) at the apex of the prostate. Patients were asked to report if they developed any symptoms after the insertion. Since image guidance was used to localize the prostate before switching on the beam, no specific instruction was given regarding diet and voiding. In radiation therapy of pelvic malignancies, we found it effective to combine vacuum fixation device with individualized knee-rest to minimize both longitudinal with the former and rotational errors with the latter. Hence both these immobilization devices were used in the present cohort of patients. A planning CT scan of the area of interest was taken with 3 mm slice thickness. All patients underwent MRI scans of the pelvic region, as well, but for one patient who had undergone Coronary Artery Bypass Graft (CABG) surgery earlier. The three laser centers for localization were tattooed as reference points. The CT and the MRI images were fused on the Coherence Dosimetrist® of Siemens and contouring was done on the same. The structures contoured included the prostate (GTV), CTV (GTV + seminal vesicles), CTV-Nodal (CTV + pelvic nodes), urinary bladder, rectum (up to the sigmoid colon), heads of femuri and small bowel. To take care of intrafractional errors PTV margin of 8 mm was given in all directions, except posteriorly where 5 mm margin was given. PTV margin chosen is based on the systematic and random errors in our setting. IMRT treatment planning was done on KonRad® Inverse planning system. Usual number of beams used was seven and segments varied from 100 to 150. The prescription isodose had to cover 95% of the target PTV. Recommendations for normal tissue dose constraints were followed. Specifically, two criteria were adopted to reduce possibility of rectal complications: a) 90% of prescription isodose to be within the half width margin of rectum and b) 50% to fall within the full width of rectum on all axial slices. [6] As per the protocol, the dose prescribed was 4500 cGy in 25 fractions to the PTV-CTV-Nodal. This was followed by 1440 cGy in 8 fractions to PTV-CTV. The final phase included the GTV with a 3 mm expansion to dose of 1800 cGy in 10 fractions. The total dose was 7740 cGy in 43 fractions over 8 ½ weeks. The patients were taken up for treatment using a linear accelerator, Oncor Impression Plus with amorphous silicon flat panel (used for Mvision® platform) from Siemens by MLC based step and shoot IMRT method. On the first day of treatment delivery, patients in the treatment position were aligned with the tattoo marks. The patients were then moved to the isocenter manually. All data about patient position were noted, including the couch vertical position (for subsequent sessions couch vertical position was used instead of source axis distance (SAD), for positioning the patient. We found this as a very practical method to reduce the vertical positional set up errors). Before the delivery of treatment, Mvision® was used for acquiring Mega Voltage Cone beam CT (MVCBCT) scans with gantry rotation from 270 to 110 degrees using 6 MU dose protocol. Cone beam MU dose protocol that we used was after evaluating minimum imaging dose that could give reasonable gold seed visualization at our center. We also reduced the imaging volume in the cranio-caudal direction to further reduce the dose delivered with MVCBCT. This field width reduction for MVCBCT was possible since visualization and co-registration with bony pelvis was not required. The total time for image acquisition and simultaneous reconstruction was less than 3 minutes [Figure - 2]. Image co-registration process, involving planning CT done on the planning day and MVCBCT image of the treatment day, was done automatically by adoptive software, which can be verified manually. This automatic registration, primarily based on bony anatomy, uses maximization of mutual information (MMI algorithm), makes the subsequent manual (external reviewer inferred) co-registration adjustment minimal. The procedure is an anatomy based physical co registration of the CT slices of the data set in each of the optional three planes, namely axial, coronal and saggital. The process of assessing external reviewer inferred registration using gold seed fiducial marker was then done. On visualization of the gold seed markers on the MVCBCT images, these markers were aligned with the planning CT image having complete tumor and normal tissue contoured structures [Figure - 3]. After the clinician was satisfied with the alignment, offset (shift) calculations were acquired in longitudinal, vertical and horizontal directions in mm. The necessary correction was then applied online if offset data exceeded 3 mm level. In our clinic protocol, cutoff level of 3 mm was adopted taking into account MVCBCT inherent resolution error and flat panel deployment error. The final table positions, including the couch vertical position and patient position vis-à-vis immobilization devices, were recorded and frozen for further daily treatments. On the second day, localization was done using antero-posterior and lateral portal imaging. We found it difficult to visualize and identify the location of seeds in digitally reconstructed images (DRRs) as well as EPI (despite the availability of high resolution flat panels), especially in lateral projections. So, we evolved a technique to overcome this problem with the following steps.
