 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
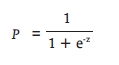
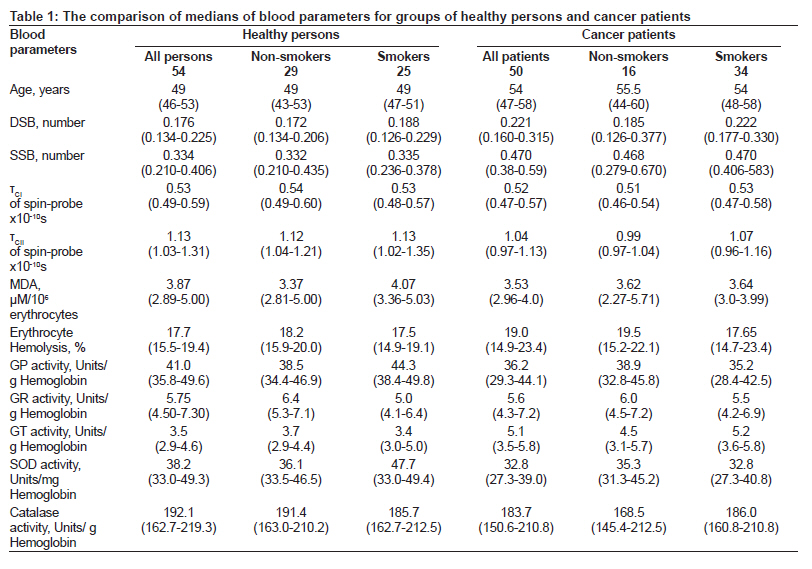
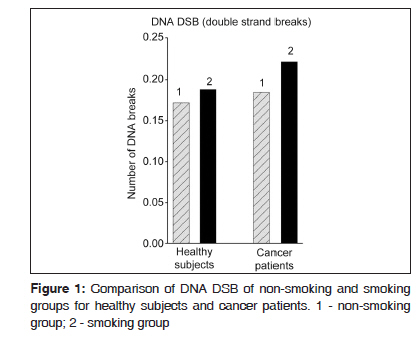
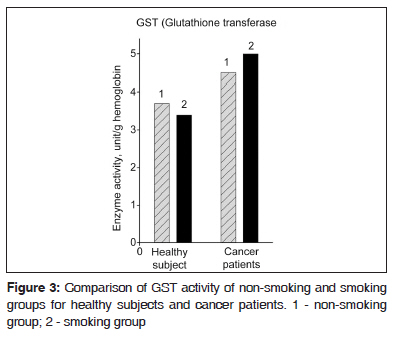
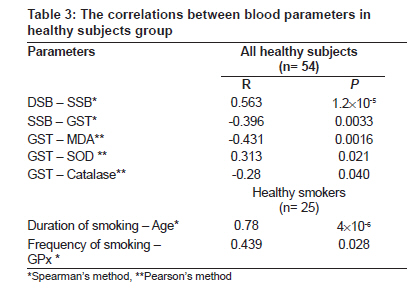
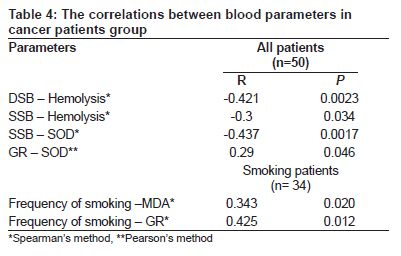
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 47-53 Original Article Biomarkers of oxidative stress and smoking in cancer patients Elena B. Burlakova, Galina P. Zhizhina, Svetlana M. Gurevich, Lyudmila D. Fatkullina, Antonina I. Kozachenko, Lena G. Nagler, Tatiana M. Zavarykina, Viktor V. Kashcheev Emanuel Institute of Biochemical Physics, Russian Academy of Sciences, Moscow, Russian Federation Code Number: cr10011 DOI: 10.4103/0973-1482.63569 Abstract Context: Increased oxidative stress is a significant part of pathogenesis of smoking-related cancer. Aim: The study aims to investigate changes in antioxidant status induced by chronic cigarette smoking in cancer patients and healthy subjects. Setting and Design: We examined the venous blood samples of 54 healthy subjects, both smokers (25) and non-smokers and of 50 patients with smoking-related cancer, both smokers (34) and non-smokers. Materials and Methods: We measured the activities of five antioxidant (AO) enzymes: glutathione peroxidase, glutathione transferase (GST), glutathione reductase, superoxide dismutase and catalase in the blood of 50 cancer patients and 54 healthy persons. Damage to cellular structures (level of malonic dialdehyde, micro viscosity of erythrocyte membranes, number of leukocyte DNA breaks) was determined. Statistical analysis of results obtained was performed using conventional and multi-factorial statistical methods. Results: Statistically significant increase in GST activity and DNA breaks, but decrease of membranes micro viscosity in cancer patients, compared with healthy subjects were obtained. In the cancer patients, no influence of smoking on studied parameters was found. Correlations of parameters within cancer patients and healthy subjects group did not coincide with each other. Conclusions: Changes of AO status parameters and oxidative damages in cell structures are related to tumor processes indicating the augmentation of oxidative stress in human blood. This study demonstrated potential applicability of a statistical model based on the evaluated biomarkers of oxidative stress to determine a smoking-induced harm of cancer incidence in healthy subjects.Keywords: Biomarkers, cancer, oxidative stress, smoking Introduction Smoking is one of the major lifestyle factors influencing the health of human beings. It is known that cigarette smoke and tar phase contain a number of oxidizing compounds, reactive oxygen species (ROS) and carcinogens, which damage the genome, membranes and macromolecules of cells. [1],[2],[3],[4] It is assumed that the quinone-hydroquinone radical complex from the cigarette tar causes redox-cycling that generates superoxide radicals from molecular oxygen and leads to formation of hydrogen peroxide and hydroxyl radicals. [5] Smoking may enhance oxidative stress not only through the production of reactive oxygen radicals in cigarette tar and smoke but also through weakening of the antioxidant defense systems. Caused by smoking prooxidant / antioxidant imbalance elevates oxidative stress which is accompanied by increase of lipid peroxidation, oxidative Deoxyribonucleic acid (DNA) damage and disturbances of enzymatic antioxidant defense. There is evidence that oxidative stress is an important event in the development of smoking-related diseases such as lung and oral cancer and chronic obstructive pulmonary disease. [3] Moreover, approximately 60 known carcinogens and mutagens are present in tobacco smoke. The action of oxidative agents and mutagens is accompanied by DNA damage, mutations in cancer-related genes, oncogenes activation, tumor suppressors' inactivation and deregulation of gene expression. Some of these events can induce the development of malignant process. [6] The present study aims to investigate potential