 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
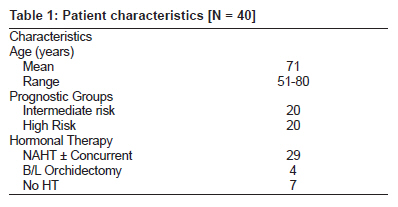
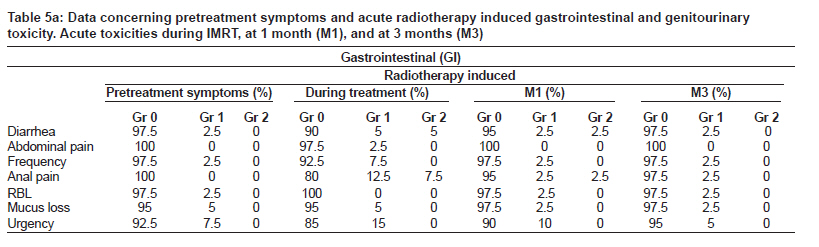
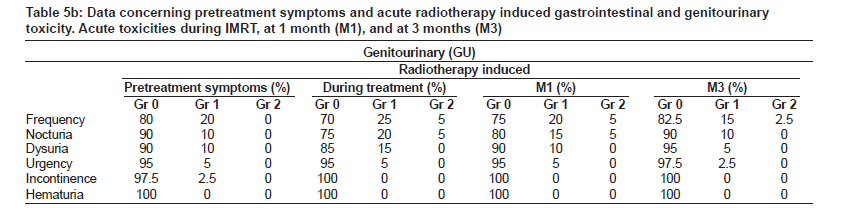
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 58-64 Original Article High-dose intensity-modulated radiotherapy as primary therapy for prostate cancer: Report on dosimetry aspects and acute toxicity in the Indian scenario Sandeep De, Venkatesan Kannan, Sudesh Deshpande, Vivek Anand, Yogesh Ghadi Department of Radiation Oncology, P. D. Hinduja National Hospital and Medical Research Center, Veer Savarkar Road, Mahim, Mumbai, Maharashtra, India Code Number: cr10013 DOI: 10.4103/0973-1482.63565 Abstract Background and Purpose: Dose escalation improves local control in prostate cancer. In this study we assess the feasibility of dose escalation to prostate and / or seminal vesicles to 76 Gy with intensity-modulated radiotherapy (IMRT); report data on dosimetry and acute toxicity in 40 patients at P. D. Hinduja National Hospital and Medical Research Center, Mumbai. Materials and Methods: In the period from May 2006 to September 2008, 40 consecutive patients with localized prostate adenocarcinoma (T1- 3 N0) were definitively treated with IMRT to a dose of 76 Gy / 38 fractions. Patients were seen on a weekly basis during treatment, and one month (M1) and three months (M3) thereafter. The radiation therapy oncology group (RTOG) toxicity scale was used to evaluate acute gastrointestinal (GI) and genitourinary (GU) toxicities. Additional symptoms such as rectal blood loss, urgency, dysuria, urinary frequency, nocturia, incontinence were scored as well. Results: All 40 patients completed treatment successfully. Acute RTOG Grade 1 and Grade 2 GI toxicities were noted in 47.5% (19 patients) and 12.5% (five patients) respectively, leaving 40% (16 patients) free of any acute toxicity. Thirty-six (90%) and four patients (10%) had Grade 0-1 and Grade 2 acute RTOG-scaled GU toxicity respectively. There was no Grade 3 or higher GI / GU toxicity. Conclusions: The escalated dose of 76 Gy to the prostate with IMRT was very well tolerated by all our patients with acceptable acute GU and GI toxicity, thereby, establishing the feasibility of dose escalation in the Indian scenario.Keywords: Prostate cancer, intensity-modulated radiotherapy, dose escalation, acute toxicity Introduction Randomized dose-escalation trials with three-dimensional conformal radiotherapy (3DCRT) have confirmed that high-dose of radiotherapy (RT) improves biochemical-no evidence of disease (bNED) outcome and freedom from failure (FFF) rate in localized adenocarcinoma of the prostate. [1],[2],[3],[4] However, the improved biochemical control in dose escalation studies with 3DCRT was also associated with an increased rate of late complications, particularly late gastro-intestinal (GI) toxicity. [1],[4] Intensity-modulated radiotherapy (IMRT) by producing highly conformal dose distribution facilitates selective dose escalation to the target volume with reasonable sparing of normal tissues, thereby, producing better biochemical control rates without compromising the risk of acute and late complications. [5],[6],[7] Acute rectal toxicity remains important as a predictor of late rectal toxicity. [8],[9] We have already reported the results of prostate patients treated with 3DCRT at our hospital. [10] But there is dearth of IMRT data on prostate cancer from the Indian sub-continent. We present here dosimetric data and results on acute toxicity of 40 patients treated in our hospital, a tertiary community hospital, with anatomy-based IMRT as primary therapy for localized prostate cancer. Materials and Methods Patient characteristics In the period from May 2006 to September 2008, 40 consecutive patients with localized prostate cancer (T1-3N0) were treated in our hospital with definitive IMRT. All patients were histopathologically proven cases of adenocarcinoma. Patients were