 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
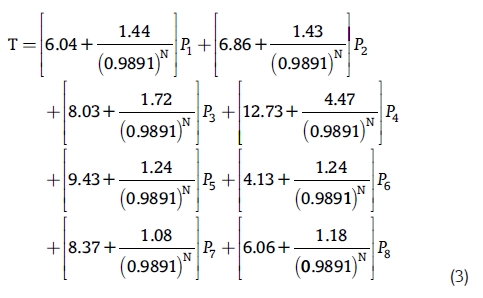
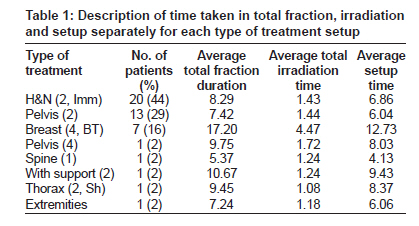
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 27-30 Original Article Workload modeling for teletherapy unit Abhijit Mandal, Anupam Kumar Asthana, Rashmi Singh, Lalit Mohan Aggarwal Department of Radiotherapy and Radiation Medicine, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221 005, U.P, India Code Number: cr10007 DOI: 10.4103/0973-1482.63568 Abstract Aims : This study aims to derive a radiotherapy workload model using a prospectively collected dataset of patient and treatment information from a teletherapy treatment unit. Materials and Methods : Information about all individual radiotherapy treatment was collected for two weeks from the Phoenix unit in our department. This information included diagnosis, treatment site, treatment time, fields per fraction, technique, use of blocks and wedges. Data were collected for two weeks (10 working days) in January 2008. During this time, 45 patients were treated with 450 fractions of external beam radiotherapy in Phoenix unit. Results : The mean fraction duration, irradiation time and setup time were 9.55 minutes, 1.84 minutes and 7.66 minutes respectively. A mathematical workload model was derived using the average fraction duration time, total irradiation time and setup time of different types of treatment. A simple software program (Workload Calculation Chart) was also constructed in Microsoft Excel using the derived algorithm. The model based software program was tested and applied for one year and found that it can be used effectively to describe workload of teletherapy unit. Conclusion : Proposed methodology for workload modeling of teletherapy unit and the workload calculation software is very effective to quantitatively plan/calculate the optimal workload which will satisfy both the patient care administrator and radiation therapy technologists.Keywords: Mathematical model, radiotherapy, workload Introduction The patient care quality and quantity should be balanced in radiation oncology department. Any treatment facility should provide well-justified and optimal patient care services. Radiation therapy technologists always struggle with complicated, time taking treatment setup and huge patient load. [1] Poor staff coherence/moral, critical error in treatment delivery, inefficient/expensive treatment may result from any type of disturbance in the balance. So there is a need to maintain balance in the department. By commenting on the number of patient being treated in a particular treatment unit cannot satisfactorily state the workload. The patient care administrator or the technologists should have some mathematical tool to quantitatively calculate/plan the workload of any treatment unit. Some researchers have formulated the workload model as per their work practice. [2],[3] But these models are complicated and cannot be applied in our work practice setup. Taking consideration in all the above factors we have made an attempt to develop a mathematical workload model for the teletherapy treatment unit by conducting a simple prospective study, collecting the patient and treatment related information in our center. Materials and Methods The center We treat about 1500 cases per year using two telecobalt units (Theratron-780E and Phoenix). All the major sites are treated. Head and neck cancers, carcinoma cervix and breast are the most common three sites treated in our center, which consists of about 70% of cases. Usually head and neck cancers are treated by two parallel opposed lateral fields with immobilization, carcinoma cervix by two parallel opposed anterior/posterior fields or by four fields, box technique and breast cancers by five fields (four fields daily and one field weekly). Wedges, shields breast cone are also used as per requirement. The radiation therapy technologists work in pair in each treatment