 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
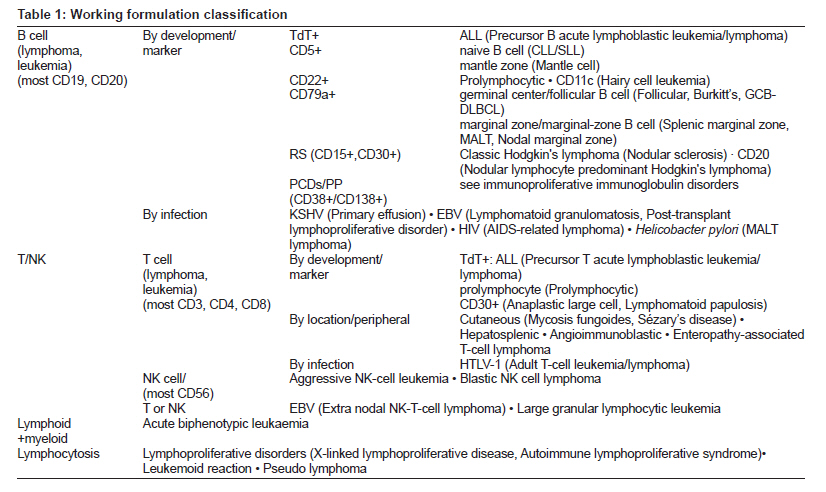
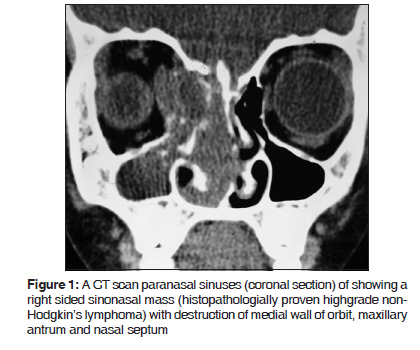
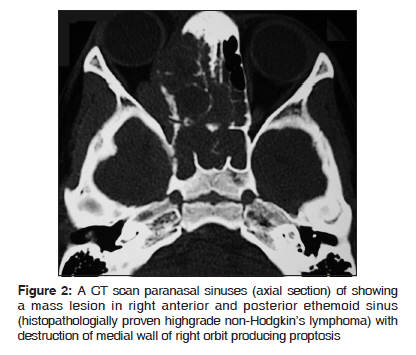
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 5-10 Review Article Non-Hodgkin's lymphoma of the sino-nasal tract in children Olaf Zagólski, Raghav C. Dwivedi 1 , Somasundaram Subramanian2 , Rehan Kazi 1 Department of Head & Neck, Medical Centre “Medicina”, Kraków, Poland, Code Number: cr10003 DOI: 10.4103/0973-1482.63553 Abstract Childhood head and neck cancers are relatively uncommon. Of all head and neck cancers occurring in children, non-Hodgkin's lymphoma (NHL) is the most common, others being rhabdomyosarcoma and nasopharyngeal carcinoma. In the head and neck region, sinuses are the second commonest primary site of NHL after neck lymph nodes. These can be of several different types depending on the predominant cell type and histologic appearance, the most common histological variant being diffuse large B-cell lymphoma. In an attempt to simplify the classification and to develop a universally acceptable classification and staging, they have been classified and staged numerous times over the last three decades, adding more confusion to the topic. Clinical presentations vary according to the histological type. The low grade lymphomas present with a nasal cavity or para-nasal sinus mass associated with obstructive symptoms and/or lymphadenopathy, while high grade lymphomas present with aggressive signs and symptoms including non-healing ulcer, epistaxis, septal perforation and bony destruction. The primary treatment consists of chemotherapy and / or radiation therapy, which is able to achieve remission in two-third of the patients, however, prognosis remains poor with cumulative five-year survival rates at about 30% for all the types of sino-nasal NHLs. Newer targeted therapy (monoclonal antibodies) and combination therapies (including stem cells) are currently being tested in order to improve survival rates in these patients. This article aims at providing an overview of clinico-epidemiologic characteristics, staging system currently in use, management, prognosis and possibilities of future research in the field of childhood sinonasal NHLs.Keywords: Children, non-Hodgkin's lymphoma, sino-nasal tract Introduction Neoplasms of the head and neck region are uncommon in childhood. [1] Lymphoma is the most common of all pediatric head and neck tumors; others being rhabdomyosarcoma, nasopharyngeal carcinomas, thyroid carcinoma and eosinophilic granulomas. [2] It is also the commonest cause of primary malignant disease of the head and neck region in the pediatric population. [2] Lymphomas can conventionally be of either Hodgkin's type or Non-Hodgkin's type. Hodgkin's lymphoma has a characteristic bimodal age incidence; the first one is seen around adolescence (pediatric age group), while the second peak is seen in the middle ages. On the other hand, non-Hodgkin's lymphoma (NHL) occurs more frequently (than Hodgkin's type) in the head and neck region in the pediatric age group. Though any anatomical sub-site may be involved by the pediatric NHL, most commonly it is encountered in neck lymph nodes, then within the nose and para-nasal sinuses. [1],[3],[4],[5] These are classified into several subtypes based on the predominant cell type of the tumor [Table - 1]. Clinical presentation, treatment options and the outcomes vary according to the histological type of the tumor, making the understanding of the topic even more confusing. This article aims to highlight some of the important commonly agreed aspects in the epidemiology, symptomatology, staging and management of this relatively rare disease. Clinico-Epidemiologic Characteristics NHLs of the sino-nasal tract can be morphologically difficult to distinguish from destructive non-neoplastic disease in the head and neck region in children and adults. [6] The disease is commonly known to involve nasal cavity, one or more para-nasal sinuses, or multiple regions within the sino-nasal tract [6] constituting 25% of all pediatric head and neck NHL. Since these are not part of the head and neck lymphatic system, it earns them a name of extra-nodal head and neck NHL. [3],[7] Other commonly involved sites are nasopharynx (16%), tonsil (12%), and the base of tongue (8%). The last three sub-sites collectively represent extension of the nodal lymphatic system within the head and neck region, the Waldeyer's Ring, giving them the name of nodal head-neck NHL, which in this way makes them the most common locations of NHL within