 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
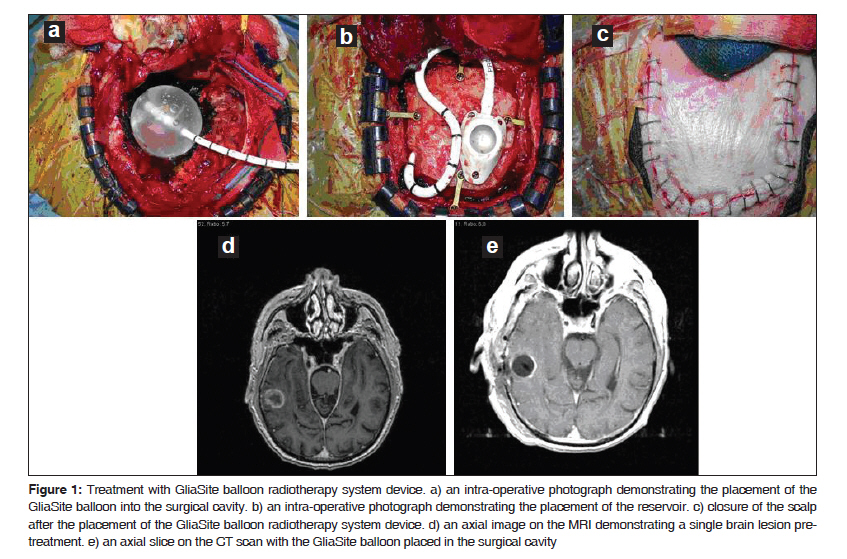
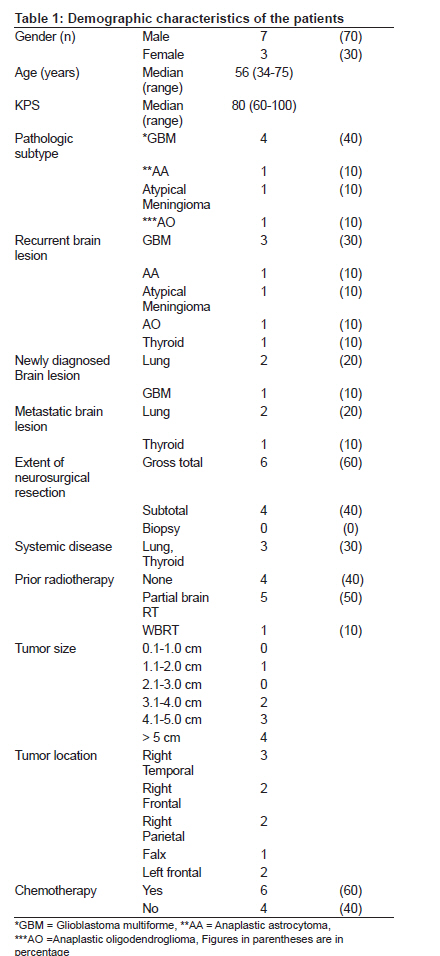
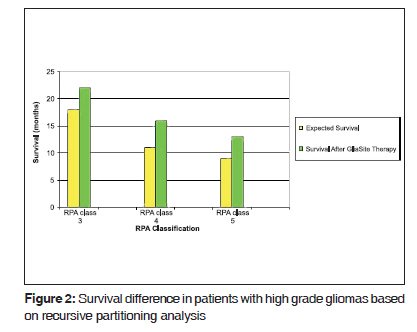
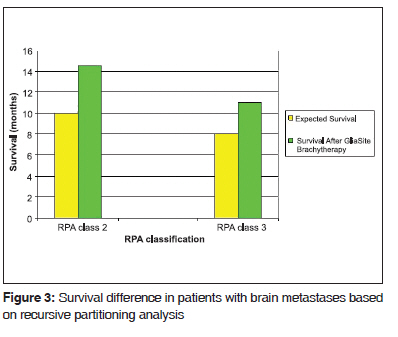
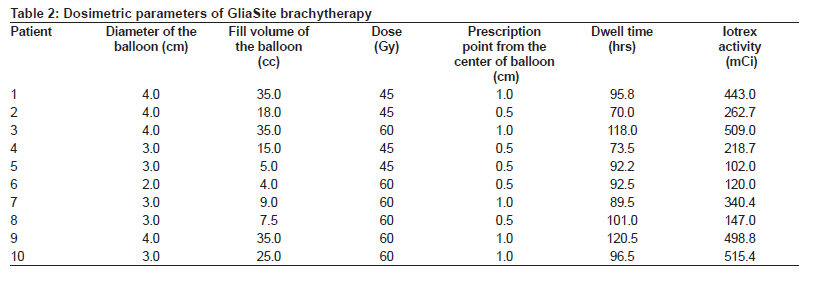
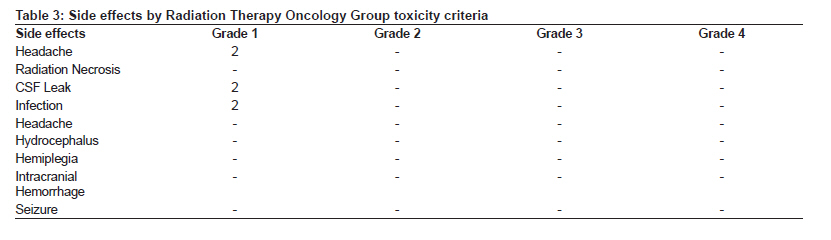
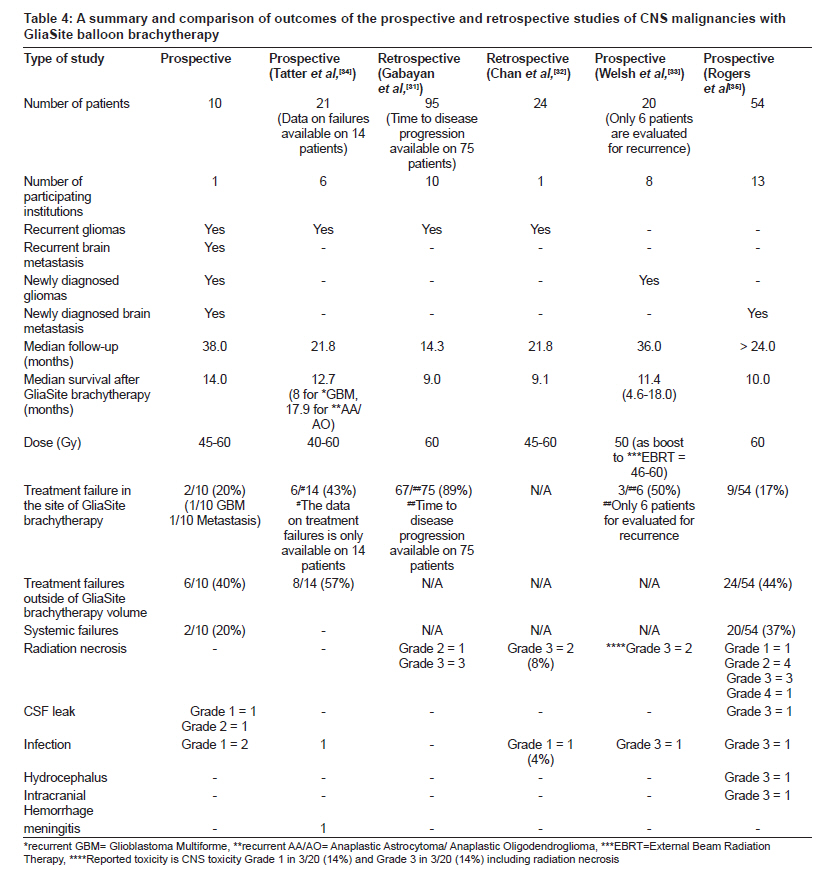
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 65-74 Brief Communication Feasibility and safety of GliaSite brachytherapy in treatment of CNS tumors following neurosurgical resection A. Gabriella Wernicke, David L. Sherr, Theodore H. Schwartz1 , Susan C. Pannullo1 , Philip E. Stieg1 , John A. Boockvar1 , Jana Ivanidze2 , Jennifer A. Moliterno3 , Bhupesh Parashar, Samuel Trichter, Albert M. Sabbas, Dattatreyudu Nori Radiation Oncology, Weil Cornell University School of Medicine, New York, Code Number: cr10014 DOI: 10.4103/0973-1482.63547 Abstract Purpose: To investigate feasibility and safety of GliaSite brachytherapy for treatment of central nervous system (CNS) tumors following neurosurgical resection. We report mature results of long-term follow-up, outcomes and toxicity. Materials and Methods: In the period from 2004 to 2007, 10 consecutive adult patients with recurrent, newly diagnosed, and metastatic brain malignancies underwent GliaSite brachytherapy following maximally safe neurosurgical resection. While 6/10 (60%) patients were treated for recurrence, having previously been treated with external beam radiotherapy (EBRT), 4/10 (40%) received radiotherapy (RT) for the first time. A median dose of 52.0 Gy (range, 45.0 - 60.0 Gy) was prescribed to 0.5 cm - 1.0 cm from the balloon surface. Radiation Therapy Oncology Group (RTOG) criteria were used to assess toxicities associated with this technique. Follow-up was assessed with MRI scans and was available on all enrolled patients. Results: Median follow-up was 38 months (range, 18 - 57 months). Mean size of GliaSite balloon was 3.4 cm (range, 2.0 - 4.0 cm). Median survival was 14.0 months for the entire cohort after the treatment. The 17.6 and 16.0 months average survival for newly diagnosed and recurrent high grade gliomas (HGG), respectively, translated into a three-month improvement in survival in patients with newly diagnosed HGG compared to historical controls (P = 0.033). There were no RTOG grades 3 or 4 acute or late toxicities. Follow-up magnetic resonance imaging (MRI) imaging did not identify radiation necrosis. Conclusions: Our data indicate that treatment with GliaSite brachytherapy is feasible, safe and renders acceptable local control, acute and long-term toxicities. We are embarking on testing larger numbers of patients with this treatment modality.Keywords: Brachytherapy, brain cancer, brain metastasis, central nervous system malignancies, glioblastoma multiforme, gliasite balloon, iotrex, radiation Introduction Advancement in improvement in local control of central nervous system (CNS) malignancies may enhance not only the quality of life but also the overall survival. A multi-modality approach to a patient with a newly diagnosed or a recurrent brain lesion typically involves a neurosurgical resection, radiotherapy (RT), and chemotherapy, depending on the histopathology of a tumor. The treatment of the gliomas is complicated by the infiltrative nature of the malignant process into the surrounding normal brain. As systemic therapies for cancers improve and the overall survivorship of a cancer patient increases, the incidence of brain metastases rises. Despite the advancement made in the fields of neurosurgery, neuro-oncology, medical oncology, and radiation oncology, local control for brain lesions continues to present a challenge to both the treating physicians and patients. Improved outcomes with the application of a multi-modality management of patients with malignant glioma have been reported in several series. The use of both external beam RT and chemotherapy has rendered an enhanced local control and survival