The acute and late effects of RT were in accordance to National Cancer Institute′s Common Terminology Criteria version 3.0 for adverse events. The patients were followed up every three months after completion of RT both clinically and biochemically. Assessment of local failure was dependent on physical examination or imaging studies. Results [Table - 1] shows the patient and treatment characteristics, including T, N status, PSA levels (baseline) Gleason score and MSKCC risk cohort, [7] in the present cohort of patients. Pre radiotherapy Androgen Deprivation Therapy (ADT) was done in 8 /12 patients and subsequently continued. Two patients were started on ADT along with radiotherapy. Two of the 12 patients evaluated were low risk and did not receive ADT. Application of criteria of 90% of prescription isodose to be within the half width margin of rectum and 50% isodose to fall within the full width of rectum on all axial slices of CT scan (except in few slices where there was sudden change in the curvature of rectal contor) was successful in all patients. Escalated dose of 7740 cGy/ 43 f′s/ 5 f per week over 8 ½ weeks was delivered in 10/12 patients (83%). One patient had co-morbid drug induced nephropathy with raised creatinine levels and had persistent urinary incontinence during the entire course of radiation. In his case radiation dose was restricted to 7020 cGy in 39 fractions. Subsequently, during the follow-up, his nephropathy got stabilized and urinary symptoms disappeared and PSA turned to normal range. One patient missed out the last fraction. One patient out of 12 had pain lasting for three days after insertion of gold seed marker. None of the others had any symptoms. In two patients, 1 mm migration of one seed was seen; in one patient, 3 mm migration was present on day 14 and in the same patient 1 mm migration of another seed was present at the end of the treatment. In such exceptional cases (since all the three seeds cannot be matched accurately) the remaining seeds were used for aligning. MVCBCT, along with EPI was used successfully in all patients in daily prostate localization with internal gold seed fiducials as surrogate markers [Figure - 2] and [Figure - 3]. The total dose delivered with MVCBCT was 140 - 150 cGy and that with EPI was 30 - 40 cGy, totaling to about 180 cGy. This added up to about one additional fraction, over 8 ½ weeks. Altogether, 217 MVCBCT procedures were done in 12 patients (average of 18 per patient). The shifts recorded in 3 directions of MVCBCT image guidance are given in [Table - 2]. On the average 30% of the time, there was a need to correct the position of the patient. Also, in 13% of the time (28 readings out of 217 procedures) the longitudinal shift was more than recommended PTV value of 8 mm and/or vertical (anteroposterior) shift of > 5mm. The median duration of follow-up was 12.2 months, maximum was 17 months and minimum was three months and all had clinical and biochemical follow-up. All the 12 patients had pre-radiotherapy urinary symptoms; of which four patients continued to have symptoms at 3 rd month and none had any symptoms at the sixth month. At the 12 th month, one of the 12 patients (8%) developed proctitis and none had > grade 2 proctitis or cystitis. PSA level < 2 ng/ml at third month in 11 patients, giving a biological response rate of 92 % (11/12) at third month. In one patient biochemical response at sixth month was awaited. During this relatively short period of follow-up no patient had local progression of disease or distant metastases. Discussion This article gives the clinical results of application of several modern technological concepts in routine clinical application in the radiotherapy management of carcinoma prostate. For PSA-era patients treated between 1987 and 1995, median radiotherapy doses increased from 64 Gy (range, 60 to 68 Gy, during 1987-89) to 70 Gy (range, 66 to 78 Gy, during 1994-95). [8] As early as 1998 Zelefsky et al. showed better outcome in carcinoma prostate with 3D Conformal Radiation Therapy. They showed in a Phase I study that a significant difference in positive biopsy at > or = 2.5 years after 3D-CRT, which was in 7% of patients receiving 81.0 Gy, compared to 48% after 75.6 Gy, 45% after 70.2 Gy, and 57% after 64.8 Gy. Therefore, they proposed dose escalation as a definition of new standard for curative radiotherapy in this disease. Later Hanks et al, performed a matched pair analysis of 714 patients, one