 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 114-116 Case Report Follicular dendritic cell sarcoma of the neck with an aggressive and fatal course Sanju Cyriac, David Praveenkumar, Urmila Majhi 1 , T. Gnana Sagar Departments of Medical Oncology and 1 Pathology, Cancer Institute, Chennai, India
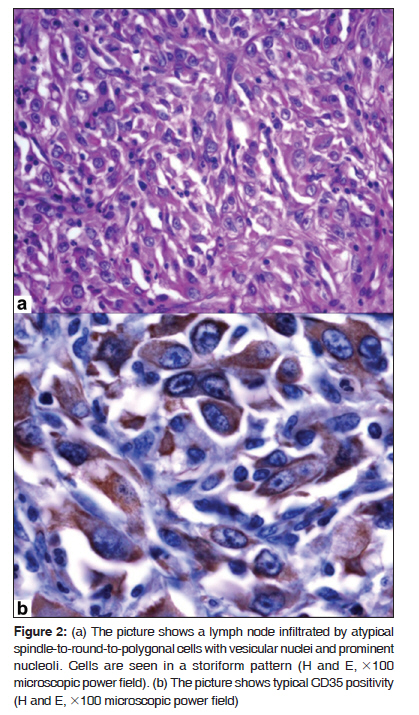
Code Number: cr10028 DOI: 10.4103/0973-1482.63545 Abstract Dendritic cell neoplasms are rare malignancies described with an increased frequency. They often involve the lymph nodes, but extranodal presentations are also described. The disease often has an indolent course. Surgery is the main modality though chemotherapy and radiation have also been tried. We present here a case of a 69-year-old male diagnosed to have follicular dendritic cell sarcoma of the neck which had a rapid and fatal course inspite of chemotherapy and radiotherapy. More studies are required to assess the biology of this rare tumor.Keywords: Dendritic cell neoplasm, immunohistochemistry, sarcoma Introduction Dendritic cell neoplasms are rare malignancies arising from the antigen-presenting cells in the lymph node. The disease has an indolent course and was first described in 1986 by Monda et al. [1] Since then, nearly 200 cases have been described in the world literature. The disease is recognized more frequently with sensitive immunohistochemical markers. A standard treatment option is lacking. A recent analysis of all cases reported so far by Tommaso et al. interestingly showed that a trimodality treatment had the best outcome. [2] Case Report A 68-year-old gentleman presented with gradually increasing swelling in the left lower neck. He was otherwise asymptomatic. Physical examination revealed left, level IV lymph nodal swelling, 10 x 10 cm, firm, and nontender. The patient had ECOG score 1 performance status. His systemic examination was unrevealing. Routine investigations showed normal hemogram and renal and liver function tests. Imaging of the neck was done [Figure - 1]a. Biopsy of the left, level IV cervical lymph node was performed [Figure - 2]. Immunohistochemical stains for CD35, vimentin, S100, CD23, and Bcl-2 were positive and those for LCA, CD3, and CD68 were negative. Ki 67 was 40-50%. The final diagnosis was follicular dendritic cell sarcoma/tumor (FDCS/T). Since the tumor was locally advanced with internal jugular vein thrombus, he was not considered for upfront surgery. Hence we initiated him on COP chemotherapy. There was progression after the first cycle of therapy [Figure - 1]b. Hence, radiotherapy was also considered which he received in 15 fractions (200 cGy/day), but the tumor mass progressed further causing progressive tracheal compression and hypoxia and he died 2 months after the diagnosis was made. Discussion Dendritic cell neoplasms are being recognized with an increasing frequency. They arise from antigen-presenting cells, and occur primarily in lymph nodes [1] and also in extranodal sites. [2],[3] They were previously classified as lymphomas, sarcomas, or histiocytic neoplasms. Various classification systems have been advocated. WHO classifies dendritic cell neoplasms into five groups: Langerhans′ cell histiocytosis, Langerhans′ cell sarcoma, interdigitating dendritic cell sarcoma/tumor (IDCS/T), follicular dendritic cell sarcoma/tumor (FDCS/T), and dendritic cell sarcoma, not specified otherwise. [4] Pileri et al. recently proposed a classification of dendritic cell neoplasms based on morphological and immunophenotypic characteristics. [5] Feldman et al. [6] studied eight patients with both follicular lymphomas and histiocytic/dendrtic cell sarcomas. All eight H/DC tumors showed a presence of the t(14;18) either by FISH, or by PCR, and hence they suggested a common clonal origin. FDCS/T is the most common subtype (70%) of dendritic cell neoplasms. It typically has an indolent course with a metastatic potential. [7] Median age of occurrence is 46 years, and is more common in males (male:Female, 1.4:1). De Pas et al. analyzed 184 cases of dendritic cell sarcoma reported to date. [2] A total of 60% of the cases occurred in the lymph nodes. The disease was more frequently localized at diagnosis in patients with FDCS than in those with IDCS (84.7% versus 60%). The mortality in various case series ranges from 6 to 58%. Patients with an abdominal disease have an aggressive clinical course. Histologically, the most common patterns are storiform, fascicular, and whorled with sprinkling of small lymphocytes throughout the tumor. The neoplastic cells of FDCS/T characteristically show a spindle quality. The most common differential diagnoses are thymoma and meningioma. Immunohistochemistry has played an important role in bringing this often-misdiagnosed tumor into light. Typically, the tumor cells are positive for markers of follicular dendritic cells, i.e., CD21, CD23, and CD35. The cells are also usually positive for vimentin, fascin, HLA-DR, and EMA. They are variably positive for S100 and CD68. Markers like CD1a, lysozyme, CD34, CD3, CD79a, CD30, HMB45, and CK are consistently negative. Since only about 200 cases have been reported worldwide, there is no consensus on the treatment of this rare disease. Surgery has remained the mainstay in localized disease. But the recurrence rate can be as high as 50%. [2] Hence adjuvant treatment is warranted. The relapse rates were better with radiotherapy compared to chemotherapy (23.1 vs. 62.5%). Interestingly, there were no relapses when a trimodality approach was used. In recurrent and advanced settings, various chemotherapeutic agents have been tried, including CHOP, ABVD, DHAP, EPOCH, ICE, cisplatin/epirubicin, with limited responses. The prognosis has been universally poor. Recently, there was a case report of using PEG liposomal doxorubicin in an adjuvant setting in a case of FDCS/T of the neck. [8] Our patient was 68 years old, had locally advanced disease with tracheal compression, and was irresectable. Hence chemotherapy was tried but showed no response; rather, progression was present. Hence radiotherapy was also tried. The patient had progressive disease and succumbed to his illness. Such aggressive course of disease outside the abdomen is unknown. Voigt et al. presented a paratracheal FDCS/T with tracheal compression which was treated successfully with tracheal stenting, and subsequently radiotherapy with gemcitabine as the radiosensitizer. [9] Since there are limited data on this rare disease, it is advisable to publish and share the knowledge about the presentations and treatment responses. In view of increased recognition, further researches may be initiated to assess the response to various treatment regimes. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10028f1.jpg] [cr10028f2.jpg] |
| |||||||||

{kind=link}
{kind=link}