changes in the antioxidant status induced by chronic cigarette smoking in cancer patients compared to healthy subjects, utility of some oxidative stress parameters for estimating smoking-induced harm and a probability of cancer incidence in healthy subjects. The evaluation of these parameters was performed in cancer patients with tumors of upper airways, oral cavity and lung. Materials and Methods Fasting venous blood samples were collected from two groups of males including 54 healthy subjects (mean age 48 ± 1.5 years) and 50 untreated cancer patients (54 ± 2.5 years). Cancer of upper airways (larynx, laryngopharynx, oropharynx, and nasopharynx) was primary diagnosed in 32 patients, cancer of oral tissues - in seven patients, cancer of lung - in 11 patients. Each of the main groups included two sub-groups such as smokers and nonsmokers. The group of healthy subjects consisted of 25 smokers and 29 non-smokers. The group of cancer patients included 34 smokers and 16 non-smokers. The mean ages of investigated human groups were sufficiently close. The healthy smokers and non-smokers were of mean age 48 ± 1.5 years; the sub-group of smoking cancer patients was 54 ± 2.5 years and group of non-smoking patients was 52.4 ± 1.1 years of age. In the group of healthy smokers, mean duration of smoking was equal to 32 ± 1 years and frequency was 18 ± 1 cigarettes daily (28.8 ± 1 pack years). Furthermore, the sub-group of high intensity smoking (11 subjects, 20-30 cigarettes daily) was matched in healthy group; in the group of cancer patients, mean smoking duration was equal to 34±1 years and frequency of smoking was 20±1 cigarettes daily (34.0± 1 pack years). Experimental information We carried out a comparative study of the activity of five AO enzymes: superoxide dismutase (SOD), glutathione peroxidase (GPx), glutathione reductase (GR), glutathione transferase (GST) and catalase, the number of single-stranded (SSB) and double-stranded breaks (DSB) in leukocyte DNA, the level of malonic dialdehyde (MDA) in erythrocytes, degree of its hemolysis and membrane micro viscosity at the surface of lipids (tC1 ) and in the protein-lipid membrane regions (tC11 ), in groups of healthy subjects and cancer patients. Fasting blood samples were collected into "BD Vacutainer TM" test-tubes (Becton Dickinson Immunocytometry Systems-BDIS, USA), which were stored and transported in a vacuum flask filled with ice. DNA was isolated from human blood using Diatom DNA Prep 400 reagents (Isogen Laboratory, Russia). Cells were lysed with a reagent comprising guanidine thiocyanate, simultaneously solubilizing cell debris and denaturizing cellular nucleases. DNA was adsorbed on NucleoS sorbent, other components of the cell (proteins etc) were washed off with a salt / alcohol solution and DNA was eluted using ExtraGen E. The obtained DNA preparations were of homogeneous molecular mass of about (14 ± 1) l0 6 Da. Determination of the number of DNA breaks was performed by the standard 0.7% agarose gel electrophoresis in neutral or alkaline buffer. [7] All the reagents were purchased from "Serva" (USA). The gels were visualized using the Gel Imager 2 system. The number of DNA breaks was quantified by scanning the gel images using Scion Image Beta 4.0.2 software. The mean value of strand breaks per DNA molecule (N) was derived from the formula: S / (S 0 -S) = exp -N , where S is the peak area limited by the maximum ordinate, S 0 - is the total peak area of DNA. [8] Membrane micro viscosity was measured by spin-probe method [9] using of stable iminoxyl radicals as probes: 2, 2, 6, 6-tetramethyl-4-capryloyloxypiperidine-1-oxyl (Probe 1), which localizes at the surface sites of lipids and 5,6-benzo-2, 2, 4, 4-tetramethyl-l, 2, 3, 4-tetrahydro-y-carbolyn-3-oxyl (Probe 2), which localizes at the paraprotein sites of lipids. The probes were introduced in the final concentration of 10 -4 - 3 Χ 10 -5 M into a suspension of erythrocytes in an alcohol solution 20-30 min before EPR-spectrometric measurements of the samples. From the spectra recorded on a Brucker-2000 EPR-spectrometer