 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
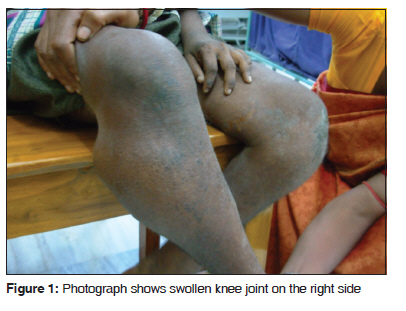
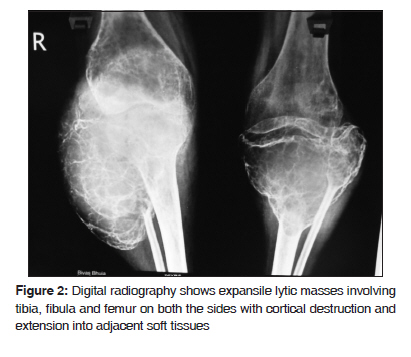
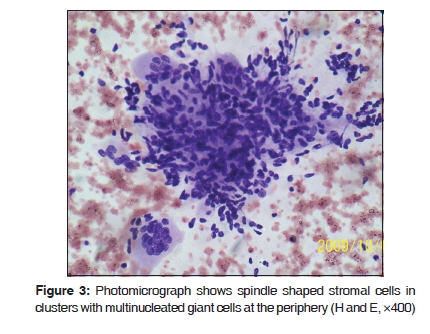
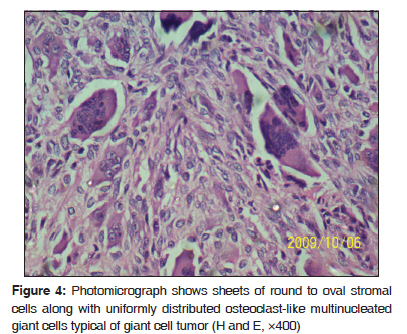
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 106-108 Case Report Synchronous multicentric giant cell tumor Ranjana Bandyopadhyay, Saumitra Biswas, Sanjay K. Bandyopadhyay1 , M. M. Ray2 Departments of Pathology, and 2 Orthopedics, Medical College, Kolkata- 700 073, Code Number: cr10025 DOI: 10.4103/0973-1482.63552 Abstract Multicentric giant cell tumors represent less than 1% of all giant cell tumors of bones. We report a case of multicentric giant cell tumors around both the knee joints in a mentally and physically challenged adult male that resulted in rapidly progressive painful swelling, restricted mobility and, ultimately, fixed deformity. These tumors had typical radiological appearance and the diagnosis was confirmed on histopathology.Keywords: Knee, multicentric giant cell tumor Introduction Giant cell tumors (GCT) account for 4-5% of primary bone tumors. [1] The typical presentation is a solitary lytic lesion involving metaphyseal-epiphyseal region of long bones of adults. About 1% of cases present with multiple synchronous or metachronous lesions and are designated as multicentric giant cell tumors (MCGCT). [2] About 101 such cases have been reported in literature till date. [3] Most of these cases are metachronously multicentric. We present a case of synchronous multicentric giant cell tumors around both knee joints. Case Report A 26-year-old male had presented with progressive painful swelling of both the knee joints (more on the right side) for one year, associated with deformity, pain on weight bearing and restricted mobility; rapidly giving rise to fixed flexion deformity. The patient was born out of non-consanguinous marriage and had normal birth history. However, his developmental (both motor and cognitive) milestones were delayed and any meaningful verbal communication was not possible as he was only able to utter incomprehensible words. There was no history of fever, vomiting, jaundice, lump abdomen, weight-loss, cough or haemoptysis of recent onset. On examination, the patient had short stature (below third percentile). A globular, hard swelling of 12×10×7 cm size was present around the right knee with stretched, glossy skin over the swelling [Figure - 1]. Local tenderness was present; movements were restricted in all directions and there was fixed flexion deformity. Around the left knee, a swelling of similar nature measuring (6×5×5) cm was present. There was no other bony or soft tissue swelling elsewhere. Rest of the examination was unrevealing. Routine hemogram was within normal range. Serum calcium, phosphorus, acid phosphatase and alkaline phosphatase levels were normal. Skeletal radiography revealed expansile lytic masses involving tibia, fibula and femur on both the sides with soap bubble appearance [Figure - 2]. The lesion on right fibula was largest; extending from metaphysis through epiphysis into the subchondral region. The cortices were expanded by the tumors with destruction and extension into adjacent soft tissues around upper end of right fibula. However, the joint space was free on both the sides. Computed tomography (CT) scan corroborated the radiographic findings. CT-guided aspiration was done from right fibula and left tibia. Cytomorphological features showed sheets of stromal cells, multinucleate osteoclastic giant cells and clustering of giant cells on the margins of stromal cell fragments [Figure - 3]. A diagnosis of GCT of bone was considered. Serum parathyroid hormone level was normal. Biopsy examination confirmed the cytological diagnosis and showed typical features of giant cell tumor: sheets of round to oval stromal cells along with uniformly distributed osteoclast-like multinucleated giant cells [Figure - 4]. The cytoplasm of stromal cell was eosinophilic with indistinct cellular outlines. There was no spindle area or storiform arrangement even at the periphery of the tumor. The tumor cells did not show any atypia and mitosis