half of whom were treated to < 74 Gy versus those who were treated with >= 74 Gy. Freedom from biochemical failure, freedom from distant metastases, and survival were all significantly higher for the patients treated to the >= 74-Gy dose level. [9] This was followed by the publication of randomized trial by Pollack A et al. which highlighted that 8-Gy dose escalation benefited most of the patients with a pretreatment PSA of more than 10 ng/mL; five-year freedom from biochemical and/or disease failure rates were 48% and 75% for the 70-Gy and 78-Gy arms, respectively. [10] Presently, three other randomized trials have shown improved PSA relapse free survival for escalation doses of radiotherapy, [11],[12],[13] in addition to several institutional series. Also, studies have shown that with the adoption of new technology, even with the dose escalation there is no deterioration of quality of life (QOL). [14] Based on the outcome of these results, dose escalation has become an established standard of practice. Consequently, in the present group a dose of 7740 cGy/ in 43 fractions, 180 cGy per fraction was prescribed to all patients. A 10-year toxicity profile is now available (with cohort of patients followed up to 15 years), after the adoption of high dose conformal techniques - initially 3DCRT and subsequently IMRT and is acceptable. In the present series, 1/12 patients (8%) developed Grade II proctitis and none had > grade II proctitis or cystitis. The follow-up is too short a period to evaluate GU toxicities. Day-to-day position of prostate (interfraction errors) varies from 3 to 5 mm. [15] To account for this error, treatment margin of 10-15 mm must be defined, which increases the possibility of normal tissue reactions. GSF is visible on planning CT and MRI, MVCBCT and MVCB portal imaging. This consistently helps in daily localization of prostate and thus permits reduction in the treatment margin. There is negligible migration of markers during the course of RT, [16] and marker migration or prostate deformation is far below the present tumor delineation accuracy. [17] Another important advantage of GSF use is that it reduces the inter-user variability of the image registration. The marker-based registrations showed the least amount of inter-user variability while the contour-based ones showed the most. [18] The role of these markers in accurate verification of position and correction is now well established. [19] Langenhuijsen et al. in a series of patients with ultrasound guided transrectal marker implantation reported minor complications of pain and fever (6.2%), voiding complaints (1.9%), transient hemeturia lasting more than three days (3.8%), hematospermia (18.5%) and rectal bleeding in (9.1%). They concluded that the procedure is safe and well tolerated. They have suggested that inserting three markers instead of 4 may be the reason for lesser rate of side effects reported in other series. [20] We found three markers procedure safe and well tolerated with none of our patients reporting any adverse effect. All our patients received prophylactic antibiotic therapy and received analgesics if necessary. In the present study we have used image guidance (IG) using implanted gold seed fiducial (IGSF). The use of implanted markers located with a variety of imaging methods is accepted as a localization technique. However, significant disagreement exists about the adequacy, accuracy, and method to follow for individual imaging techniques. The contentious points are; a) frequency of imaging, b) accuracy of localization vs. the cost associated with imaging, c) excessive use of machine time, d) patient imaging dose. It is also suggested that localization should be performed daily. [21] For the purpose of daily imaging and to simultaneously balance the associated issues, we have effectively alternated MVCBCT (6 MU dose per session) with portal (2 MU dose per session). Although IG with IGSF, by daily verification eliminates the effect of voiding, full bladder/ loaded rectum etc, evaluation of intrafraction movement of the prostate is a limitation in the present study. A 3-mm margin for intrafractional errors could be adequate for prostate dose coverage. However, it is documented that a subset of patients lost seminal vesicle dose coverage significantly due to rectal volume changes. Also, analysis suggests that the impact of bladder positional variations was secondary to the rectal positional