the rotary correlation time τC (τC1 for probe 1 and τC11 for probe 2), which corresponds to the period of a radical reorientation by an angle of π/2, was calculated by the formula for rapidly rotating radicals: τC = 6.65ΔH +1Χ((I +1 /I -1 ) 1/2 - 1)10 -10 , sec. ΔH +1 is the width of a low-polar component of the spectrum, I +1 and I -1 are the intensities of a low- and a high-polar component of the spectrum, respectively. Determination of MDA (TBARs) levels in blood samples was performed by means of a standard spectrophotometric thiobarbituric acid assay. [10] The degree of erythrocytes hemolysis in blood was studied in 5% suspension in 0.05 M Tris-HCl buffer (pH 7.2-7.4) by measuring the optical density at 532 nm. Spectrophotometric measurement of the activities of antioxidative enzymes was performed in centrifuged blood probes (at 1500 rpm for 10 min) with subsequent plasma separation. The erythrocytes were washed with isotonic saline solution, and lysed by addition (1/5 v/v) of double distilled water. Samples were stored at - 70ºC prior to analysis. The activity of superoxide dismutase (CuZnSOD) was derived from inhibition of the reduction of nitroblue tetrazolium (NBT) by superoxide radicals generated in the xanthine oxidase-catalyzed oxidation of xanthine. The unit of activity is the amount of the enzyme that inhibits the rate of formazan dye formation by 50% per mg of hemoglobin content in the sample. [11] The activity of glutathione peroxidase (GPx) was derived from oxidation of reduced nicotin amid- adeninedinucleotide phosphate (NADPH) in a conjugated GR system using tertbutyl hydroperoxide as a substrate. [12] The activity of glutathione reductase (GR) was derived from oxidation of NADPH. The unit of activity for GP and GR is the amount of the enzyme that catalyzes the conversion of 1μmol of substrate per one minute. [13] The activity of glutathione transferase (GST) was determined based on the accumulation of thio-ethers from l-chloro-3.4-dinitrobenzene with reduced glutathione. [14] The activity of catalase was derived from the changes in the optical density at D 240 as result of the decomposition of hydrogen peroxide . The unit of activity is the amount of hydrogen peroxide in μmol decomposed per one minute. [15] The activity of all the enzymes (except SOD) was calculated per gram of hemoglobin content in the sample. Concentration of hemoglobin was determined from. [16] Statistical analysis of the obtained results was carried out. Since not all parameters had a normal distribution, values of Median (lower quartile - upper quartile) were calculated. Statistical significant differences between the parameters in groups were evaluated by using the nonparametric Mann-Whitney criterion. The correlations between parametric variables were evaluated using Pierson's method, or Spearmen's method in case of nonparametric variables. The level of significance was P < 0.05. A multi-factorial analysis of cancer incidence among cigarette smokers was performed using binary logistic regression with approximation to the regression model by means of the forward stepwise method in the Statistical Package for the Social Sciences (SPSS). Ethics Collection of venous blood samples and data processing were conducted in full compliance with the principles of World Medical Association Declaration of Helsinki "Ethical Principles for Medical Research Involving Human Subjects" (Helsinki, 1964, as amended during 1975-2000) and the current legislative and government regulations of the Russian Federation, including the Fundamentals of the Legislation of the Russian Federation on Health Protection of the Citizens, 1993, and the Law of the Russian Federation "On Personal Data" No.152-FZ, 2006. All data and the personal information collected in this study are subject to medical confidentiality and may only be brought together for processing and evaluation in an anonymous form. Blood samples were taken from all subjects following their signing the informed consent to participate in the study. The ethical approval has been obtained and informed consent