divided into prognostic subgroups based on T-stage, pre-treatment prostate-specific antigen (PSA) level and Gleason score. [11] All patients with intermediate and high risk diseases had undergone a metastatic work-up and had no evidence of metastatic diseases. The distribution of patient age, prognostic risk-group stratification and details of use of hormone therapy are given in [Table - 1]. TNM staging was scored according to the American Joint Committee on Cancer (AJCC) staging guidelines 2002. To determine T-stage, the information from digital rectal examination was supplemented with computed tomography (CT) scan and magnetic resonance imaging (MRI) scan data. Hormonal therapy (HT) consisted of luteinizing hormone releasing hormone (LHRH) analog (29 patients) or bilateral orchidectomy (four patients, done elsewhere before reporting here) in intermediate or high risk patients. The first injection of LHRH analog was given within one to three months before the start of radiotherapy. The intake of anti-androgens started four to seven days before the first LHRH analog injection and was continued for about one to four weeks. Depending on the risk category subgroup, HT was continued for six months to two years duration. Treatment planning and dose prescription All patients were immobilized from gluteal region down to the toes, in supine posture with upper limbs on chest, using a vacuum cushion device. Planning CT scan was done in 64 multislice hi-speed spiral GE-CT scanner, with patient in treatment position, from L5-S1 junction to 10 cm caudal to the ischial tuberosities. CT scans were taken with 2.5 mm slice thickness with intra-venous non-ionic contrast injection in all patients, unless otherwise contraindicated for some reason. All patients had radio-opaque localization markers fixed during the planning CT scan on three tattoos done on the patient body after localization with fluoroscopic simulation of the patient - one in the midline at a point located 0.5 cm inferior to the superior edge of the symphysis pubis and one each on the lateral aspect of the hip defined at a depth of 10 cm from the anterior midline point (at a depth of 90 cm). MRI scans used for image fusion and planning were acquired on 1.5 Tesla GE Sigma twin speed machine using T-2 weighted images (WI) with patient in treatment position; using a pelvic phase-array coil. MRI scans were taken in 3 mm slice thickness through the level of seminal vesicles and prostate decided from sagittal and coronal tomograms. Flat top couch was used for CT scan. Hard bed was used for MRI scan to achieve near similar position to that of the CT scan. We used MRI routinely in all patients for better delineation of the prostate base-bladder and prostate apex-rectum interfaces. For all patients a policy of active emptying of the rectum in the morning and that of the urinary bladder just before entering the CT/MRI scan room was followed. By performing planning CT/MRI scans with the rectum empty, the proportion of the rectum treated above the constraint threshold will be at the highest possible - a worst case scenario. Since most patients have more increased bowel movements and, consequently, a reduced rectal volume in the latter half of RT, this maneuver makes simulation more representative of the extent of rectal filling during actual treatment. The interval period between acquiring the planning CT scan and MRI scan was kept as minimum as possible to prevent any change in the shape and filling of the rectum and the bladder. Planning CT scan and T-2 W MRI images were transferred and fused in the BrainLab IMRS planning system (BrainLab, Germany) using the automated fusion algorithm. The clinical target volume (CTV) was delineated using the fused images by the radiation oncologist in consensus reading with a radiologist. Critical organs like rectum, urinary bladder, sigmoid colon were all contoured. Specifically, the rectum (as a solid organ) was contoured