the head and neck region (36%). [3] Sinuses are primary site of NHL in 90% of cases, most commonly invaded by diffuse large B-cell lymphoma (DLBCL) [8],[9] while primary nasal tumors occur in just 10% of cases. [8] Primary lesions located in the orbit, hard palate or in multiple sites are rare. [9] Within nasal cavity, NK/T-cell lymphoma is the most commonly encountered variant. [8] NK/T lymphoma occurs predominantly in younger population, with a lower male-to-female ratio, [8] however, the overall disease shows a male preponderance. [6],[8] Clinical presentations vary according to the histological type. The low grade lymphomas present with a nasal cavity or para-nasal sinus mass associated with obstructive symptoms and/or lymphadenopathy. [8] Shortness of breath, wheezing, high-pitched breathing sounds are among the common presentations but they are not suggestive of NHL themselves. [10] The high grade lymphomas (38% of NHL in the sinonasal tract) are more likely to present with aggressive signs and symptoms including non-healing ulcer, cranial nerve manifestations, facial swelling, epistaxis, or pain. [8],[9] High grade B-cell lymphomas tend to present with soft tissue or boney destruction [Figure - 1] particularly of the orbit with associated proptosis [Figure - 2] whereas the T-cell lymphomas are associated with nasal septal perforation and/or destruction. [8] Extra nasal dissemination occurs rarely to lymph nodes, skin, and testes. [9] At presentation, approximately 50% of patients have associated nodal disease, and only 20% report systemic or B symptoms. [8] There is a high incidence (15%) of extra nodal relapse outside of the gastrointestinal tract in patients with oral-sinonasal lymphoma to larynx, skin, liver, uvula, kidney, breast, lacrimal gland, testis, and prostate gland. [1],[6],[11] At initial presentation, three-fourth of the patients have Stage I or II disease and approximately two-thirds of those have intermediate-grade lymphoma. [3],[8] Histologically, mixed-cell lymphomas (MCLs) and large cell lymphomas (LCLs) prevail over lymphoblastic lymphoma (LBL) and small cleaved-cell lymphoma (SCCL); the frequencies of occurrence of T-cell and B-cell lymphomas being almost similar. [6],[9] High predominance of B-cell lymphomas in the sino-nasal region in oriental populations was reported with the T:B ratio greater than that observed for primary lymph node-based neoplasms. [9] Staging Systems There is a wide spectrum of morphologic types of lymphoma; [6] as a result several different staging systems were proposed and tested from time to time. Over the last three decades, a variety of systems including the Rappaport, Luke-Collins, and Working Formulation classifications have been used to classify extra nodal NHLs of the head and neck. [3] The Working Formulation is a classification of non-Hodgkin lymphoma that was published in early 1980s [Table - 1]. [12] In this system, miscellaneous tumors include composite, mycosis fungoides, histiocytic, extramedullary plasmacytoma, and unclassifiable lesions. [12] Working Formulation has been recognized as imperfect for primary extra nodal lymphoma, especially for patients with sino-nasal disease because of their histological characteristics. [13] Ann Arbor staging system, which was initially developed for Hodgkin's lymphoma is by far the commonest staging system to be used for the adulthood NHL as well and is still used by many despite its limited utility in NHL. [14] It has roughly the same function as TNM staging in solid tumors. [15] The stage depends on location of malignancy (confirmed on physical examination, CT scanning, positron emission tomography or MRI) and on systemic symptoms due to the lymphoma ("B symptoms": night sweats, weight loss of > 10% or fevers). [15] Principal stages are determined by location of the tumor:
The older classifications have been replaced by other lymphoma staging systems; the most recent was published by the World Health Organization (WHO) in 2001, which is still used by cancer agencies for compilation of lymphoma statistics. [16] According to the classification, there are four major types of childhood non-Hodgkin lymphoma:
Evaluation and Management Childhood sino-nasal NHL should be suspected in any case presenting with breathing problems with/ without painless swelling of the lymph nodes within the head and neck region. [10] In some cases the diagnosis is further suggested by the presence of axillary / inguinal lymphadenopathy, abdominal mass, dysphagia, fever of unknown reason, unexplained weight loss, bone pains and night sweats. [17] The pretreatment clinical investigations include physical examination, serum biochemical assessments, determination of lactate dehydrogenase (LDH) levels, computed tomography [Figure - 1] and [Figure - 2] and/or magnetic resonance imaging (MRI) of the head and neck, computed tomography (CT) of the thorax, abdomen, and pelvis, and examination of the bone marrow aspiration smears. In cases where erosion of the cribriform plate is suspected an MRI should ideally be performed to rule out any dural involvement. The gold-standard diagnostic method is the histopathological examination of the tissue; therefore a tissue biopsy is a must to be performed. [18] In case of nodal enlargement, excisional biopsy should be preferred over the incisional biopsy or a core biopsy. [18] But if the mass is limited to the nasal cavity or the peripheral nervous system (PNS), a generous tissue biopsy should be undertaken to establish correct histological type of the tumor. Bone marrow biopsy may be necessary in some cases to rule out any marrow involvement by the disease. [19] Chest X-ray, CT or MRI scans of the thorax and the abdominal cavity should be routinely performed for correct staging of the disease. [10],[20],[21],[22] In general, in pediatric patients, Murphy's classification is used, [23] which takes into account the natural history of the disease and has greater prognostic value. Murphy's Classification Stage I : A single tumor or nodal area outside of the abdomen or mediastinum. Stage II : A single tumor with regional node involvement or two or more tumors or nodal areas on one side of diaphragm or a primary gastrointestinal tract tumor (resected) with or without regional node involvement. Stage III : Tumors or lymph nodes on both sides of diaphragm or any primary intrathoracic or extensive intra abdominal disease or any paraspinal or epidural tumors. Stage IV : Patients with bone marrow or central nervous system (CNS) disease, regardless of other sites of involvement. Treatment for childhood sino-nasal NHL primarily includes chemotherapy and / or radiation therapy. [13] Role of surgery is limited to establishing the diagnosis only. [3] The type of chemotherapy and the route of administration of the chemotheraptic agents depend on the type and stage of the disease. [13] Most frequently administered drugs include doxorubicin, vincristine, prednisone, 6-mercaptopurin, and methotrexate. [24] Intrathecal chemotherapy is used if the disease has spread or may spread to the brain. [7] Radiation therapy is the primary treatment modality for localized disease in children and adolescents (Stages I and II), especially for low-grade lymphomas. [3],[24] It is generally not preferred if the tumor is lying close to the optic nerve because of the fear of damaging it and producing a blind eye; also, radiation-induced second cancers limit its use in treating sino-nasal NHLs. [13] Combination chemotherapy with or without radiation is used for more advanced disease and for intermediate- and high-grade lymphomas. [3],[24] Newer treatment modalities are currently being tested in clinical trials. Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells. [25] Monoclonal antibody therapy is the most widely tested form of the targeted therapy for NHL which has shown some promising results. [25] Monoclonal antibody therapy uses antibodies made in the laboratory from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances that may help cancer cells to grow. [25] The antibodies then attach to these identified substances and block their growth, keep a check on their spread and finally killing them. It is a systemic therapy and is given by the infusion. They can be used alone or to carry drugs, toxins, or radioactive material directly to kill the cancer cells. [25] Standard treatment for disseminated B-cell (Burkitt and Burkitt-like) non-Hodgkin lymphoma in children and adolescents is usually combination chemotherapy with CNS prophylaxis (intrathecal chemotherapy). [26] Monoclonal antibody therapy combined with chemotherapy is being tested in clinical trials for disseminated B-cell non-Hodgkin lymphoma in children and adolescents. [25] Standard treatment of disseminated lymphoblastic lymphoma in this age group, which was considered incurable until the 1970s, is usually combination chemotherapy with or without radiation therapy to the brain. [27] Standard treatment of disseminated anaplastic large-cell lymphoma in children and adolescents is combination chemotherapy with or without CNS prophylaxis (intrathecal chemotherapy). [7],[28] The treatment of recurrent childhood non-Hodgkin