was given by each subject. Results Antioxidant enzymes, membrane micro viscosity were analyzed in erythrocytes and DNA breaks in leukocytes of peripheral human blood. We have estimated an influence of smoking on healthy subjects and cancer patients. [Table - 1] lists values (as medians) of all measured parameters in cancer patients group and in healthy group. This table shows the blood parameters values (as median) of two main groups (healthy humans and cancer patients). Each main group included two sub-groups such as smokers and nonsmokers. Statistical comparison between the groups was performed. It was shown that smoking led to increasing activity of GPx (P 0.038) in healthy group. In healthy subjects, the trend of increasing SOD activity and DNA double-strand break (DSB) number was seen when comparing non-smokers and smokers. This increase was confirmed in non-smokers compared with high intensity smokers (P < 0.05 for both parameters). In contrast with healthy group, no significant influence of smoking was found in cancer patients. There was no statistically significant distinction in studied parameters between smoking and non-smoking cancer patients. We have compared smoking and non-smoking groups of cancer patients with matched groups of healthy subjects [Table - 2]. The comparison of the parameters for these groups showed a statistically significant increase in the number of leukocyte DNA DSB [Figure - 1], SSB [Figure - 2] and in GST activity [Figure - 3] in smoking cancer patients compared with smoking healthy subjects. The increase in number DNA SSB and GST activity and decrease of parameter τCII were observed also in non-smoking patients [Table - 1] and [Table - 2]. The GST activity and number of DNA SSB were independent on smoking in the group of healthy subjects as well as in the group of cancer patients. This suggests that the increased level of these parameters in cancer patients is caused by the development of pathological process. [Table - 1] also shows the decreased level of GPx and SOD activities in smoking patients compared with healthy smokers. However, no difference between these parameters was found in the both groups of non-smokers, as soon as between smoking and non-smoking patients [Table - 2]. Statistical analysis showed that GPx and SOD activities in cancer patients were not different also from those in healthy non-smokers. These data suggest that the decreased activities of GPx and SOD in smoking patients compared with healthy smokers were due to the increase of these activities in healthy smokers as result of smoking. We also evaluated relationships between various parameters in groups of healthy subjects and cancer patients by the correlation analysis. [Table - 3] lists the relationships between blood parameters in entire healthy group and in healthy smokers. It is seen that the duration of smoking correlates with age of smokers and frequency of smoking correlates with GP activity (P < 0.05). [Table - 4] shows the correlations in the cancer patients group and reveals that they differ from the healthy group. In the cancer patients group, there are no correlations of GST activity with other AO enzymes (SOD and catalase) and with markers of oxidative damage (MDA, SSB) observed in the healthy group. However, there are correlations of SOD activity with DNA SSB and GR activity. Besides, the correlations of erythrocyte hemolysis (reflecting structural and functional changes of membranes) with oxidative stress markers (DNA SSB and DSB) become apparent. The correlations were revealed between age and duration of smoking, the smoking frequency correlated with GR activity and malonyldialdehyde (MDA) level (P < 0.05). Although smoking did not affect the parameters of patients, the correlations in the groups of smoking and non-smoking patients were different. The correlations observed in smokers are substantially the same as in the entire group of cancer patients. This is explained to the prevalence of smokers (n = 34) over non-smokers (n =16) in this group. In non-smokers the correlations of hemolysis stability with GPx and parameter τCI with GR activity were observed. The data obtained permit to conclude that the revealed difference of the correlations between the group of patients and the healthy group is a consequence of the pathology development. Multi-factorial analysis revealed a regular dependence of cancer occurrence with the parameters presented for the analysis. Binary logistic regression served as a basis for the present investigation. A statistical analysis identified the summarized model of the following view:
where P is the probability of cancer incidence, Z = Constant + B0 Χ AGE + B1 Χ (DSB Χ Cat) + B2 Χ (SSB Χ GT) + B3 Χ (τCII Χ GP) + B4 Χ (Hemol Χ GP) Z = - 9.7 + 0.141 Χ AGE + 0.033 Χ (DSB Χ Cat) + 1.684 Χ (SSB Χ GT) - 0.09 Χ (τCII Χ GP) + 0.003 Χ (Hemol Χ GP) Thus, the calculated coefficients enable us to determine a probability of cancer incidence (P) for a certain case using values of eight parameters: age, SSB, DSB, catalase, GT, GP, τCII, and erythrocyte hemolysis. The calculated probability of cancer incidence was equal to > 0.6 in 12% of the healthy non-smoking and smoking subjects, whereas the P value was equal to 0.999 in 93% cases of cancer patients. The results obtained for the examined healthy subjects could be interpreted as the evidence for an elevated cancer risk for 12% of healthy subjects. Thus, we can assume that this statistical model could be useful in investigation of larger human cohorts, as well as in creating a diagnostic test for elevated cancer risk. Discussion The damages caused by ROS of tobacco smoke occur as a consequence of an imbalance between the generation and detoxification of these species. Defense against oxidative stress is provided by a system of enzymes and antioxidants capable of preventing an excess production of ROS and neutralizing free radicals. [4] Free radical-scavenging enzymes such as superoxide dismutase (SOD), catalase (CAT) and glutathione peroxidase (GPx) are the first line of cellular defense against oxidative injury, decomposing superoxide radicals and H2O2 before interacting to form the more reactive hydroxyl radicals, which damage DNA and lipids of membrane. GST play an important role in the protective mechanisms catalyzing the conjugation of reactive electrophilic agent to glutathione (GSH) and the reduction of lipid hydroxides. The published data on the smoking influence on the antioxidant enzymes and the level of MDA in blood plasma of healthy subjects are contradictory. In various studies on healthy smokers, it is observed as an increase [17] or reducing [18] and even absence [19],[20] of changes in enzyme activities. We found no change in the level of MDA, in smokers, which is consistent with the data given in. [21],[22],[23] At once, an intensification of lipid peroxidation was observed at work. [24] We found that in high intensity smokers, the number of DNA DSBs is significantly higher than in non-smokers, which is consistent with the data given in. [25] The above discrepancies in results may be explained by variability in the studied parameters caused by the effects of age, moderate alcohol consumption, drugs and dietary supplement use. [1] Extensive epidemiological [26] and statistical date [27] clearly establish role of cigarette smoking in the genesis of lung cancer and head and neck cancer. It is known that neoplastic transformation is accompanied by changes in AO status, [28] in the extent of lipid oxidation, [29],[30],[31],[32] micro viscosity of membranes and lipid composition [33],[34] and an increase of DNA breaks number in both tumor tissue and leukocytes of blood. [35],[36],[37],[38],[39] The changes in these parameters indicate the involvement of oxidative stress in the process of malignancy. In our extensive study, we have found statistically significant difference between parameters in cancer patients and healthy subjects. In addition, it should be noted the homogeneity in the age of healthy subjects and cancer patients studied groups. Oxidative DNA damage in blood and other human tissues were detected in our study and in investigations of