from the level of the anal verge to the recto-sigmoid junction. The bladder was contoured in its entirety from the apex to the base. The CTV-1 included the prostate and bilateral seminal vesicles (SV). The planning target volume (PTV)-1 was created using a three-dimensional, anisotropic expansion of the CTV-1 by 10 mm (except at the prostate-rectum interface where the margin was 6 mm). The seminal vesicles were excluded from the CTV-1 at a dose of 50 Gy for T1and T2 disease and at a dose of 60 Gy for T3a disease respectively. The CTV-2 included the prostate only (except for T3b disease where the proximal bilateral SV were also included in the CTV-2 volume). The PTV-2 was created by an anisotropic expansion of the CTV-2 by 8 mm (5 mm on the prostate-rectum interface). A total dose of 76 Gy / 38 fractions to the prostate was prescribed at 95% isodose level, thereby, delivering a dose of 79.8 Gy to the isocenter (ICRU reference point). Patients with T1 and T2 disease received 50 Gy/ 25 fractions and T3a disease received 60 Gy / 30 fractions to the seminal vesicles, followed by boost dose of 26 Gy / 13 fractions and 16 Gy / 8 fractions respectively to the prostate only volume. For T 3b disease, the dose to the proximal bilateral seminal vesicles was also taken up to 76 Gy / 38 fractions in entirety. For the IMRT planning, isocentric seven-field and five-field techniques were used for the PTV-1 and PTV-2 respectively. PTV-1 planning included the following beam directions: two left anterior oblique (24° and 75°), a left posterior oblique (123°), a direct posterior (180°), a right posterior oblique (231°), two right anterior oblique(282° and 333°). For PTV-2 planning the beam directions were as follows: a left anterior oblique (45°), a left posterior oblique (100°), a direct posterior (180°), a right posterior oblique (260°) and a right anterior oblique (315°). [12] IMRT planning was done on the BrainLab IMRS planning system. The desired beam intensity profiles were delivered by dynamic multileaf collimator (DMLC). Delivery of IMRT was carried out using the sliding window technique. As part of the quality assurance program, point dose verification and film dosimetry were carried out before treatment for each patient. The IMRT plan approval to a dose of 76 Gy was based on meeting the dose volume histogram (DVH) constraints. PTV coverage was the priority to ensure that 95% of the PTV and 100% of the CTV receive the prescription dose. The minimum dose to the prostate should be above 65 Gy. Maximum dose to the PTV should not exceed 17% above the prescription dose. The DVH threshold constraint for rectum for plan approval was that < 17% and < 35% of the rectal volume should receive a dose over 65 Gy and 40 Gy respectively. The DVH constraints for the bladder were set at < 25% of the bladder volume to be treated over 65 Gy and < 50% over 40 Gy. [13] On examination of the isodose lines on CT slice-by-slice basis, our attempt was to see that the 90% line falls at less than half the width posteriorly and the 50% line falls at less than half the full width posteriorly. [13] The dosimetric parameters examined for the rectum included the maximum dose received by 17% (D17), 35% (D35), 50% (D50), 60% (D60) and 70% (D70), respectively, of the volume of the rectum and the maximal rectal dose (Dmax). Similarly, for the bladder, the dosimetric parameters evaluated were the maximum dose received by 25%, 50%, 60% and 70% (D25, D50, D60, and D70) of the bladder volume respectively and the maximal dose to the bladder (Dmax). For all patients treatment was delivered with 6 / 15 MV photons in a Varian 2300 CD linear accelerator (Varian medical system, Palo Alto). Orthogonal portal imaging through electronic portal imaging device (EPID) in anterior-posterior and lateral directions were acquired on first 3 days of starting IMRT. Tolerance for acceptability was 3 mm in all directions based on bony anatomy, beyond which on-line