unit. Data collection Data were collected for every fraction delivered by a telecobalt unit (Phoenix), during the first two-week period in January 2008. Patients who were treated for first/last fractions during this study period and altered fractionation were excluded from this study. Data collected for each fraction included diagnosis, treatment site, number of fields, use of immobilization device/wedges/shielding blocks, total fraction duration and total irradiation time. All data collected and entered on a daily basis during the study. Fraction duration was defined as the time when the patient entered the room until the time the patient left the room. The radiation therapy technologist used a stopwatch to calculate the total time taken in every treatment fraction. Results We collected data for two weeks (10 working days) in January 2008 in Phoenix unit. During this study period, 45 patients were eligible for the study. These 45 patients were treated with 450 fractions of external beam radiotherapy. The mean fraction duration, irradiation time and setup time were 9.55 minutes, 1.84 minutes and 7.66 minutes respectively. The median fraction duration, irradiation time and setup time were 8.08 minutes (range: 5.37 minutes-19.91 minutes), 1.42 minutes (range: 1.08-5.49 minutes) and 6.72 minutes (range: 4.13-14.43 minutes) respectively. Out of 45 patients, 20 (44%), 8 (17%), 7 (16%) and 10 (23%) patients are head and neck, carcinoma cervix, breast and others respectively. Radiation treatment was delivered to 20 (44%), 13 (29%), 7 (16%), 1 (2%), 1 (2%), 1 (2%), 1 (2%) and 1 (2%) patients with head and neck (two lateral fields with immobilizations), pelvis (two AP/PA fields), breast (four fields), pelvis (four fields), spine (single fields), thorax (two fields with shields), with stretcher (two fields) and extremities (two fields). [Table - 1] describes the average fraction duration time, total irradiation time and setup time for each type of treatment setup. Workload modeling From [Table - 1] it can be observed that for any type of treatment the fraction duration is the sum of total irradiation time and treatment setup time. So we can write: Fraction duration = Irradiation time + Treatment setup time ...(1) We consider the treatment in telecobalt unit, the eqn 1 can be written as: Fraction duration = Irradiation time + Treatment setup time/[0.9891] N (2) Where 0.9891 = Decay factor of co-60 Radioisotope in one month and N = Number of month between the time when model used for plan/calculate workload and the time when the workload model derived. On the other hand, the operational time of the unit is the time between start of first fraction of the day to the end of last fraction of the day. In our center, the working time is eight hours, which includes 30-minute lunch break. So the actual operational time (T) can be written as: T = 8 hours - 30 minutes = 450 minutes This actual operational time should be distributed properly among the fractions. So that
Where P1 - Number of Patients with two pelvic fields (AP/PA) P2 - Number of Patients with two lat fields (Rt/Lt) and immobilizations P3 - Number of Patients with four pelvic fields box technique P4 - Number of Breast treatment with four fields and breast cone P5 - Number of Patients with two pelvic fields (AP/PA) with streture P6 - Number of Spinal treatment with single field P7 - Number of Thorax region treatment with two fields and shields P8 - Number of Extremities region treatment with two fields
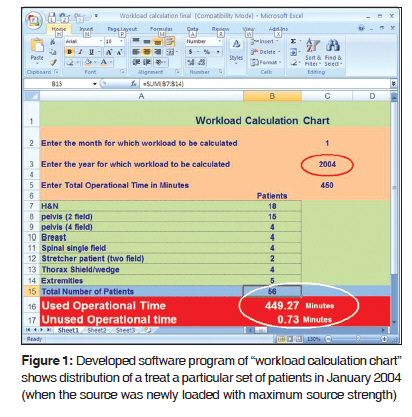
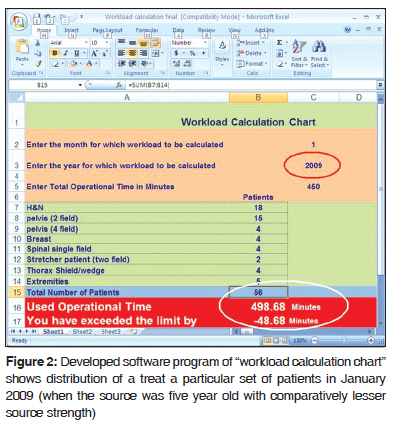
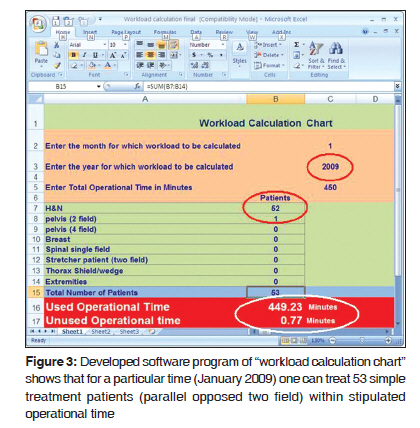
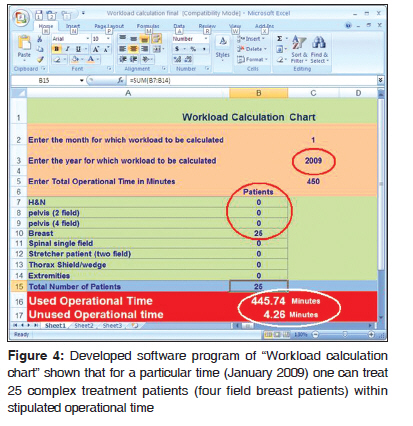
