 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
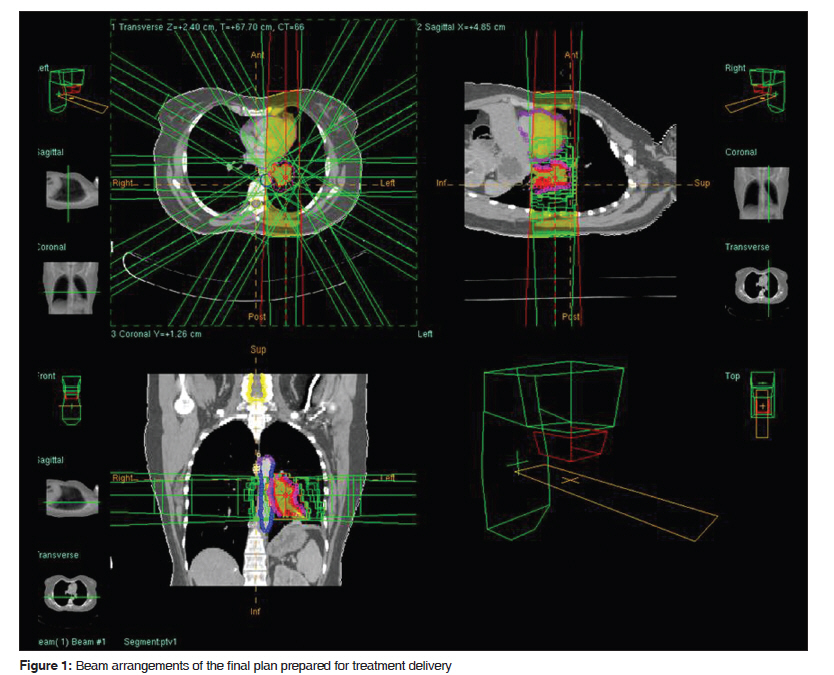
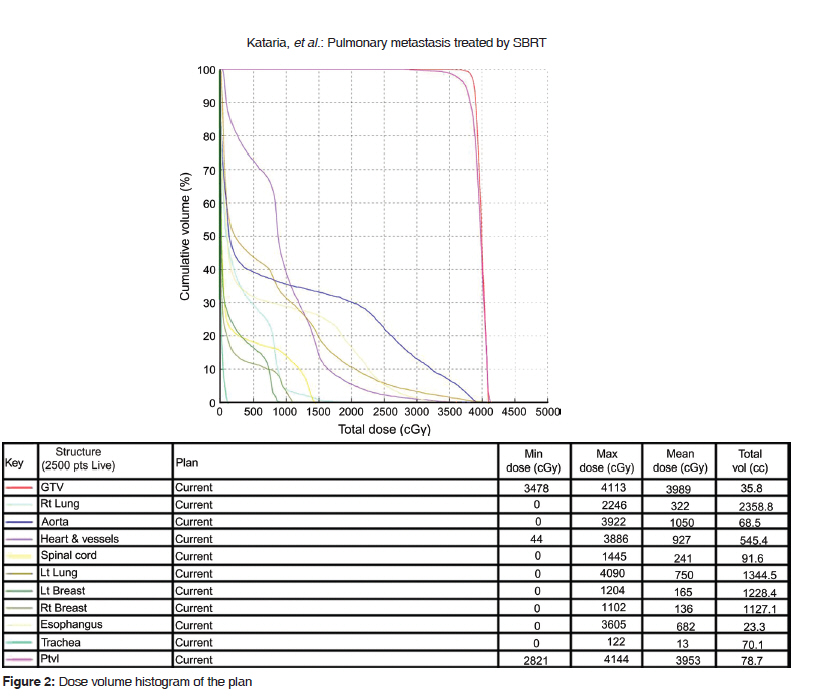
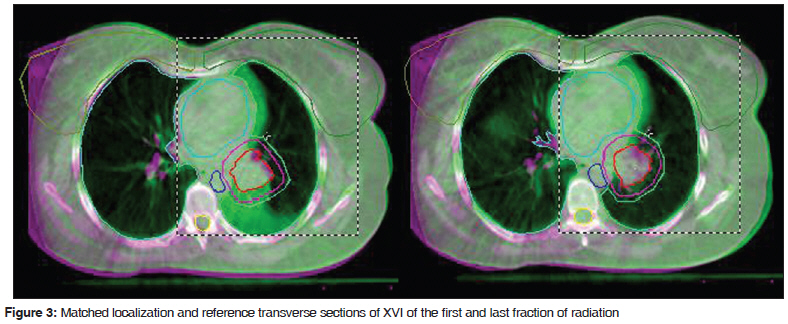
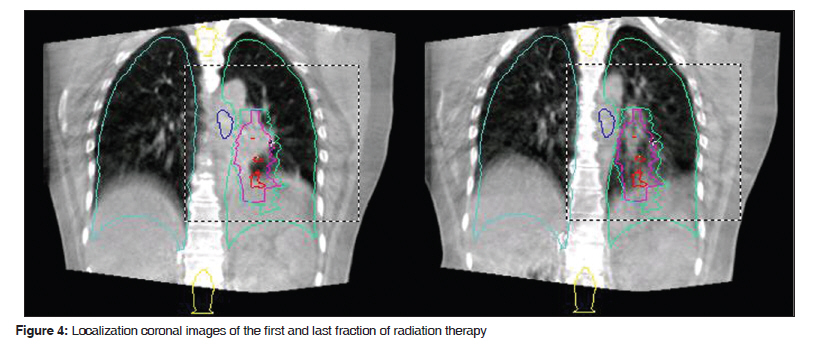
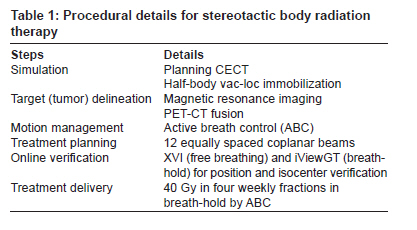
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 75-79 Case Report Pulmonary metastasis from renal synovial sarcoma treated by stereotactic body radiotherapy: A case report and review of the literature Tejinder Kataria, Nandigam Janardhan, Ashu Abhishek, Gautam K. Sharan, Swarupa Mitra Department of Radiation Oncology, Artemis Health Institute, Gurgaon, Haryana, India Code Number: cr10015 DOI: 10.4103/0973-1482.63551 Abstract Primary synovial sarcoma of kidney is an uncommon neoplasm, metastasizing most commonly to lung. Surgery and/or palliative chemotherapy for pulmonary metastases is commonly used to improve tumor control and survival. Stereotactic body radiotherapy (SBRT) is a relatively new approach to treat pulmonary metastasis, encouraged by the results of cranial and spinal stereotactic radiosurgery. The local control and toxicity profile of patients with pulmonary metastasis treated with SBRT are comparable to pulmonary metastatectomy. Furthermore, with advancement of imaging techniques, immobilization techniques, tumor-tracking techniques, and treatment planning and delivery system, SBRT can now be alternatively employed for the treatment of pulmonary metastasis as a comparable substitute to surgical resection.Keywords: Pulmonary metastasis, renal synovial sarcoma, stereotactic body radiotherapy Introduction Primary sarcomas of kidney are rare tumors with a reported incidence of 1-3% of all renal malignancies. The pattern of presentation is similar to renal cell carcinoma, including aggressive local spread with distant metastasis to lung and liver in their natural history. [1] Metastatectomy and palliative chemotherapy have traditionally been used to improve control and survival. However, stereotactic body radiotherapy (SBRT) has recently been shown to be of comparable efficacy. We, hereby, present a case report of solitary pulmonary metastasis from renal sarcoma successfully treated by SBRT. Case Report A 52-year-old female, with a known case of right renal sarcoma, presented with PET-CT (3.2 x 3.6cm, SUV max. 5.4) and cytological diagnosis (malignant round cell tumor) of a left hilar mass. She was diagnosed in August 2003 following a right radical nephrectomy with vena cava thrombectomy for a symptomatic renal mass with the thrombus extending into the vena cava. Adjuvant chemotherapy was administered for eight cycles. She remained disease free till February 2007, when she was diagnosed with a left lower lobe solitary pulmonary nodule. Metastatectomy of the 2 x 1.5cm lesion revealed molecular evidence of synovial sarcoma (SYT-SSX2 fusion). She was kept on a close follow-up and presented to the clinic in August with mild hemoptysis for which she was investigated and diagnosed with left hilar recurrence. She was advised left pneumenectomy by her thoracic surgeon. She presented to us in September with a history of hemoptysis and breathlessness at rest. In view of solitary metastasis around left