correction was done. After applying correction for any systematic error off-line, EPID was done once weekly or more frequently till the completion of the entire treatment. Toxicity During treatment, patients were seen on a weekly basis and as and when required in between. Follow-up was performed at one month (M 1) and three months (M 3) after the end of treatment and thereafter every three months for the first year. Further follow-up was planned at every six months thereafter. Acute toxicity was defined as an occurrence and/or increase of any toxicity during radiation and/or within three months after the end of radiation treatment. [14] The grade of acute toxicity (gastro-intestinal and genitor-urinary) was scored and graded according to the radiation therapy oncology group (RTOG) toxicity scale. [15] There have been a few limitations, which include certain symptoms in the RTOG acute toxicity scoring system; and multiple adaptations have been made by various authors over the years concerning various GI and GU toxicity criteria and grading pattern. [14],[16],[17],[18] Hence, to include all toxicity data in a single score and to allow multivariate analysis of the acute toxicity data with continuous variables given by the planning system, the following two continuous variables were introduced:
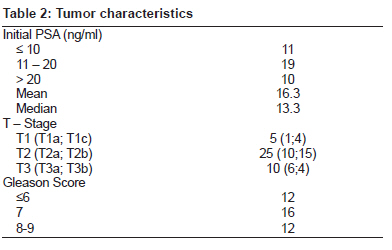
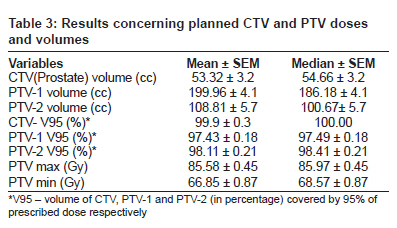
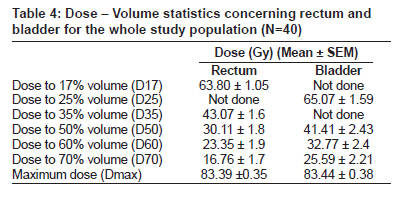
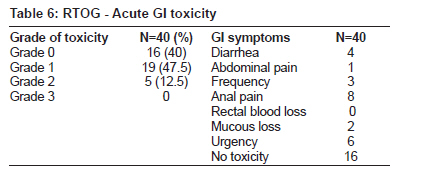
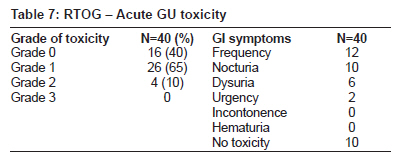
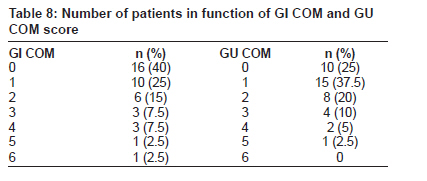
For GICOM, seven symptom scores were used: diarrhea, rectal blood loss (RBL), mucus loss, abdominal cramps, urgency, frequency and anal pain. For GUCOM scores, six different symptoms were measured: daily frequency, nocturia, dysuria, hematuria, urgency, and urinary incontinence. For each symptom, the maximal toxicity score in the time period from the start of IMRT up to and including the third month after therapy was registered. The sum of all the maximal symptom scores was the GICOM and GUCOM. The range of GICOM is 0 (not a single toxicity during the whole treatment) to 21 (seven symptoms with Grade 3 toxicity). The range of GUCOM is 0 to 18 (six symptoms with Grade 3 toxicity). Pearson's correlation coefficient was used to compare GICOM and GUCOM with treatment-related parameters; and a two-sided P value of ≤ 0.05 was considered significant. Result The overall tumor characteristics are summarized in [Table - 2]. All 40 IMRT plans were delivered successfully without any interruption and / or technical problem. Daily treatment time was 20 minutes in all cases and less than 15 minutes in 90% of cases. Prescribed doses and dose-volume parameters of CTV, PTV, rectum and bladder The total prescribed dose to the prostate (± bilateral SV) was 76 Gy / 38 fractions, prescribed at 95% isodose level in a phased manner. [Table - 3] lists the planning results concerning the CTV and PTV. The mean rectal volume was 68.83 ± 5.9 cc. The mean bladder volume was 146.75 ± 4.2 cc. The dose-volume parameters of the rectum and the bladder are presented in [Table - 4]. In most of the patients (36 patients), the dose-volume values for the rectum were within prescribed constraints. The cut-off points exceeded in four patients for rectum D17 and D35 (68.40Gy and 45.23 Gy; 69.50 Gy and 50.10 Gy; 71.10 Gy and 52.75 Gy; and 70.27 Gy and 46.48 Gy) respectively. In case of bladder the cut-off points exceeded for D25 and D50 in 5 patients (70.74 Gy and 56.94 Gy; 68.26 Gy and 47.10 Gy; 66.76 Gy and 50.23 Gy; 74.70 Gy and 55.50 Gy; and 68.17 Gy and 54.30 Gy) respectively. The maximum dose to femoral heads and penile bulb was 58.75 Gy ± 1.2 Gy and 55.25 Gy ± 2.4 Gy respectively (expressed as mean ± standard error of the mean). Acute GI toxicity The results concerning pretreatment symptoms and radiotherapy-induced acute toxicity (during RT, at M1 and M3) for all patients are summarized in [Table - 