in the newly diagnosed malignant gliomas. [1],[2] An absolute increase in the one-year survival rate from 40 to 46% was reported in the meta-analysis of randomized clinical trials which compared RT alone vs. RT with chemotherapy. [3] The biodegradable carmustine wafers (Gliadel) have been shown to increase survival by approximately 2 months with less toxicity than with systemic chemotherapy. [4] The use of Temozolomide increased median survival when added to RT to 15 months. [5] Various modalities are employed for recurrent gliomas, ranging from invasive techniques such as re-operation (with or without chemotherapy with local therapy Gliadel wafers or systemic use of Temozolomide) and brachytherapy (interstitial or intra-cavitary), to non-invasive techniques with three-dimensional (3-D) conformal external RT, intensity modulated radiotherapy (IMRT), stereotactic radiosurgery (SRS), or stereotactic radiotherapy (SRT). With regard to brain metastases, they outnumber primary neoplasm by at least 10 to 1, and they occur in 20 to 40% of cancer patients. [6] Because no national cancer registry documents brain metastases, the exact incidence is unknown, but it has been estimated that 98,000 to 170,000 new cases are diagnosed in the United States each year. [7] This number may be increasing because of the capacity of MRI to detect small metastases and because of prolonged survival resulting from improved systemic therapy. The most common primary cancers metastasizing to the brain are lung cancer (50%), breast cancer (15-20%), unknown primary cancer (10-15%), melanoma (10%), and colon cancer (5%). [8],[9] Prospective randomized trials have established that resection of a single brain metastasis, particularly in patients without systemic cancer with a good performance status, led to improved survival and prolonged functional independence. [10] Irradiation of the whole brain (WBRT) improved local control (from 10 to 46%) and distant brain tumor control (from 14 to 37%) but had no impact on survival or functional independence. [11] However, more data have emerged with respect to treating few brain lesions with aggressive local radiation as a good alternative to avoiding the side effects of WBRT. [12][13],[14] High grade gliomas tend to recur within 6-10 months after treatment. The patterns of recurrence and failure studies examining recurrence of glioblastoma multiforme (GBM) after primary therapy have demonstrated that majority of the patients experience recurrence immediately near the resection bed (within 2 cm) with virtually no metastases outside the CNS system. [15],[16],[17] Disease progression is followed shortly by death. Therefore, optimization of sterilization of the surgical margin may offer an advantage in local control and potentially survival. Established adjuvant RT, administered to the surgical bed with margin using external beam techniques, has been delivered with standard fractionation to a total dose of 60.0 Gy. Dose escalation beyond 60.0 Gy with external beam RT did not result in benefit of improved survival and was likely to result in injury to the normal brain tissue. [18],[19] A number of attempts have been reported to escalate the dose with interstitial brachytherapy. Several trials reported that radiation necrosis dampened the results of treating primary and recurrent GBM with high-dose rate (HDR) temporary 125 I seed implants which require a stereotactic frame placement and drilling of multiple holes in the skull for seed delivery. [20],[21],[22],[23],[24] Repeated operations for radio necrosis in generally occurred within 6months of the end of RT 26 to 64% of treated patients. [20],[24],[25],[26],[27],[28] Low-dose-rate (LDR) interstitial brachytherapy with permanent 125 I implants does not require a stereotactic frame or drilling of holes in the skull for seed placement and reduces the incidence of such complications as symptomatic radio necrosis. However, with both HDR and LDR 125 I seed placement in the