 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
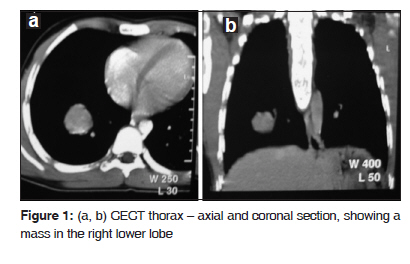
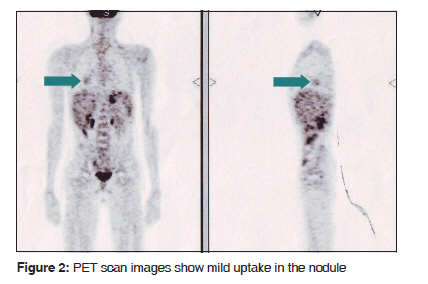
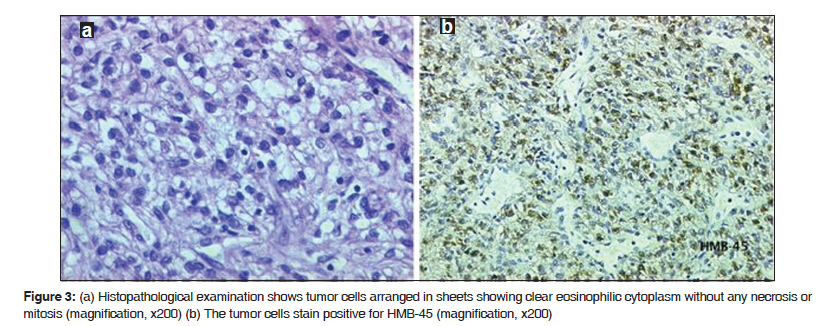
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 109-111 Case Report PEComa of the lung Vijayabhaskar R., Sanket S. Mehta, Kedar K. Deodhar1 , Pramesh C. S., Rajesh C. Mistry Departments of Surgical Oncology and 1 Pathology, Tata Memorial Hospital, Mumbai, India Code Number: cr10026 DOI: 10.4103/0973-1482.63548 Abstract Perivascular epithelioid cell tumor (PEComa), also called clear cell ''sugar'' tumor of the lung, is a rare benign tumor arising from perivascular epithelioid cells (PECs). We report a case of a 15-year-old boy who presented with right lower lobe lesion which turned out to be a clear cell tumor of the lung. An [18F]-fluoro-2-deoxy-D-glucose (FDG) - positron emission tomography (PET) scan revealed mild FDG uptake in the lung lesion (SUV<1) with no active uptake elsewhere in the body. We discuss the clinical, radiologic and immunohistochemical features of clear cell ''sugar'' tumor of lung and compare them with published literature.Keywords: Benign lung tumor, clear cell tumor, PEComa, sugar tumor Introduction Benign tumors of the lung are uncommon and account for less than one per cent of all lung tumors. [1] Perivascular epithelioid cell tumors (PEComas), also called 'sugar' tumors or clear cell tumors of the lung (CCTL) are rare benign neoplasms, which had originally been described by Liebow and Castleman. [2] The name 'sugar tumor' is given due to the high glycogen content in the cytoplasm. Definitive preoperative diagnosis is difficult owing to its rarity. As less than 50 cases have been published so far, [3] there is a scarcity of detailed literature on this tumor. We report a case of clear cell tumor of the lung in a young boy treated by surgical resection. Case Report A 15-year-old boy presented with a two-year history of vague chest pain and breathlessness. Chest X-ray showed a solitary nodule in the lower zone of right lung field. A contrast enhanced computed tomography (CECT) scan of the chest [Figure - 1]a and b showed a 4 × 2.2 × 2.8 cm mass in the lower lobe of right lung. The nodule showed heterogeneous enhancement in CECT (50-85 HU). CT-guided biopsy of the lung mass showed a mesenchymal tumor without any unequivocal features of malignancy. An [18F]-fluoro-2-deoxy-D-glucose (FDG)-positron emission tomography(PET) scan revealed mild FDG uptake in the lung lesion (SUV< 1) with no active uptake elsewhere in the body [Figure - 2]. We decided on surgical resection as the boy was symptomatic and the mass was solid on CT scan. After relevant investigations, he underwent right lower lobectomy and had an uneventful postoperative recovery. Gross examination showed a yellowish brown, well circumscribed tumor with well defined margins, measuring 3 × 3 × 2 cm in the central region. Histopathological examination [Figure - 3]a showed a tumor composed of cells with sheeted appearance and scant stroma interspersed with thin walled blood vessels. The tumor cells had clear to pale eosinophilic cytoplasm, low nuclear to cytoplasmic ratio, well defined cell borders and inconspicuous mitotic activity without any necrosis. Immunohistochemistry showed that the tumor cells were negative for cytokeratin, epithelial membrane antigen (EMA), synaptophysin, chromogranin, S-100, thyroid transcription factor-1, surfactant protein, CD31, desmin, mucin, CK-7, C-kit and smooth muscle actin. The tumor cells were, however, positive for HMB-45 [Figure - 3]b. The overall features favored a diagnosis of PEComa of the lung. The patient is asymptomatic and disease-free on a six-month follow-up. Discussion PEComas are a group of mesenchymal neoplasms that incorporates angiomyolipoma, lymphangiomyomatosis, clear cell tumors of lung (CCTL) and a set of similar visceral and soft tissue lesions that are all characterized by the 'perivascular epithelioid cell'. [4] Although CCTL usually occur in adults in the age group of 40 to 50 years, [5] they can occur in any age group (range 8-73 years) and have a slight female predominance. [6] Most lesions are solitary, asymptomatic, located within the peripheral lung and pose a significant diagnostic problem. Hemoptysis and high fever are rare presenting symptoms of CCTL. [7],[8] Our patient presented with symptoms of shortness of breath and chest pain which is unusual for such type of tumor. CCTL radiographically presents as a round, peripheral parenchymal nodule with no evidence of cavitation or calcification. On CECT scans, they might show intense post-contrast enhancement, due to its rich vascular stroma. [7] Macroscopically, CCTL appears as a pink nodule of about 2 cm (range, 1-6.5 cm) that is well demarcated from the lung parenchyma, unencapsulated, without necrosis or bleeding. Microscopic study shows typical large cells with clear abundant cytoplasm, without atypia or mitoses, consistent with a benign tumor; CCTL is characterized immunohistochemically by immunoreactivity for HMB-45, and nonreactivity for cytokeratin or EMA. [6] CCTL should be distinguished from clear cell carcinoid of lung, metastatic renal cell carcinoma, metastatic melanoma, granular cell tumors, oncocytoma and acinic cell tumor. [5,6] CCTL is traditionally considered benign, with only one argued report of fatal recurrence and metastasis. [9] Size > 2.5 cm, necrosis, mitotic index of 1 per 50 high-power fields, marked pleomorphism and nuclear atypia could point to a malignant potential. [10] The rarity of these tumors and the paucity of published literature makes it difficult to make strong recommendations for management. However, according to WHO guidelines, excision is the treatment of choice and no adjuvant therapy is recommended. [6] In conclusion, our case underlines the atypical presentation of benign clear cell tumor of lung. PEComas should be considered in the differential diagnosis of lung nodules in younger population. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10026f2.jpg] [cr10026f3.jpg] [cr10026f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}