Where S i, I i and P i are the average patient set up time, average patient irradiation time and number of patient of i th type of treatment (e.g. head and neck, breast, pelvis etc.). By using the above algorithm we have constructed a simple "Workload Calculation Chart" software in Microsoft Excel, which can instantly determine the "Used Operational Time" and provide the message of "Unused operational time" or "You have exceeded the limit by" by entering the total operational time, number of patient of different type, month and year of application. Discussion We have derived a mathematical model and a software program to plan/calculate the efficient and optimal workload for our telecobalt treatment unit using a prospective dataset of patient and treatment related information. From the developed software program of "Workload Calculation Chart," it is observed that one can treat a particular set of patients in January 2004 (when the source was newly loaded with maximum source strength) easily [Figure - 1] and on the other hand in January 2009 (when the source was five year old with comparatively lesser source strength) to treat the same set of patient we got the message "You have exceeded the limit by 48.68 Minutes" [Figure - 2]. From this observation one may consider that in telecobalt therapy the patient load should decrease accordingly from time to time. [Figure - 3] and [Figure - 4] describe that for a particular time (January 2009) one can treat 53 simple treatment patients (parallel opposed two field) or 25 complex treatment patients (four field breast patients) within stipulated operational time. These observations state that the number of patients should not be taken as the only parameter to describe the workload in the telecobalt unit. There are several workload models, which have been proposed to standardize the workload of radiation facility. The Inter-Society Council for Radiation Oncology derived the equivalent simple treatment visit (ESTV) model, where Treatments are divided into simple, intermediate and complex categories. A simple treatment is equivalent to 1 ESTV unit that is about 15 minutes. [2] The more complex treatment needs more ESTV units. Another proposed model is basic treatment equivalent (BTE). [3] In this model, a BTE equation was derived for each patient. This equation estimates the time required to deliver a fraction of treatment. BTE model considers all the factors such as first fraction/subsequent fractions, photon beam/mixed photon/electron beam, junction, number of fields, number of Shields/wedges/port films and performance status. It is assumed that 1 BTE is approximately equal to a basic treatment of 10 min. performance of different radiotherapy workload models also compared by Barbera et al. [4] One can also categorize simple treatment required less fraction duration (with single and two fields in single spinal, extremities and pelvis treatment), intermediate treatment required moderate fraction duration (two field treatments with immobilization/support/shield/wedge like head and neck) and complex treatment required more fraction duration (with large no of fields and use of complex accessory). In our center, we regularly struggle with the huge workload and we do not want the actual operational time to be misused by any means. We have tested and applied the proposed model based software "Workload Calculation Chart" to plan/calculate the workload of the treatment unit during the year 2008. It was observed that this model is capable of defining the workload quantitatively, which satisfactorily balances the quantity and quality of patient care. Conclusion It may be proposed that by using the above methodology one can develop a workload model based simple software program for teletherapy treatment unit and quantitatively plan/calculate the optimal workload which will satisfy both the patient care administrator and radiation therapy technologists. Acknowledgment Authors are thankful to Mr. Santosh Kumar Sharma, Mr. Vikas Kumar Mishra, Ms Kanak Upadhya and Ms Priya Singh for their contribution in data collection. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10007f1.jpg] [cr10007f3.jpg] [cr10007f4.jpg] [cr10007f2.jpg] [cr10007t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}