surgical cavity can produce an inhomogeneous dose distribution which in turn may have led to radio necrosis in the over-dosed areas and recurrence in the under-dosed regions. Lack of improvement in survival in patients with recurrent GBM treated with HDR and LDR interstitial brachytherapy with 125 I implants may be explained by deficiencies in dose distribution. [29],[30] Intracavitary type of delivery with GliaSite brachytherapy is a form of localized radiation treatment that involves delivery of highly localized doses of radiation implanted in the resection cavity of the tumor while minimizing dose deposition to the surrounding tissues. Further, this method allows the delivery of radiation dose to areas most at risk of recurrence while addressing the limitations of interstitial brachytherapy. The intracavitary LDR device is a balloon catheter system (GliaSite) and an aqueous iodinated radiation source (Iotrex (sodium 3-( 125 I)-iodo-4-hydrobezenesulfonate) are designed to fill the tumor resection cavity and allow for the dose to be precisely defined and reproduced. While two retrospective and a few prospective studies have reported the safety and feasibility of the device and a modest survival, few studies follow-up on all patients and therefore do not report the patterns of treatment failure, rates of local or distant brain tumor control, and side effect profiles. [31],[32],[33],[34],[35] In this prospective study, we report not only on the feasibility and safety of the GliaSite system when used in patients with either newly diagnosed or recurrent brain cancers but also we provide long-term follow-up and mature results of rates of local or distant brain tumor control, and treatment side effects and on all enrolled subjects. Materials and Methods Between 2004 and 2007, 10 consecutive adult patients with recurrent, primary, and metastatic brain malignancies were offered participation in the institutional board review- approved prospective pilot study. All subjects provided informed consent prior to initiation of treatment. Eligibility criteria included age ≥ 18 years and potentially respectable tumors. The patients had to be medically cleared for a neurological resection, with an estimated life expectancy of ≥ 60 days. The exclusion criteria were the use of any other investigational agent, multifocality of disease, residual tumor exceeding 2 cm from the surface of the GliaSite balloon, lack of medical clearance to undergo surgical resection and a GliaSite balloon placement due to the medical co-morbidities. Six patients were treated for recurrence, having previously been treated with external beam radiotherapy (EBRT) (3 for glioblastoma multiforme (GBM), two for metastatic disease, and one for atypical astrocytoma (AA)). Four of the study participants received radiotherapy (RT) for the first time (two for metastasis, one for GBM, and one for anaplastic oligodendroglioma (AO)). The primary end point of this trial was feasibility of the successful performance of the device. It was assessed based on: a) ability to implant the GliaSite balloon into the surgical cavity, b) conform the device to the resection cavity, c) avoid migration of the balloon, and d) successful dose delivery. The secondary end point of this study was the safety of the device, which occurred at the times of implantation, delivery of brachytherapy, and finally explantation. GliaSite balloon was placed intra-operatively by the neurosurgeons, immediately following maximally safe neurosurgical resection [Figure - 1]. The size was selected so as to conform to the surgical cavity. The GliaSite system consists of an infusion port with self-sealing silicone septum at the proximal end for instillation of (Iotrex ® ) (sodium3-(125I)-iodo-4-hydorybenzenesulfonate). The shaft is an 18 cm length of bi-lumen, radiopaque silicone tubing with a malleable titanium element to assist in positioning the balloon. The dual configuration of a balloon at the distal end comes in