hila, preserved pulmonary functions, and a long disease-free interval, she was considered for high-dose-per-fraction SBRT. She was trained for active breath control (Active Breathing Coordinator TM , Elekta, UK) and a threshold inspiratory volume of 1.1 l and breath holding time of 15 s were registered. She underwent contrast-enhanced computed tomography (Gemini GXL PET/CT Imaging System - Philips Medical Systems Inc. USA) using half-body vac-loc immobilization and adequate hydration with N-acetyl cysteine (600-mg tablets twice a day for 2 days, followed by 1000mg i/v in 500ml normal saline over 3 h, to prevent contrast-induced nephropathy, in view of her postnephrectomy status). Images were acquired in both free-breathing and breath-hold positions, and the cranial displacement of central fiducial by 7mm on breath holding was noted. The planning target volume (PTV) was constructed from the gross tumor volume (GTV) as defined by the left hilar mass on planning CT, by adding 5mm radial and 10mm craniocaudal margins. A radiotherapy plan was generated for 40 Gy in 4 fractions (equivalent conventional dose being 74 Gy/37 fractions), delivering 10 Gy per fraction per week in a breath-holding position, with 12 equally spaced coplanar beams on PrecisePLAN TM (Elekta, UK) [Figure - 1] and [Figure - 2]. The patient was positioned for treatment as per the free-breathing images (planning CECT), and X-ray volume images (XVI) were acquired on the Elekta Synergy accelerator (360 rotation, acquisition time 3 min, dose delivered 8 mGy). Images thus obtained were matched with reference CT images and couch repositioning was done, if required, based on the correction obtained. Field matching and isocenter confirmation were done using orthogonal View Gun to Target (iViewGT TM , Elekta, UK) images in a breath-hold position. Treatment was delivered after set-up confirmation and couch adjustment, with verbal instructions to hold breath. Time taken for each fraction was approximately 45 min. Except for mild cough in the third week, she remained asymptomatic. XVI during the delivery of the last fraction showed resolution of the mass with appearance of cavitations and irregularity in previous well-defined opaque borders [Figure - 3] and [Figure - 4] [Table - 1]. Discussion Stereotaxy refers to a three-dimensional coordinate system to guide a procedure. The technique of stereotactic radiotherapy was pioneered by Lars Leksell at Karolinska Hospital in Stockholm. The transition from biologically potent high-dose-per-fraction cranial stereotactic radiosurgery to extracranial sites has been made possible by the advancement of technology in immobilization, tumor tracking, image guidance, and radiation planning and delivery. SBRT is defined as the management and delivery of image-guided high-dose radiation therapy with tumor ablative intent within a course of treatment up to five fractions. [2] Primarily used for liver, lung, and spine lesions, SBRT has also been investigated for prostate cancer, renal cell carcinoma, and pancreatic cancer, among other sites. Lax and Blomgren have reported the anatomic distribution of 1965 tumors treated with SBRT. Intrathoracic tumors constituted largest number (55%) followed by liver (24.6%), pancreas (7.6%), and abdominal (6%) tumors. [3] Synovial sarcoma is an uncommon tumor, and constitutes 6-10% of soft tissue sarcomas. Primary synovial sarcoma of the kidney is rare, and leiomyosarcoma is the most common type of renal sarcomas, followed by rhabdomyosarcoma, histiosarcoma, chondrosarcoma, and osteosarcoma. Differential diagnoses include mesoblastic nephroma, adult neuroectodermal tumor (PNET), adult Wilm's tumor, and fibrosarcoma. [4] Theoretically, SBRT has the potential to cure oligometastasis of lung and to improve quality of life in multiple metastases. There is a high rate of 3-5 years of survival following aggressive local therapy (surgical resection, radiofrequency ablation, cryotherapy, etc.) in pulmonary metastasis, and SBRT can be considered as a noninvasive substitute, providing a comparable efficacy and same or lesser toxicity. In contrast to conventional radiotherapy, margins around the target volume are small in order to decrease normal tissue toxicity. The ability to target the tumor precisely, taking into account the interfractional set-up errors (relative independence of lung from bony landmarks) and intrafractional variation (due mainly to respiration) along with a decrease in the irradiated lung volume, promises dose escalation, and therefore, better tumor control. Radiobiologically, fractionation is employed to allow for a normal tissue repair of a sublethal damage to the cell. The observations of dose dependency and fraction size on tumor control have been well documented. If the irradiated volume is restricted to tumors with a very close margin, a sublethal damage to normal tissues is not a concern and complete tumor control is intended. Schetfer et al. reported early results on dose escalation and toxicity in their phase I SBRT trial for lung metastasis. First cohort of patients received 48 Gy in three fractions and subsequent cohorts got a dose escalation of preselected maximum 60 Gy in three fractions. The percentage of a normal lung receiving more than 15 Gy (V 15 ) was less than 35%. Acute grade 3 lung or esophageal toxicity or any other grade 4 toxicity was defined as dose-limiting toxicity (DLT). None of their patients experienced DLT and no significant change in pulmonary function tests was noted. [5] Similar results have been reported by Okunieff et al. in their analyses of 50 patients. Sixty-two percent of patients received 50 Gy in 10 fractions. Local control of treated lesions was 83% in a mean follow-up of 18.7 months with 2% grade 3 toxicity. Local control of lung metastases treated by SBRT is impressive and comparable to other modalities of treatment. Song and Blomgren have reviewed the literature and reported 78-100% local control with a median follow-up of 8-20 months. [6] Acknowledgments The authors wish to acknowledge the compassion and dedication of Mr. Joseph Yesudoss, Mr. Standley Jayaraman, and Mr. Rakesh Nair, the radiotherapy technologists in assisting the set-up and delivery of this complex treatment. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10015f3.jpg] [cr10015t1.jpg] [cr10015f4.jpg] [cr10015f2.jpg] [cr10015f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}