 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
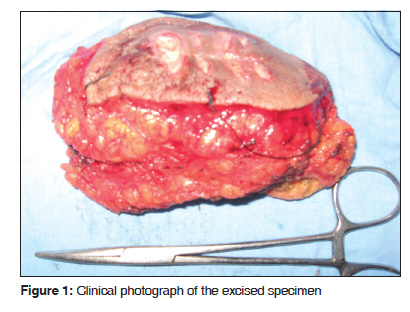
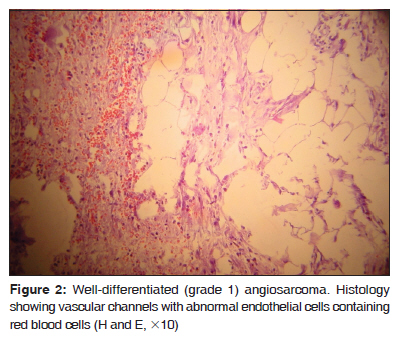
Journal of Cancer Research and Therapeutics, Vol. 6, No. 1, January-March, 2010, pp. 120-122 Case Report Primary angiosarcoma of the breast in a postmenopausal patient Vinayak S. Rohan, Abhinandan M. Hanji 1 , Jayesh J. Patel 1 , Rajen A. Tankshali 1 Department of Surgical Oncology, Kasturba Medical College, Manipal, India, Code Number: cr10030 DOI: 10.4103/0973-1482.63543 Abstract Primary angiosarcoma of the breast is a rare entity forming 0.04% of primary breast tumors. It is a highly aggressive tumor with a high propensity for locoregional and distant metastasis. Surgery in the form of mastectomy or wide excision remains the cornerstone of treatment. Radiotherapy and chemotherapy have been tried with varying results.Keywords: Angiosarcoma, chemoradiotherapy, mastectomy Introduction Primary angiosarcoma of the breast is a rare and highly aggressive tumor. It forms 0.04% of all the breast tumors and approximately 8% of breast sarcomas. [1],[2] It is most commonly seen in young patients (30-50 years). These tumors have a high propensity for distant metastasis with 8-50% 5-year survival. [3] These tumors usually develop as a complication of a preexisting condition . Prior radiation and lymphedema are associated with secondary angiosarcoma of the breast. [4] The etiology of primary angiosarcoma remains unknown. Surgery in the form of mastectomy or wide excision (lumpectomy) remains the cornerstone of treatment. Radiotherapy and chemotherapy have been tried with varying results. Here we present a case of a 60-year-old postmenopausal woman with primary angiosarcoma of the breast presenting to our institute. Case Report A 60-year-old postmenopausal female presented with a lump in the left breast. There was no history of pain or nipple discharge. There was no previous history of radiation. On mammary examination, the patient had an oval lump, located on the lower outer quadrant of the left breast, 5 x 5 cm in diameter, smooth and elastic in consistency, and having bosselated contours. She did not have any suspicious axillary lymphadenopathy. FNAC and a tru-cut biopsy done outside were inconclusive. Mammography was not possible due to the hematoma secondary to the attempted tru-cut biopsy done outside. Sonography of the breast revealed a cystic lesion of 4.1 x 3.2 cm with an internal hypoechoic mural nodule with internal vascularity. Abdominal sonography, CT of the thorax, and a bone scan were normal. Incisional biopsy was undertaken which revealed angiosarcoma of the breast. The patient underwent lumpectomy with wide margins [Figure - 1]. Histopathology revealed a 4 x 4 cm mass with the features of a well-differentiated angiosarcoma with marked proliferation of atypical capillaries and endothelial cells [Figure - 2]. The skin was free of the tumor. All the margins of resection were free of the tumor. Immunohistochemistry showed positivity for factor VIII-related antigen and CD34. The patient is free of recurrence and metastasis 10 months after the completion of the treatment. Discussion Schmidt in 1887 described the first case of angio sarcoma of the breast. [5] In general, it is seen in the younger population during their third or fourth decade of life but our patient was 60 years old. Angiosarcoma can arise in the soft tissue, bone, or skin. Four variants of cutaneous angiosarcoma are currently recognized, including angiosarcoma of the scalp and face, angiosarcoma in the context of lymphedema (Stewart-Treves syndrome), radiation-induced angiosarcoma, and epithelioid angiosarcoma. The etiology of most of the cases of angiosarcoma is unknown. The tumors may develop as a complication of a preexisting condition. The risk factors for the development angiosarcoma are chronic lymphedema (radical mastectomy- Stewart-Treves syndrome or radical inguinal lymphadenectomy-Kettle′s syndrome), radiotherapy, foreign material introduced in the body like Dacron, shrapnel, steel, plastic graft material, surgical sponges, bone wax, and environmental carcinogens like arsenic, dioxin, and vinyl chloride. Multiple studies have established an association between radiation therapy and breast angiosarcoma, especially after breast-conserving surgery. [4],[6] Huang and Mackillop reported a 16-fold increased risk (95% CI, 6.6-38.0). [4] Lesions tend to develop 4-7 years after therapy, and may be due to persistent lymphedema. The diagnosis of angiosarcoma can be challenging. Mammogram may show a nonspecific mass, and up to one-third of the patients have no abnormalities. [7] MRI has become a useful tool for diagnosis. [8] FNAC has a low specificity with a false negative rate of 37%. [9] Histologically, angiosarcomas of the breast are classified into three grades: Grade 1 to Grade 3 or well to poorly differentiated. It was believed that histologic grading of mammary angiosarcomas plays an important role in prognostication, but a recent study has shown that there is no correlation between histologic grade and patient outcome. Differential diagnosis of this rare malignancy includes benign hemangioma, cystosarcoma phyllode, stromal sarcoma, metaplastic carcinoma, squamous cell carcinoma with sarcomatoid features, myoepithelioma, fibromatosis, fibrosarcoma, liposarcoma, and reactive spindle cell proliferative lesions. An ultrastructural examination can reveal Weibel-Palade bodies and pinocytic vescicles under the electron microscope. Immunohistochemistry can show positivity for factor VIII antigen, CD34, CD31, Ulex lectin, desmin, and vimentin. CD31 appears to be the most promising marker. [6] The treatment is primarily surgical, either by mastectomy or wide excision. [10] There is no role of axillary dissectiondue to the low incidence of axillary metastasis. [11] The role of adjuvant therapy with radiotherapy and chemotherapy is equivocal. This is because of the small sample size in studies and the selection bias. Although there is no survival advantage, adjuvant radiotherapy has shown to reduce the local recurrence of the tumor. [11] It is reasonable to offer radiotherapy if there is a high risk of microscopic residual disease. Metastatic tumors have shown response to combination cytotoxic chemotherapy (up to 48%) which suggests that angiosarcoma is likely to be a chemosensitive disease. Chemotherapy should be considered for patients with high-risk, localized breast angiosarcoma. [11] Angiosarcoma carries a poor prognosis. Five-year survival ranges from 8 to 50%. [3] Distant metastases have been seen in lung, skin, liver, bone, CNS, spleen, ovary, and heart. The nodal metastasis rate is low (6%). [11] The prognostic factors for sarcoma of the breast include the tumor size, presence of residual disease, and cellular pleomorphism. [12],[13] According to a recent report, grade of the tumor may not be an important prognostic factor. [14] Conclusion Primary angiosarcoma of the breast is a rare malignancy with a poor prognosis. Although surgery is the primary treatment, due to a high propensity for locoregional and distant failure, multimodality treatment should be considered. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10030f2.jpg] [cr10030f1.jpg] |
| |||||||||

{kind=link}
{kind=link}