 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
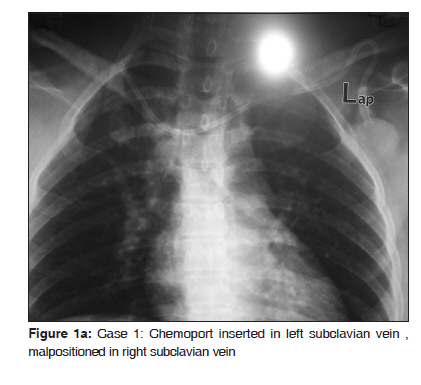
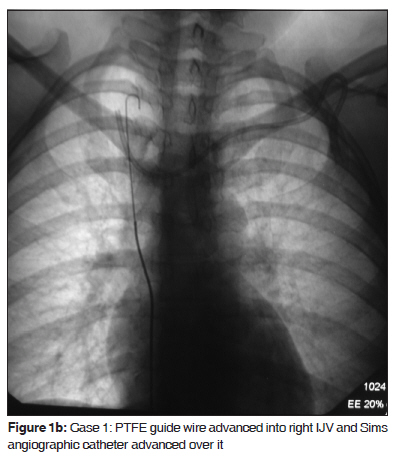
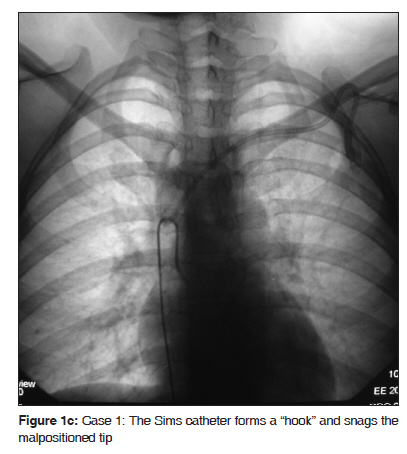
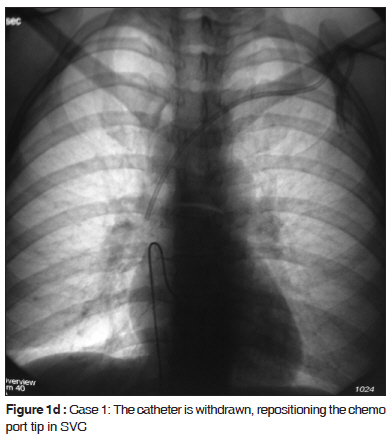
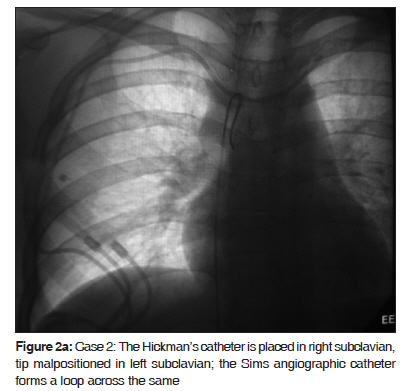
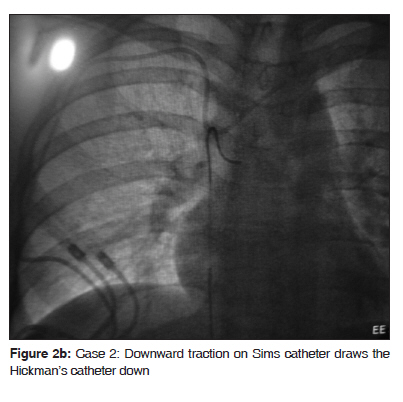
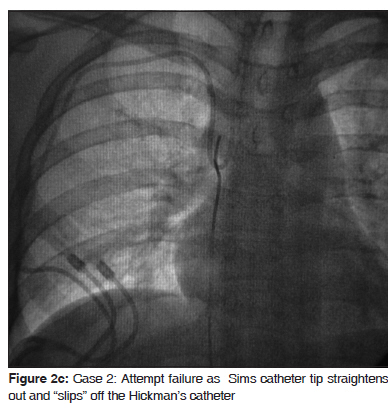
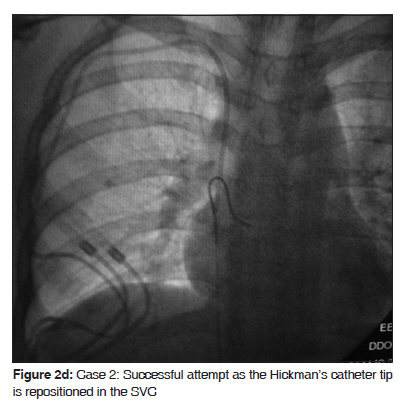
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 102-105 Case Report Percutaneous transfemoral repositioning of malpositioned central venous access device: A report of two cases Ashutosh Chauhan, Kamal Pathak1 , Manomoy Ganguly Departments of Surgical Oncology and 1 Interventional Radiology, Army Hospital (R &R), Delhi, India Code Number: cr10024 DOI: 10.4103/0973-1482.63554 Abstract Placement of long term central venous access devices (CVAD) such as chemo ports and Hickman's catheters are associated with a definite risk of catheter tip malpositioning. As such, malpositioning runs a risk of venous thrombosis and related complications; it is imperative to reposition the catheter. Percutaneous transfemoral venous approach has been described as a minimally invasive and safe method for the repositioning. We present two cases in which the CVAD implanted in one subclavian vein got malpositioned in contra lateral subclavian vein. A percutaneous transfemoral venous approach utilizing 5 Fr angiographic catheter was successful in repositioning of the catheters in both cases.Keywords: Chemo port, Hickman's catheter, malposition, repositioning Introduction Long term Central Venous Access Devices (CVAD) are frequently utilized in oncological practice, most commonly for chemotherapy and long term parenteral nutrition. CVAD insertion can be done "blind" using the Seldinger technique or under radiological guidance, either by ultrasound or fluoroscopy. [1] Malpositioning of the same is a known complication with reported incidence in an extremely wide range from less than 1% to more than 60%. [2] Unfortunately, improper catheter tip position is associated with a high rate of complications. [3] Various methods of repositioning have been described in the literature, which includes direct manipulation by guide wires or tip-deflecting wires by manipulation via transfemoral venous approach and by injection of contrast or saline. [4] We present two cases in which CVAD catheter tips were malpositioned into contra lateral subclavian vein when the device was inserted in one subclavian vein, and its subsequent repositioning into SVC by a fluoroscopic guided, transfemoral venous approach utilizing 5-Fr Sims angiographic catheter (Cordis, Johnson and Johnson Ltd, Netherland). Case Reports Case 1 The patient, a 50-year-old woman, was a diagnosed case of carcinoma of right breast. She had already undergone modified radical mastectomy and was referred to our Center for placement