diameters of 2, 3, and 4 cm with corresponding full volumes of 5, 15 and 35 cc. The inner balloon acts as a reservoir for the liquid I-125 source (Iotrex ® ). Iotrex ® solution is a sterile, non pyrogenic solution containing sodium 3-iodo-4-hydroxybenzenesulfonate. Radio-opaque markers denote the proximal and distal sides of the inner balloon. The outer balloon acts as a backup in the event that the integrity of the inner balloon is compromised. A safety lumen is incorporated into the catheter shaft to allow access to the outer balloon should there be a need. Positioning markers are provided on the catheter shaft at 1 cm intervals beginning at the proximal end of the balloon. A right-angle anchoring clip is used to secure the catheter where it exits the burr hole. After successful placement, a postoperative MRI was performed. From the postoperative MRI, the conformality of GliaSite balloon (filled with 75% sterile normal saline and 25% non-ionic contrast agent) to the surrounding brain tissue was assessed. Exact calculations were made to measure the maximum diameter, calculate its volume and compare it to the fill volume as per fluid chart. The amount of activity ordered was based on prescription dose, prescription depth and fill volume. Iotrex ® solution is delivered in 1.0 ml unit doses containing a minimum of 150 mCi. The 5 cc syringe with the Iotrex solution is placed within a syringe shield. Two to three weeks after the patient recovered from surgery, a combination of Iotrex ® and saline was injected into the catheter and filled the balloon allowing for size and placement verification of the balloon with an MRI scan. The radioactive Iotrex ® solution was administered in the patient's room by an attending radiation oncologist in the presence of a radiation oncology physicist and radiation safety personnel. All the patients were given a single room. The Iotrex ® dwelled for three to seven days, delivering the prescribed dose of radiation. At the end of this period, the Iotrex ® and saline was withdrawn and the balloon catheter was then removed during a brief surgical procedure. Twenty-four hours prior to, and continuing throughout brachytherapy, the patients received SSKI (Potassium Iodide) or equivalent to block the thyroid in case of balloon rupture. Even in the case of balloon ruptures, no organ was expected to receive any appreciable dose as the Iotrex ® is rapidly and completely excreted via the renal pathway and bladder. A commercial 3-D planning system was used for detailed analysis of dosimetry. The treatment dwell times are a function of prescription dose, prescription depth from the balloon surface, balloon fill volume and net afterloaded activity of the Iotrex ® solution. Based on the prescription dose and depth, generally 1 cm from the surface, as well as the balloon fill volume, an order is placed for the appropriate amount of Iotrex ® solution in mCi. The fill volume is assessed using postoperative MRI following the placement of the catheter to assess balloon conformality to the surgical cavity. The order is placed in terms of prefilled 5 cc syringes that greatly facilitate the subsequent handling of the solution. The volume of the Iotrex ® ranges from 1 to 4 cc with an approximate concentration of 150 mCi/cc. We base our orders on tables provided by the company of suggested activity specifically designed for Gliasite. These tables are organized in terms of prescription dose, depth and fill volume and are derived based on Monte Carlo calculations and subsequent experimental verification of the radiation around the balloon. As a rule, we order an additional 20 mCi of activity than what the tables suggest to account for any losses of the activity in the cap of the syringe which is removed to place the needle as well as the walls of the syringe itself. The net activity infused in the patient is based on two measurements before and after (residual activity) the injection into the balloon using Capintec, CRC 