5a] and [Table - 5b]. Before the start of IMRT, RBL was observed in one patient. He presented with bleeding hemorrhoids. But during radiotherapy he had no symptoms of rectal blood loss though he had Grade 2 anal pain. However, the same patient had complaints of rectal blood loss at M1 and M3. Overall, there was no RT-induced Grade-3 or Grade-4 acute RTOG-scale toxicity [Table - 6]. We observed Grade-2 acute toxicity in five patients (12.5%) - mainly diarrhea (n = 2) and anal pain (n = 3). Nineteen patients (47.5%) developed Grade-1 acute GI toxicity - mainly urgency (n=6), anal pain (n=5), increased frequency (n=3), mucous loss (n=2), and diarrhea (n=2). Sixteen patients (40%) were free of any acute toxicity. All Grade-1 and Grade-2 toxicities according to the RTOG toxicity score decreased with time, including urgency. Acute GU toxicity The acute RTOG-scaled toxicity profile during the whole treatment period was very much favorable [Table - 7]. No patient had any Grade-3 or higher GU toxicity. Only four patients developed Grade-2 GU toxicity (10%), mainly nocturia (n=2) and frequency of urination (n=2). Grade-1 GU toxicity was observed in 26 patients (65%). The main Grade-1 GU toxicities seen were frequency (n=10), nocturia (n=8), dysuria (n=6), and urgency (n=2) respectively. All Grade 1 and 2 toxicities decreased with time. We did not find any correlation between any of the separate acute GI as well as acute GU toxicity scores and the physical rectal and bladder dose parameters respectively. The data concerning GICOM and GUCOM are presented in [Table - 8]. Maximal GICOM was 6 (one patient). There was a significant correlation between GICOM and rectal D17 and D35 (P = 0.01), D50 and D60 (P = 0.03). GICOM was also significantly correlated with minimal and maximal PTV dose (P = 0.01 and P = 0.04, respectively). The maximal GUCOM was 5 (one patient). But there was no statistically significant correlation between GUCOM and the physical bladder end points. Discussion The present series, to our knowledge, represents the first compilation of IMRT-treated patients in the Indian subcontinent and demonstrates the feasibility of high-dose radiation delivery with IMRT for patients with localized prostate cancer in the Indian scenario. The intent of our study was not to compare outcome with lower dose levels delivered in other centers, but to report the feasibility and tolerance of 76 Gy IMRT in this cohort of patients. We present here details on dose-volume histograms and report on the time evolution of radiotherapy-induced acute GI and GU toxicity. We routinely do MRI-CT scan image fusion to plan for all our prostate cancer patients. A couple of studies [19],[20] have shown that prostate volume delineated on MRI usually is around 30% lesser compared to that done on CT images for prostate cancer. The dose-volume histograms resulting from CT and MRI comparison show that it is possible to spare a mean 10% of rectal volume and approximately 5% of bladder when MRI based contouring is used for planning. [20] During MRI scan, hard bed was used for patient positioning so as to achieve the flat table top position of CT scan. This was done to reduce/prevent the ventral shifting of the rectal wall, which was observed by Steenbakkers et al. [19] The dose-volume relationships for rectal and bladder complications are a continuous function and not adequately described by a single point. [13] As addressed by Pollack et al. we have reduced our dose-volume histogram (DVH) threshold for plan approval from < 25% of the rectal volume treated over 70 Gy to that of < 17% over 65 Gy. [13] In four cases where the DVH constraints for the rectum were not met, the plan was accepted when the DVH values were within 7% of the target limitations. Skwarchuk et al. have shown that when the 50% isodose line encloses the outer rectal wall on the central slice, the complication risk is significantly elevated. [8] Our plan evaluation criteria