 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
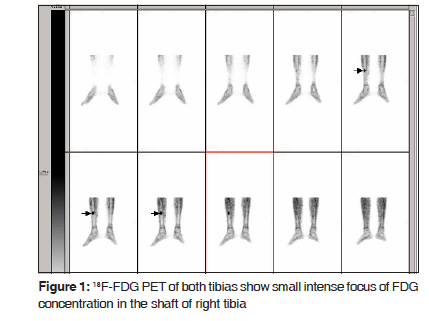
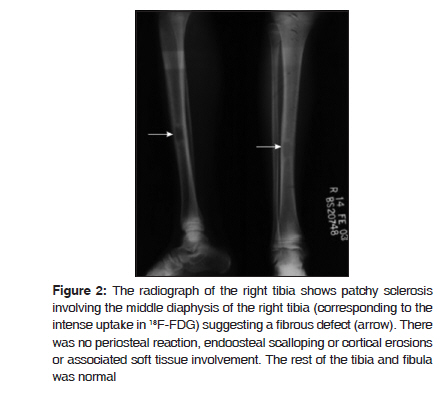
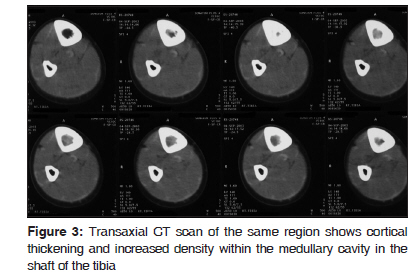
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 92-94 Case Report 18 F-FDG avid lesion due to coexistent fibrous dysplasia in a child of embryonal rhabdomyosarcoma: Source of false positive FDG-PET Sandip Basu, N. S. Baghel, Ajay Puri 1 , Tanuja Shet 2 , N. H. Merchant 3 Radiation Medicine Centre (BARC), Departments of 1 Surgical Oncology, 2 Pathology and 3 Radiology, Tata Memorial Hospital Annexe, Jerbai Wadia Road, Parel, Mumbai-400 012, India Code Number: cr10020 DOI: 10.4103/0973-1482.63564 Abstract With increasing use of 18 F-fluorodeoxyglucose (FDG)-positron emission tomography (PET) in the current oncological practice, there is a growing body of evidence of false positive scans due to various benign conditions. In this communication we present intensely avid 18 F-FDG uptake in fibrous dysplasia of right tibia in a 12-year-old child suffering from embryonal rhabdomyosarcoma (ERMS) that could have been easily mistaken to be a metastatic focus if not carefully correlated. The patient was a case of ERMS (presenting with left cervical mass with intrathoracic extension) who was treated successfully with chemotherapy and was referred for FDG-PET to evaluate the disease status. His whole body survey was unremarkable except for an intensely avid FDG uptake (SUV max 8.5) in shaft of right tibia. The scan was extended up to foot in view of the fact that a prior bone scan had shown a focal uptake in the similar location. Efforts were undertaken to elucidate the exact etiopathology of the aforementioned 18 F-FDG uptake because the rest of the whole body survey was unremarkable. A plain radiograph (both anteroposterior and lateral views) of the right tibia showed patchy sclerosis involving the middle diaphysis of the right tibia suggesting a fibrous defect. The computed tomography (CT) scan of the same region showed cortical thickening and increased density within the medullary cavity in the shaft of the tibia. A histopathological diagnosis was sought for and the lesion was subsequently proven to be fibrous dysplasia by histopathology of the bone piece obtained from the right tibial lesion by J needle biopsy. The present case is a useful addition to the current body of literature of false positive 18 F-FDG-PET study due to a benign skeletal pathology and underscores the importance of high index of suspicion and careful clinicoradiopathologic correlation, whenever one comes across such an unusual PET finding.Keywords: FDG PET, fibrous dysplasia, embryonal rhabdomyosarcoma, false positive Introduction FDG-PET is considered to be relatively specific compared to skeletal scintigraphy in the detection of skeletal metastases because it detects the presence of tumor directly by metabolic activity. The latter, on the other hand, indirectly shows tumor involvement to be mainly dependent on local osteoblastic reaction. However, potentially misleading falsely elevated 18 F-FDG uptake can arise from various anatomical variants, physiological processes and benign pathologies unrelated to the primary disease processes and with its increasing use in current practice, these are increasingly recognized. There have been attempts to characterize bone lesions as benign or malignant, based on qualitative as well as quantitative 18F-FDG PET studies, but this issue still is an open question. [1],[2],[3],[4] There is a relative paucity of literature regarding the FDG uptake pattern in benign bone tumors. Case Report A 12-year-old male