of chemo port to facilitate the planned adjuvant chemotherapy. A chemo port was placed in the left subclavian vein under general anesthesia using classical Seldinger technique. A check X-ray in the postoperative period demonstrated that the catheter tip had malpositioned into contra lateral subclavian vein [Figure - 1a]. The patient was taken up for fluoroscopic-guided repositioning of the catheter the next day. Under local anesthesia, intravascular access was gained through the right femoral vein puncture and a 6 Fr sheath inserted. Through this sheath, the 5 Fr Sims angiographic catheter was first guided into the right internal jugular vein (IJV) along with a 0.035" PTFE guide wire (Medtrionic Vascular, Danver, MA,USA) [Figure - 1b]. Then the loop of the catheter was made, pulled down and rotated so that its tip wound around the malpositioned chemo port and snagged it [Figure - 1c]. During this maneuver, the PTFE guide wire remained in the catheter lumen to improve torque transmission. Subsequently, gradual gentle constant traction was applied on the Sims catheter till the malpositioned tip was repositioned into SVC [Figure - 1d]. Case 2 The patient, a 27-year-old man, was a diagnosed case of Refractory Hodgkin's Lymphoma Stage IVB who had undergone three different chemotherapy regimes on different occasions. As he continued to suffer from the disease, a bone marrow transplant was planned. He was referred to our Center for placement of Hickman's catheter. A Hickman's catheter was placed in the right subclavian vein under general anesthesia using classical Seldinger technique. However, postoperative check X-ray indicated that the catheter traversed the right innominate vein and malpositioned into the left subclavian vein instead of SVC, as expected [Figure - 2a]. The patient was taken up for fluoroscopic-guided repositioning of the catheter the next day. Under local anesthesia, venous access was gained via right transfemoral venous route and a 6 Fr sheath was placed in the right common femoral vein. Through this sheath, the 0.035" PTFE guide wire was inserted into the IVC and up to right IJV and the 5 Fr Sims angiographic catheter threaded over it [Figure - 2b]. Subsequently, the Hickman catheter was hooked with the curve of the Sims catheter. A gentle constant tug to Sims catheter attempted to pull the Hickman catheter tip down but failed as the Sims catheter tip straightened out and the traction was lost [Figure - 2c]. A third attempt at hooking the Hickman catheter was successful and the catheter was repositioned in the SVC [Figure - 2d]. Discussion Insertion of Ports, Groshong or Hickman catheters is a fairly routine practice in Oncology to provide a permanent central venous access for infusional chemotherapy, parenteral nutrition, or hemopoietic stem cell transplantation. Though radiological guidance in placing the CVAD has