12, dose calibrator from nuclear medicine. Radiation Therapy Oncology Group (RTOG) criteria were used to assess acute and long-term toxicities associated with this technique. All patients underwent serial MRI scans every two months (or sooner if symptomatic) for tumor recurrence or progression. Time to failure locally or distantly in the brain was calculated from the time GliaSite brachytherapy ended to the first detectable recurrence by the MRI. Systemic recurrence (outside of brain) was assessed with Positron emission tomography - computed tomography (PET-CT) or CT scans. Treatment failures, survival, and toxicity profile related to therapy were available and recorded for all 10 patients. Descriptive statistics were employed for characterization of this cohort of patients. Each patient was stratified into a respective recursive partitioning analysis (RPA) class. [36] The medial survival of the subjects on our study was compared to the historical controls of 14.0 and 13.9 months for newly diagnosed and recurrent high grade gliomas. [4],[5] Results A total of 10 patients with recurrent, primary, and metastatic brain malignancies underwent the neurologically safe maximal tumor resection followed by brachytherapy with GliaSite balloon radiotherapy system. [Table - 1] summarizes the patients' demographics and tumor characteristics. The median patient age of the cohort was 56 years (range, 34 -75 years). The mean Karnofsky performance status (KPS) was 80 (range, 60-100), with the majority of patients having a KPS of ≥ 70. Gross total neurologically safe resection was accomplished in 6 (60%) of the patients, while subtotal resection took place in 4 (40%) cases. Of the 10 participants in the study, two patients were not classified by RPA, [36] as one of them had an AO and the second one had an atypical meningioma. Of the RPA classifiable eight patients, five had a high grade glioma and three had single brain metastasis. RPA class distribution for a high grade glioma, including AA, was as follows: class 3, n = 1/5 (20%); class 4, n = 1/5 (20%); class 5, n = 3/5 (60%), and no patient belonged to a class 6. RPA classes for metastasis had the following distribution: class 1, n = 0 (0%); class 2, n = 2/3 (67%); and class 3, n = 1/3 (33%). The primary tumor site was predominantly supratentorial. For four patients (40%) treatment with GliaSIte brachytherapy was the first treatment with radiotherapy. The other six study subjects had received EBRT to either partial brain (50%) or whole brain (10%) [Table - 1]. The prior doses of RT to partial brain and whole brain were 60 Gy and 37.5 Gy, respectively. Sixty per cent of the patients were treated with systemic chemotherapy and four (40%) were not. The median survival was 14.0 months for the entire cohort after the treatment with the GliaSite device. Our study subjects experienced 17.6 months and 16.0 months average medial survival time (MST) for newly diagnosed and recurrent high grade gliomas, respectively. The additional three-month improvement in MST in patients with newly diagnosed high grade gliomas represented a statistically significant increase compared to historical controls (P = 0.033), while a 2.1 month increase in MST in the subjects with recurrent disease had a trend toward statistical significance (data not shown). We compared survival based on the RPA classification of historical controls in the literature and our cohort of patients. [Figure - 2] demonstrates an increase is survival for the patients in this pilot with recurrent high grade gliomas by 4.0, 5.0, and 4.0 months for the respective RPA classes 3, 4, and 5, respectively. Similarly, [Figure - 3] displays the improved survival in our patients with brain metastases as compared with historical controls by 4.5 and 3.0 months for their respective RPA classes 2 and 3. MST was 20.0 months for newly diagnosed patients with AA/AO and 17.0 months for recurrent AA. After a median follow-up of 38 months (range, 18 - 57 months), all