case of ERMS (presenting with left cervical mass with intrathoracic extension) was treated successfully with chemotherapy and referred for 18 F-FDG PET for a whole body survey to evaluate the disease status. His whole body survey was unremarkable except for an intensely avid FDG uptake in shaft of right tibia [Figure - 1]. That the rest of the whole body survey was unremarkable was the reason for strenuous efforts undertaken to elucidate the abovementioned uptake. A plain radiograph (both anteroposterior and lateral views) of the right tibia showed patchy sclerosis involving the middle diaphysis of the right tibia suggesting a fibrous defect [Figure - 2]. The CT scan of the same region [Figure - 3] showed cortical thickening and increased density within the medullary cavity in the shaft of the tibia. A histopathological diagnosis was sought for and the lesion was subsequently confirmed as fibrous dysplasia by histopathology of the bone piece obtained by J needle biopsy from the right tibial lesion. Discussion FDG hyper metabolism in benign pathologies is often a source of a false positive scan and may be misinterpreted as metastatic lesion, if not carefully correlated. This is particularly important in the setting of malignancy, as in this case. With the given intensity of the uptake in the present case, the lesion could have been easily mistaken as a metastatic focus. The present uptake pattern is a useful addition to the current body of literature of false positive 18 F-FDG- PET scans due to a benign skeletal pathology. The 18 F-FDG uptake is probably related to the hyper metabolism due to high bone turnover in fibrous dysplasia. Till date, there has been only one report of FDG-PET in fibrous dysplasia. Our case is in sharp contrast to what has been reported by Toba et al. [5] They reported a case of fibrous dysplasia in craniofacial bone showing acceleration of bone mineral turnover without elevated glucose utilization evidenced by bone scan and 18 F-FDG-PET. [5] Fibrous dysplasia is a benign disorder of bone-forming mesenchyme, comprising around 10% of all benign bone tumors; [6] 70-80% of these are monostotic and 20-30% polyostotic. [6] The ribs, femur, tibia, calvarium, bones, spine, pelvis, and shoulder girdle are the frequently involved sites. [6] It is caused by an activating somatic mutation in the alpha subunit of the Gs protein, resulting in abnormal osteoblastic differentiation and increased bone turnover. [6] When polyostotic disease is associated with hyper pigmented cafι-au-lait macules and precocious puberty or other endocrinopathies, the McCune-Albright syndrome is diagnosed. Histopathologically, fibrous dysplasia is characterized by immature, relatively undifferentiated fibro-osseous connective tissue that fails to produce normal amounts of collagen within affected bones. On microscopy, it demonstrates a fibrous/collagenous matrix with randomly oriented bone trabeculae that are formed by osseous metaplasia of spindled stromal cells. In a conventional three phase bone scan it shows hyperemia, increased blood pool and intense tracer uptake in the delayed cortical phase. [7] This is related to the high bone turnover associated with the immature woven bone, a characteristic feature of this disorder. This also probably results in glucose hyper metabolism, resulting in high FDG uptake in a PET scan. Awareness of this situation cannot be overemphasized nor can be the value of careful correlation of an unusual finding in a PET scan. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10020f2.jpg] [cr10020f1.jpg] [cr10020f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}