various types of cancer. We observed two-fold increase of DNA DSB and SSB levels in blood of cancer patients compared to healthy subjects. Increased level of oxidative DNA lesions (DNA breaks, 8-hydroxy-deoxyguanosine) in blood and other human tissues was detected also in other studies on various types of cancer. [35],[36],[37],[38],[39] The reduced DNA repair capacity observed in human carcinogenesis [40],[41] and a weakening of AO enzymes system are likely to be reasons for enhanced level of DNA breaks measured in our study. We have shown that the GST activity increased significantly in the groups of cancer patients compared to healthy subjects. This result is in agreement with previous reports of other research groups. [17],[42] It is known that GST is involved in detoxification of carcinogens including those contained in tobacco smoke. The role of GST in modulating susceptibility to smoking-related lung cancer, [43] oral cancer [44] and chronic obstructive pulmonary disease [45] is the object of current intensive study. The decrease of GPx and SOD activities observed in the group of cancer patients as compared to healthy subjects is consistent with the published data on the changes of antioxidant enzymes activity during cancer development. [18],[46] However, in these works, the results are considered without drawing attention to smoking status of healthy subjects and cancer patients. Our results show that the levels of GPx and SOD activities in non-smoking patients are not different from smoking patients and non-smoking healthy subjects. As a result, we note the loss of sensitivity of these AO enzymes to smoking among patients and the absence of a response of AO enzymes, except for GST, in course of pathological process. We believe that these facts indicate a weakening of AO enzymes system. The elevated lipid peroxidation and decline in enzymatic antioxidant status were noticed previously in oral cancer and other types of cancer. [29],[30],[31],[32] Our study found a reduction of erythrocyte membranes micro viscosity in protein-lipid regions (τCII ) in cancer patients, which is consistent with data of authors who have reported analogous structural changes in cell membranes in patients with other cancer diseases. [33],[34] The correlation of AO enzymatic activity and MDA level in erythrocytes was obtained with the stage of lung cancer of patients. [47] We found no change in the MDA level, which is consistent with the work [48] about the absence of changes in total antioxidant status and MDA levels in patients with oral cancer. Previously, it was found that in the development of tumor process the total antioxidant status changes depending on the cancer stage: in initial period its level is increased compared with control, but later it decreased. [49] The lack of significant differences between MDA levels of patients and healthy subjects may be due to this phenomenon. Overall, cancer is characterized by a certain damage in DNA structure, decrease in viscosity of erythrocyte membrane, weakening of AO enzymes system in patients. These results indicate that the studied parameters of the AO status in human blood are changed by a tumor process, thus indicating the augmentation of oxidative stress. One can assume that the level of studied markers as well as the presence or absence of correlations between parameters in patients group might have a prognostic importance for healthy smoking subjects. The above analysis of the selected oxidative stress markers in human blood showed their utility for detection smoking-induced harm in healthy subjects and cancer patients. This study also demonstrates a potential applicability of the statistical model based on the evaluated oxidative stress markers in the blood of healthy non-smokers and smokers to determine the risk of cancer incidence in these subjects. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10011f2.jpg] [cr10011f1.jpg] [cr10011t3.jpg] [cr10011t4.jpg] [cr10011t2.jpg] [cr10011t1.jpg] [cr10011f3.jpg] |
| |||||||||

 (1)
(1)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}