but one patient had died. The remaining living study subject is alive at 19 months after treatment and is evaluated in the final analysis as if he died at the time of the analysis. Of our cohort, 6/10 (60%) patients sustained a recurrence (20% local and 40% distant). The median time to recurrence after treatment with GliaSite was 8.0 months, and median time to death after recurrence was 7.5 months. To date, 1/10 (10%) of patients remain alive. The dosimetric brachytherapy parameters of GliaSite treatment are outline in [Table - 2]. There were no balloon ruptures. The mean size of GliaSite balloon was 3.4 cm (range, 2.0 - 4.0 cm), with 1/10 (10%) patients treated with a 2.0 cm, 5/10 (50%) with 3.0 cm, and 4/10 (40%) with 4.0 cm balloon diameter. The mean volume of filling was 19.0 cc (range, 4.0 - 35.0 cc). The median dwell time was 94.3 hours (range, 68.0 - 120.5 hours), following which the balloon was explanted in all patients. A median dose delivered was 52.0 Gy (range, 45.0 - 60.0 Gy), and it was prescribed to 0.5cm - 1.0 cm from the balloon surface. Patients with a subtotal resection were treated with a higher dose and to a greater depth so as to ensure that the residual gross tumor received the full prescribed dose. The typical dose for such situations was 60.0 Gy prescribed and delivered to the depth of 1.0 cm. The median activity of Iotrex ® was 301.6 mCi (range, 95.0 - 515.4 mCi). In all patients, GliaSite balloon implantation and its removal were successful. [Table - 3] summarizes the side effects of GliaSite brachytherapy as graded by the RTOG central nervous system morbidity criteria. There were no serious adverse GliaSite balloon-related effects and no grades 3 or 4 acute or late toxicities. Acute headache (grade 1) was reported in 2/10 (20%) of patients which resolved after increase steroid administration. Of the subjects enrolled, 2/10 (20%) experienced cerebral spinal fluid (CSF) leak at the time of surgery. Presence of CSF leak appeared to be the only risk factor leading to an acute infection in 2/10 (20%) patients. The infection occurred in patients with prior previous treatments, and both patients were treated successfully with antibiotics. No patients developed symptomatic radiation necrosis. Follow-up MRI imaging did not identify any evidence of radiation necrosis. Discussion Localized CNS malignancies continue to remain a challenging therapeutic and clinical task despite advances in neurosurgery, novel chemotherapeutic agents, and radiation delivery techniques such as SRS, SRT, or IMRT. The predominant number of patients develops recurrent disease within several months of diagnosis and therapy. The vast majority of recurrences occur locally within the post-operative surgical bed and in the region targeted with EBRT. Several studies reported that dose escalation with RT has been reported to improve survival in patients with malignant glioma. [1],[2],[37] However, increase in the dose beyond 60.0 Gy with the external beam techniques has not translated to an improved survival likely because of injury to the normal brain. Interstitial brachytherapy has been used in an attempt to increase radiation dose delivered to tumor cells while limiting doses received by the healthy brain tissue. The risk of developing radiation necrosis is likely a result of suboptimal dosimetry (due to the challenges of producing homogeneous dose distributions with multiple discrete seed sources around complex 3-D cavities) prevents this methodology from a wide application. [22],[26],[27],[28],[29],[32],[38],[39],[40] An attractive alternative to WBRT after a resection of a single brain metastasis can be rendered with brachytherapy. Such an approach targets the most frequent site of tumor recurrence, the resection cavity, while sparing unaffected brain tissue from the toxicity of WBRT which can worsen quality of life and cognitive function. [41] In contrast to malignant gliomas, the data on brachytherapy use in the setting of a