been demonstrated to result in smaller incidence of catheter malpositions, majority of the procedures are done by Seldinger technique using anatomical landmarks. [1] While some authors opine that clinical use of malpositioned catheters is associated with a few complications, [5] others argue that improper catheter tip position increases the risk of venous thrombosis and related complications. [3],[6] Moreover, if these catheters are not central venously located, the therapy may be painful and affect the non-central vein. The risk of catheter or vascular thrombosis is also higher, especially if the catheter tip is oriented against the venous blood flow. [7] Hence the displaced catheter either has to be removed and then re-inserted, or repositioned. Removal and reinsertion of the CVAD would entail another major procedure and its inherent risk in potentially immunocompromised patients, hence repositioning of the same CVAD would appear to be a more attractive option. Percutaneous transfemoral approach offers a minimally invasive option for repositioning of the malpositioned catheter. The procedure has previously been described in literature using vascular snare wire [4] and pigtail catheters. [8] In both our cases, we utilized the 5 Fr Sims angiographic catheter guided over the PTFE wire with successful outcome [Figure - 3]. The angiographic catheter is soft and malleable enough so as not to damage the chemoport and the PTFE guide wire provides the necessary torque and stiffness to the angiographic catheter so as to allow the "hook" of the angiographic catheter to apply necessary traction. Direct manipulation by tip-deflecting wires [9] and injection of saline [10] are other minimally invasive techniques described. The authors have no direct experience with the said techniques but it has been suggested that increased risk of infections is the drawback of direct manipulation by tip deflecting guide-wire and that vigorous injection of saline may be unsuccessful for the reasons that it seldom exerts sufficient force to reposition large-caliber central venous catheters. [4] The transfemoral approach described has inherent advantages such as it avoids a second surgery, decreases the patient's discomfort and can be done as a daycare procedure. Its limitation is that it requires a skilled operator and specialized angiographic suite to be carried out, which may not be universally available. Nevertheless, percutaneous transfemoral approach is a quick and convenient method to reposition the catheter tip in cases of malpositioned catheter tips in CAVDs such as chemo ports and Hickman's catheters. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10024f1c.jpg] [cr10024f1b.jpg] [cr10024f2b.jpg] [cr10024f1a.jpg] [cr10024f2a.jpg] [cr10024f2c.jpg] [cr10024f2d.jpg] [cr10024f3.jpg] [cr10024f1d.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}