were similar. It was made sure that the 50% isodose line never covers the entire anterior-posterior dimension of the rectum fully, thereby sparing the posterior aspect of the rectal wall. We tried to supplement our toxicity scales and match them as closely as possible to the original RTOG scale, when any symptom out of RTOG scale was seen (e.g. anal pain and urgency for stools). Urgency, anal pain, or a combination of both symptoms was seen in 27.5% (Grade 1) and 7.5% (Grade 2) of our patients respectively. Urgency has been considered an important radiotherapy-induced acute morbidity and reflects heterogeneous changes in anorectal function [21] and significantly predicts for late fecal urgency. [9] The major clinical advantage of IMRT has been its ability to decrease rectal toxicity. [22],[23] IMRT by achieving significant reduction in acute GI toxicity could be partially responsible for the subsequent reduction in late GI toxicity. Several studies [24],[25],[26] have concluded that acute GI toxicity and, more specifically, acute proctitis were significant predictors of late GI toxicity, suggesting a significant consequential component in the development of late Grade 2 and greater GI toxicity. In most reports, no correlation between rectal dose-volume histograms and acute rectal toxicity could be found. [17],[27] However, Peeters et al. from the Dutch group demonstrated a correlation between rectal dose-volume and acute toxicity. [28] We did not find any correlation between any of the separate acute GI toxicity scores and the physical rectal dose parameters.[Table - 4] But "Composite GI toxicity score" was significantly related to most of the above-mentioned rectal dose parameters. Regarding GU toxicity - Peeters et al.[28] assessed absolute and relative bladder surface receiving ≥ 5 - 65 Gy (S5-S65), from dose-surface histograms (DSHs) of the bladder surface computed from three-dimensional binary bladder volume. They found a significant correlation between acute GU toxicity and aS40, aS45 and aS65 on multivariate regression analysis. In our analysis, though the corresponding bladder doses were decreased with IMRT in our patients [Table - 4], we did not find any correlation between any of the separate acute GU toxicity scores and the physical bladder dose parameters. Other studies [17],[18],[29] also reported no relationship between acute GU toxicity and any bladder dosimetric parameters. These findings, along with ours, support the notion that most of the acute GU toxicity is related to the RT effect of inducing edema and inflammation in the prostate and the prostatic urethra rather than in the bladder. Zelefsky et al. reported on acute toxicity in 772 patients treated to at least 81 Gy with IMRT. [11] Acute Grade 2 GI toxicity was observed in 4.5% of patients. Grade 2 acute GU toxicity was reported in 28% of patients. Our grade 2 acute GI and GU toxicity was higher than that reported by Zelefsky et al. Two important factors could account for this difference. First, the RTOG scale tabulated in 1991 [30] was used by Zelefsky et al. which differs from the one we used. Secondly, with the prescribed dose of 81 Gy to the target, the overlap region between the PTV and the rectum was limited to 88% of the prescribed dose (i.e. 71.3 Gy in 1.58 Gy fractions, BED a / b=10 = 85.6 Gy). This is lower than the maximal rectal dose of at least 76 Gy (at 2 Gy fractions) we used in all our patients (BED α / β = 10 = 91.2 Gy). Teh et al. reported on 100 patients treated with IMRT definitively to a prescribed dose of 70 Gy (mean doses to the prostate and seminal vesicles were 75.8 and 73.9 Gy) with the use of a rectal balloon for prostate immobilization. [31] They reported acute Grade 1 toxicity in 11%, Grade 2 toxicity in 6% and no GI toxicity in 83% of patients respectively. They attributed the favorable GI toxicity profile to the use of the rectal balloon which lowers the mean rectal dose (35 Gy) and the