brain metastasis are scarce. In one of the largest series reported to date, iodine-125 seed brachytherapy alone as applied for a newly diagnosed single brain metastasis resulted in a 17- month median survival. [42] Other studies on a recurrent or newly diagnosed metastasis report a range of survival, from six to 26 months. [43],[44],[45],[46] In 2001, the Food and Drug Administration approved the GliaSite radiotherapy system as a device for the treatment of resected malignant brain tumors. It offers a potential advantage over the conventional interstitial brachytherapy by means of delivering a more conformal, uniform and relatively homogeneous dose distribution, avoiding the "hot" and "cold" spots of over- and under-dosing of seed or strand brachytherapy approaches. [25],[47] Furthermore, the balloon conforms to the surgical cavity, and the dosimetry is precise and easily reproduced. This treatment method eliminates the need for stereotactic head frame, multiple scalp incisions and bur holes. Thus, the device is placed at the time of resection and allows delivery of high radiation dose to the areas most at risk for local recurrence while limiting the risk of radio necrosis by using a single radiation delivery vehicle that produces a homogeneous dose distribution. It has been noted that continuous LDR radiation in laboratory models appears better suited for enhancing the therapeutic ratio between normal and abnormal tissue. [48],[49],[50] Additionally, there is a hypothesis that LDR radiation may offer potential advantages in treating hypoxic cells in a surgical cavity. Our prospective study indicates that implantation, dose escalation with GliaSite balloon brachytherapy, and explantation procedures are feasible, safe and well-tolerated by all patients. The encouraging survival and local control results indicate that the approach with the GliaSite device may provide benefit to patients with localized CNS malignancies. As assessed by the follow-up MRI scans, treatment failures in two of 10 patients occurred within the treatment volume which translates into a local control of 80%. This fact confirms that some malignant tumors are resistant to the doses of radiotherapy administered in this study. Furthermore, the fact that majority of the treatment failures took place outside the GliaSite brachytherapy volume points to a therapeutic rationale for intracavitary brachytherapy. Expected MST for newly diagnosed high grade gliomas from a randomized study is 14.6 months [5] and for recurrent gliomas treated with Gliadel wafers is 13.9 months. [4] In our trial, this translated to 17.6 months and 16.0 months average MST, respectively. The additional three-month improvement in MST, observed in the patients with newly diagnosed high grade glioma, was corroborated as a statistically significant increase in the prior report by Welsh et al. [34] Similarly, a 2.1-month improvement in the MST in our cohort of recurrent gliomas as compared to the historic control showed a trend to significance. [4] When separated by RPA classification, our patients sustained superior survival than the reported literature [Figure - 2]. Historical controls of delivering radiotherapy to the whole brain (WBRT) following neurosurgical resection compare favorably with our study with respect to the MST in brain metastases. [9],[10],[11] We further examined the survival of our cohort with respect to the RPA classes and the addition of stereotactic radiosurgery after WBRT as reported in RTOG 9508. [51] An average MST in this report is 14.0 months. Similar to the high grade gliomas, the patients with brain metastases treated with GliaSite brachytherapy in our trial sustained a prolonged survival when examined based on the RPA classification [Figure - 2] and [Figure - 3]. As reported previously by RTOG trials, our data confirmed that systemic disease such presence of extra cranial metastases negatively impacted on patients' survival. [52] Nevertheless, we refrain from making