lymphoma in children and adolescents may include high-dose chemotherapy with stem cell transplant [29] or combination chemotherapy or combination chemotherapy and monoclonal antibody therapy. [13] Standard treatment of lymphoproliferative disease in children and adolescents with diminished immune response may include, surgery with or without radiation therapy or combination chemotherapy. [30] Some ongoing clinical trials are trying to test the efficacy of combination of multiple therapies like monoclonal antibodies combined with chemotherapy and stem cell transplant followed by donor lymphocyte infusion or an infusion of T-cell lymphocytes that have been treated in the laboratory, the results of which are awaited. [30] Sino-nasal infections with microorganisms are typical of immunosuppresed patients as they occur very frequently. [31] These can also be a result of complication of the therapy which is often difficult to manage and may require specific treatment for longer periods. Prognosis The prognosis depends on the type and stage of disease, the number of sites of extra nodal spread, invasion of the CNS and the patient's general condition. [3] Patients with lymphomas of high histopathologic grade and recurrent or disseminated disease have the worst prognosis. [3] Two-third of the patients remain in the remission phase after initial therapy. [3] In one-third of the patients diseases relapse and three-fourth of these patients die of the disease. [3] The cumulative five-year survival rates are about 30% for all the types, 55% for diffuse large B-cell lymphoma, 33% for peripheral T-cell lymphoma, and 20% for angiocentric lymphoma. [13] Five-year overall and event-free survival rates after treatment are 52% and 50%, respectively. [7] Ten-year survival is relatively better for the patients with Waldeyer's ring non-Hodgkin's lymphoma than for individuals with oral-sinonasal non-Hodgkin's lymphoma. [11] In contrast to results of Asian studies in which nasal NK/T-cell lymphoma has a very poor prognosis, American studies report that nasal NK/T-cell lymphomas have an outcome similar to that of DLBCL. [8] Conventional combined treatment (CHOP chemotherapy + radiotherapy) is ineffective for the NHL of the sino-nasal tract (especially NHLs of the nasal cavity), NHLs with tumor cells positive for T-cell markers, NHLs with stage higher than Stage IIE and NHLs with B symptoms. [13],[32] Possibilities of Future Research Several types of mutation are known to occur in NHLs. In sino-nasal NK/T-cell lymphoma (NKTCL), frequency of mutations in p53, K-ras, c-kit, beta-catenin, and bak gene is found to be 62.9%, 0%, 11.1%, 18.5%, and 25.9% respectively, while in cases of B-cell NHLs these figures are 71.4%, 0%, 23.1%, 21.4%, and 57.1%, respectively, showing that mutation frequency in all genes was higher in B-cell than in NKTCL cases. [33] These findings suggest that gene mutations might be the driving-force for B-cell lymphoma, whereas combined Epstein-Barr virus (EBV) infection and gene mutations contribute to NKTCL development. [33] c-kit gene encodes for a receptor tyrosine kinase, which plays a crucial role in proliferation and differentiation of hematopoietic stem cells. [34] Mutations of p53, a well-known tumor suppressor gene, as well as exon 4, K-ras, c-kit and beta-catenin mutations, were observed in sino-nasal NHL to show significant differences between different countries. [34] Mutations causing constitutive activation of KIT have been shown to be a causative factor in sinonasal lymphomas. [35] These activating mutations can be divided into two types - 'regulatory type' mutations, which affect regulation of the kinase molecule, and 'enzymatic pocket type' mutations, which alter the amino acid sequence directly forming the enzymatic site. [35] KIT inhibitors have been suggested to be an important therapeutic strategy for these conditions, but different types of activating mutations respond differentially to KIT inhibitors, so classification of individuals on the basis of specific mutations is necessary to guide therapy. [35] The findings that gene mutations might be the driving force behind lymphomas can promote further research aiming at possible treatment methods in the future. Specific gene inhibitors might be promising as therapeutic agents. Also, the roles of coexisting infectious factors (EBV and others) which play potentially causative roles in lymphomas need to be further investigated. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10003f1.jpg] [cr10003f2.jpg] [cr10003t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}