volumes receiving greater than 60, 65, or 70 Gy. But no statistically significant relationship was found between acute toxicity and rectal dose-volume parameters. The use of rectal balloon may reduce rectal dose. De Meerleer et al. reported on 114 patients treated with IMRT with three dose levels of 72 Gy, 74 Gy, and 76 Gy, as the primary treatment; with the most detailed and composite data on GI and GU toxicity scores. [14] Grade 1 and Grade 2 GI toxicities were observed in 44% and 29% of the patients respectively. If only the RTOG scale was used, Grade 1 and Grade 2 GI toxicities were noted in 39% and 27% of the patients respectively, leaving 34% free of acute RTOG-scaled toxicity. Grade 3 GU toxicity was seen in 7% of patients. Grade 2 and Grade 1 GU toxicities were seen in 36% and 47% of the patients respectively, leaving only 10% free of acute GU toxicity. Our Grade 2 GI and GU toxicity was lesser (12.5% vs. 27%) and (10% vs. 36%). Fonteyne et al. reported on 230 patients treated with IMRT to 78 Gy and simultaneous integrated boost (SIB) to patients with intra-prostatic lesion (IPL) to 81-82 Gy. [32] Grade 2 acute GI toxicity was seen in 11% of patients. No Grade 3 or higher toxicity was noted. Grade 2 and 3 acute GU toxicity was reported in 41% and 7% patients respectively. Our acute GI toxicity is comparable, though our acute GU toxicity was much less and we didn't have any Grade 3 toxicity. In the Dutch trial, 78 prostate cancer patients were treated to a total dose of 78 Gy with either a 3DCRT technique with a sequential boost (SEQ) or a simultaneous integrated boost using IMRT (SIB-IMRT). [5] In the SIB-IMRT arm, Grade 2 or greater acute GI toxicity was significantly lesser than the SEQ arm (20% vs. 61%; P=0.001). Using an ultra-high dose (86.4 Gy) IMRT for 478 localized prostate cancer patients, Cahlon et al. [7] reported 8% acute Grade 2 GI toxicity, which is almost similar to ours. There was no acute Grade 3 or higher GI toxicity noted. Grade 2 and 3 acute GU toxicity was seen in 22% and 0.6% patients respectively. There are several limitations to our series. First, this is a very small cohort of 40 patients. Secondly, it's our departmental practice / policy for the treatment of localized prostate cancer with IMRT, rather than a typical study. It's a retrospective analysis of prospectively evaluated and entered data on acute toxicity scores. Finally, we believe that the recent implementation of image-guided RT (IGRT) and adaptive RT (ART) will further enhance the safety and accuracy of IMRT because of the better correction of both interfraction positional variation and intrafraction prostate motion and achieve, therefore, additional decreases in acute and late toxicity. Conclusion Our results provide the first detailed assessment of acute toxicity in localized prostate cancer patients treated with definitive IMRT within the Indian sub-continent. In conclusion, the dose escalation to the prostate to a dose of 76 Gy (79.8 Gy to the isocenter, ICRU reference point) implemented through IMRT is safe, effective and very well tolerated by all of our patients with limited and acceptable acute GI and GU toxicity rates, thereby, establishing the feasibility of dose escalation with IMRT in the Indian scenario. This series paves way for future clinical trials directed towards further dose escalation in prostate cancer to improve biochemical control rates leading to overall improved outcome. We realize that a longer follow-up would be necessary for our series to corroborate and substantiate our data on acute toxicity to that of the late toxicity and also to evaluate biochemical response outcome. We are working towards assessing our two-year follow-up data. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10013t2.jpg] [cr10013t5b.jpg] [cr10013t5a.jpg] [cr10013t1.jpg] [cr10013t3.jpg] [cr10013t4.jpg] [cr10013t7.jpg] [cr10013t6.jpg] [cr10013t8.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}