variations. Therefore, in the treatment of advanced-stage prostate cancers, larger than 3 mm margins is to be given or one has to improve organ immobilization (e.g. with a rectal balloon) to ensure adequate seminal vesicle coverage. [22] According to Kotte A et al. intrafraction motion of the prostate occurs frequently during external-beam irradiation on a time scale of five to seven minutes and minimum margins of 2 mm can account for these intrafraction motions. However, they conclude that larger margins are required in practice to accommodate other uncertainties in the treatment. [23] In our series we used 8 mm margin (5 mm posteriorly) during initial phases of the treatment and 3 mm margin during the GTV boost phase. Data on the use of linear accelerator based MVCBCT technology in localization of prostate cancer is emerging presently and not as widespread as Kilovoltage (KV) and Kilovoltage Cone Beam Computerized Tomography (KVCBCT) imaging. The literature about KVCBCT for day-to-day image guided localization and alignment in the treatment delivery of prostate tumors is extensive. It is obvious that the dose delivered during cone beam imaging using kV is definitely lower. [24] In our clinic, we have seen both software and hardware based improvement in the image quality over the last two years. We have found MVCBCT as a useful and well-integrated system in the workflow, especially in the management of carcinoma prostate. One aspect of this technique has been the dose of MVCBCT contribution to the total dose. We have limited this contribution of additional dose by using a lower MU dose of 6 MU, reducing the width of exposure and alternating MVCBCT with EPI and single exposure (since no matching was done with bony pelvis) for both antero-posterior and lateral EPIs′. The visualization of gold seeds has been adequate with our technique. The amount of seed migration and prostate deformation was not significant. Learning curve has been smooth, greatest impact being at the level of technologists, with significant improvement in positioning of patients. We have evolved our IGRT protocol at our clinic regarding the daily MU of MVCBCT. In addition, a protocol was designed to reduce the contribution of total dose of Image guidance by alternating MVCBCT (6 MU) with EPI (2 MU). Further, we evolved a DRR technique of seed localization for EPI, as enumerated in the material and methods. Our results also show that in about 30% of the number of fractions there was a need to correct the position of the patient. Also, in 13% of the number of fractions, when IMRT is delivered without IGRT (with the generally recommended PTV margins), some portions of the tumor could be under dosed or normal tissue could get included in the high dose area. This occurs primarily due to interfractional movement of the prostate in longitudinal and /or antero-posterior directions. Our initial results in terms of local and biochemical control are comparable with that of literature. The toxicities were acceptable in this dose escalation study. Small number of patients and shorter duration of follow-up are the limitations of this study. This limitation has precluded us from analyzing the effect of ADT on outcome. The other limitation is inability to evaluate intrafraction motion of the prostate. We conclude that IGRT technique using MVCBCT for implanted fiducial gold seed localization was feasible for IMRT dose escalation in carcinoma prostate with excellent results. For about 30% of the number of fractions there was a need to correct the position of the patient. Also, when IMRT is delivered without IGRT (with the generally recommended PTV margins) in 13% of the number of fractions some portion of the tumor could be under dosed or normal tissue may get included in the high dose area. The learning curve has been smooth, the greatest impact being at the level of technologists, with significant improvement in positioning of patients. Hypo-fractionation schedules and sub-volume boost would be the future prospects at our center. References
Copyright 2009 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr09066f3.jpg] [cr09066t1.jpg] [cr09066t2.jpg] [cr09066f2.jpg] [cr09066f1.jpg] |
| |||||||||

![[Figure - 1]](/showimage?cr/photo/cr09066f1.jpg){kind=link}
{kind=link}
![[Figure - 3]](/showimage?cr/photo/cr09066f3.jpg){kind=link}
![[Table - 1]](/showimage?cr/photo/cr09066t1.jpg){kind=link}
![[Table - 2]](/showimage?cr/photo/cr09066t2.jpg){kind=link}