any conclusions, other than to document this observation, regarding statistical significance of these findings due to the small number of patients. The rate of infection was within the expected range for this population, in which the patients who experienced infection had previously undergone numerous treatments, including surgical manipulation. The lack of radiation necrosis in this study cohort suggests that patients may tolerate this regimen better than the one with interstitial seed brachytherapy. None of our patients required surgical intervention to address radiation necrosis. This offers a possibility of further dose escalation with the potential to improve the efficacy of this treatment while avoiding the morbidity associated with high rates of radiation necrosis. The rate of the acute and long-term toxicities was acceptable. [Table - 4] summarizes the results of our study, compares and contrasts them with the data from previous prospective and retrospective single or multi-institutional reports. Of the five largest experiences in the literature listed, three were conducted in the setting of recurrent gliomas (two in a prospective and one in a retrospective manner, respectively). [31],[32],[34] One prospective study used GliaSite balloon brachytherapy as a boost for EBRT for the newly diagnosed GBM. [33] Additionally, this treatment approach was examined in a prospective manner for newly diagnosed single brain metastasis. [35] The doses prescribed in our study were similar to the ones used in other reports. This report gives a full account of 10/10 (100%) patients treated with the GliaSite device with respect to the local, distant and systemic treatment failures and provide the longest follow-up, as well as compares and contrasts the outcomes to the published literature [Table - 4]. While our trial was comprised of treating various histopathological tumor types, whether newly diagnosed or recurrent, the break down of survival by histological type, though slightly superior, compares to the published data. We report a 20% local failure, defined as a treatment failure in the volume treated with GliaSite balloon brachytherapy as detected on the follow-up MRIs. Tatter et al. reports a 43% failure rate but comments despite 21 patients accrued and treated on this prospective trial, the data on treatment failures are only available in 14/21 (67%) patients. [34] Of 20 participants in another prospective study, Welsh et al. publish that only 6/20 (30%) were evaluated for recurrence with local failure rate of 50%. [33] The study of GliaSite application for newly diagnosed single metastasis reports similar rates of local and elsewhere in-brain progression of disease to our report: 17% vs. 20%; 44% vs. 40%, respectively.[35] Our RTOG-based toxicity profile is quite favorably compared to the prior reports and is devoid of any high grade toxicity, including radiation necrosis, hydrocephalus, intracranial hemorrhage, or meningitis. Conclusions Though we report long-term follow-up, data on treatment failures and toxicity in all patients in this prospective study, we have to acknowledge some of the limitations of our study. The number of patients for this pilot is small, and the patient population is heterogeneous with respect to the histopathology and either newly diagnosed or recurrent setting of the disease. However, the objective of this preliminary pilot study was to assess feasibility and safety of the GliaSite balloon brachytherapy device and not to evaluate survival. This study demonstrates that GliaSite brachytherapy can be a valuable tool for dose escalation in patients with localized CNS malignancy. Based on our encouraging results, we are embarking on testing larger numbers of patients with this treatment modality. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10014t3.jpg] [cr10014f3.jpg] [cr10014t2.jpg] [cr10014t1.jpg] [cr10014f2.jpg] [cr10014t4.jpg] [cr10014f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}