 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
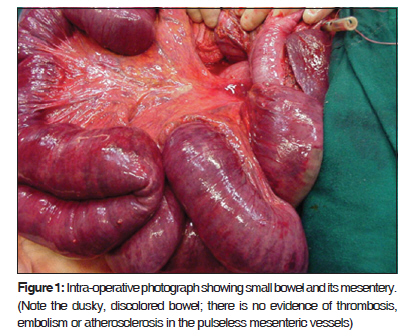
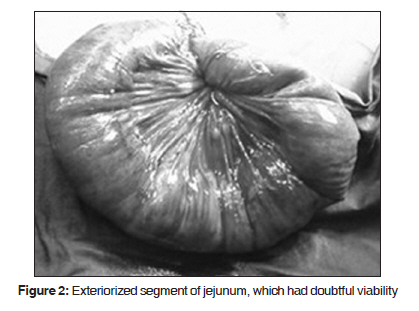
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 112-113 Case Report Fatal non-occlusive mesenteric ischemia after esophagectomy Sajid S. Qureshi, Rakesh S. Neve, Sudip A. Raina, Rajesh C. Mistry Department of Thoracic Services, Tata Memorial Hospital, Mumbai, India Code Number: cr10027 DOI: 10.4103/0973-1482.63546 Abstract Non-occlusive mesenteric ischemia (NOMI) is a disorder with an extremely high mortality. Salvage of affected patients requires early recognition and aggressive intervention to prevent intestinal gangrene. We present a case of NOMI developing after esophagectomy and discuss the pathophysiology diagnosis and therapy.Keywords: Esophagectomy, non occlusive mesenteric ischemia, enteral feeding Introduction Non-occlusive mesenteric ischemia (NOMI) has been defined as diffuse intestinal ischemia that often results in intestinal gangrene in the presence of patent arterial trunk. [1],[2] The mortality rate for this intestinal disorder remains high up to 70%. This dismal prognosis is due to failure of antemortem diagnosis and an incomplete understanding of the pathophysiology. [3] NOMI after esophagectomy is rare, with only three cases reported in English literature. [4] We report a case of NOMI developing after esophagectomy and discuss its pathophysiology, diagnosis and treatment. Case Report A 58-year-old male presented with history of Grade III dysphagia of three months duration. Relevant investigations revealed the presence of squamous cell carcinoma of the middle third of esophagus, which was deemed resectable. Patient had a history of myocardial infarction six years back and was on ACE inhibitors and nitrates. A 2D Echo showed hypokinesia and thinning of left ventricle with a left ventricular ejection fraction of 45%. The patient had a good effort tolerance and was able to climb two flights of stairs. A transthoracic total esophagectomy with mediastinal and abdominal lymphadenectomy was performed. The procedure was uneventful with 600 ml blood loss, which was adequately replaced with blood and crystalloids. The total duration of surgery was five hours. Postoperatively, the patient had normal vitals and jejunostomy feeds were initiated on the second postoperative day. On the third day the patient developed abdominal distension, however, there was no tenderness or guarding. In addition, there was an episode of supraventricular tachycardia, which reverted to sinus rhythm spontaneously. Suspecting an anastomotic leak and mediastinitis a CT scan of the chest was performed which revealed the presence of mediastinal collection. On exploration, the gastric tube was congested with sloughing at the anastomotic site. The entire small and large bowel was dusky with two patches of gangrene in the jejunum. The major mesenteric vessels had no pulsation though; there was no evidence of thrombosis, embolism or atherosclerosis [Figure - 1]. Attempts at restoring the vascularity with warm saline packs and 100% oxygen failed. In view of the poor general condition of the patient the stomach tube was disconnected and the gangrenous jejunum exteriorized [Figure - 2]. Postoperatively, the patient′s condition deteriorated and he succumbed after three hours. Based on the perioperative and post-mortem finding a diagnosis of NOMI leading to bowel ischemia and gangrene was established. Discussion NOMI, first documented by Thorek in 1934, accounts for 20-30% cases of acute mesenteric ischemia with an overall incidence of one case for every 5000 hospital admission. [1],[3],[5] The etiology of NOMI is poorly understood. Mesenteric vasospasm is a sine qua non of NOMI which persist even after correction of the precipitating event. Vasopressin and Angiotensin are the putative neurohormonal mediators. [1] Ischemic reperfusion injury due to production of toxic oxygen free radicals and uric acid may also complicate NOMI, since the hypo perfusion may be partial and occasionally repetitive. [1],[2],[3] NOMI has also been documented after initiating enteral feedings. This may be due to increasing metabolic demands for absorption, secretion and metabolism, which outstrips the ability of mesenteric vascular system to supply the necessary blood flow. The increased metabolic rate in combination with a marginal or decreased oxygen supply can result in intestinal ischemia. [1] The other theories put forth for NOMI are intestinal hypoxia, and infection. [1],[2] Diagnosis of NOMI requires a high index of suspicion, especially in elderly patients, and patients with history of myocardial infarction, cardiac arrhythmia′s, congestive heart failure, generalized atherosclerosis and patients undergoing major cardiac or intra-abdominal operations. [2],[3],[5] NOMI after esophagectomy is rare and only three cases have been reported. [4] Definitive diagnosis of NOMI requires arteriographic study. Treatment of NOMI is essentially pharmacologic after control of the precipitating event and maintaining hemodynamic stability. [3],[5] If peritoneal signs do not improve, an exploratory laporotomy is performed. Nonviable bowel is excised and intestinal continuity maintained if the margins are unequivocally viable, otherwise exteriorization is advised. Broad-spectrum antibiotics are given to prevent septic complication due to bacterial translocation and peritonitis. [1],[5] Our patient was an elderly person and had undergone major esophageal surgery. He had the sequelae of the previous myocardial infarction; however the overall general condition and effort tolerance encouraged for opting surgery over other modality for a seemingly resectable disease. Although the surgery was complete and uneventful, the occurrence of the exceptional complication of NOMI proved fatal. In retrospect, the cardiac status, extensive surgery and probably the enteral feedings were the precipitating factors for the development of NOMI. Although the diagnosis of NOMI was confirmed after until the literature search, the rapid fulminant course could have precluded any active intervention. A similar rapid fulminant course had been described by Hokamura et al. after esophagectomy. [4] Conclusion Considering the rarity of NOMI, except for a high index of suspicion in patients with high risk factors for NOMI no further recommendations could be made. In patients in whom the diagnosis is confirmed early initiation of therapy is of paramount importance for successful management. Although esophagectomy can be performed with reasonable safety, patients with high risk features, in addition to the allied complications, NOMI should also be considered in the differentials. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10027f1.jpg] [cr10027f2.jpg] |
| |||||||||

{kind=link}
{kind=link}