was only occasional. There were no obvious sarcomatous changes. The tumor on the right fibula showed secondary aneurysmal bone cyst-like changes. CT scan of thorax, abdomen and brain could not identify any metastatic deposit. Digital radiography of chest, small bones of hands and feet were normal. Considering the number, distribution and extent of lesions, resection of the tumor with arthrodesis using ipsilateral fibula after fixation with long intramedullary nail was performed on right side. On the left side, resection was followed by custom made prosthesis. Postoperative radiotherapy was contemplated, but the patient was lost to follow-up. Discussion GCTs make up (4-5)% of primary bone neoplasm cases with (40-50)% reported to occur around the knee. [1] MCGCTs are extremely rare and account for less than 1% of GCT. [2] Approximately 101 cases have been reported in the literature, most of them being single case report with only one large series involving 30 cases. [2],[3] Postulated pathogenic mechanisms of multicentricity include contiguous spread, iatrogenic tumor cell seeding, benign metastasis, malignant transformation and de novo formation. [3] The affected age group of MCGCT is reported to be younger than solitary one with majority presenting before the age of 20 years. [2],[3] However, as in case of solitary GCTs, female patients outnumber males. [2],[3] Most tumors arise in bones of lower extremity predominantly around the knee followed by proximal part of humerus and distal part of radius. [2] Dhillon et al. noted that unlike solitary GCT, MCGCTs more frequently involve the short bones of the hands and feet and is commoner in the meta-diaphyseal region of long bones. [3] However, fibula is not a common site for MCGCT. In a large series of 30 patients, only four tumors were reported in fibula. [2] Multicentricity in MCGCT can be synchronous (developing simultaneously or with in a period of six months) or metachronous (second tumor appears six months after the diagnosis of the first). Patients of MCGCT usually have two to three lesions but one patient with 10 tumors had been described in the literature. [4] In routine Roentgenogram, multicentric GCT must be differentiated from Brown tumor of hyperparathyroidism and from metastasis. [5] However, clinical, biochemical and radiological findings can guide the diagnosis if one considers the full continuum of findings, and their association with subject's medical history instead of focusing only on bone lesion. [6] Other remote possibilities like hydatid cyst of bone and osteomyelitis particularly tubercular osteomyelitis need to be excluded. [7] Appropriate serology and culture can exclude these possibilities. Although synchronous and metachronous GCTs are accepted as entities, it is impossible to exclude a metastatic process completely especially in those cases that are metachronous. [5] However, all the lesions were synchronous in this case. Screening for other metastatic sites including CT scan of thorax, abdomen and brain did not show any metastatic focus. Taking these facts into consideration, the present case can be taken as multicentric and not metastatic. Magnetic resonance imaging (MRI) is currently the best imaging modality since it allows accurate tumor delineation, extra-osseous extent and articular surface involvement. [8] CT is a reasonable alternative. [5] The radiographic features, cytomorphology, and histological characteristics of MCGCT do not differ from that of solitary tumors. However, some cases may contain fibroblastic and fibrohistiocytic areas. [2] McKinney et al. showed that multicentric or metachronous GCTs demonstrate aggressive behavior similar to that of primary GCT. [9] To conclude, the present case had six tumors - all of which started appearing at 25 years of age and were synchronous in all likelihood. Though fibula is not a common site for MCGCT, both right and left fibulae were affected in this patient with the largest tumor arising from the right fibula. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10025f3.jpg] [cr10025f2.jpg] [cr10025f4.jpg] [cr10025f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}