 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
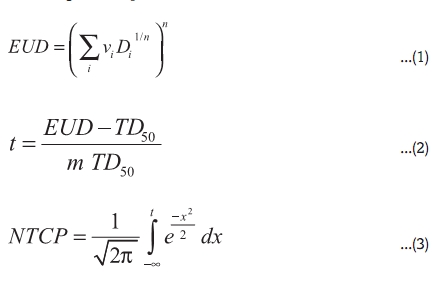
Journal of Cancer Research and Therapeutics, Vol. 6, No. 2, April-June, 2010, pp. 194-198 Original Article Helical tomotherapy for head and neck squamous cell carcinoma: Dosimetric comparison with linear accelerator-based step-and-shoot IMRT Vedang Murthy, Zubin Master, Tejpal Gupta, Sarbani Ghosh-Laskar, Ashwini Budrukkar, Reenadevi Phurailatpam, Jaiprakash Agarwal Department of Radiation Oncology, Tata Memorial Hospital and Advanced Centre for Treatment, Research and Education in Cancer (ACTREC), Tata Memorial Centre, Navi Mumbai, India Correspondence Address: Dr. Vedang Murthy, Consultant Radiation Oncologist, Tata Memorial Hospital and Advanced Centre for Treatment, Research and Education in Cancer (ACTREC), Tata Memorial Centre, Navi Mumbai, India. vmurthy@actrec.gov.in Code Number: cr10042 PMID: 20622367 DOI: 10.4103/0973-1482.65245 Abstract Background: Linear Accelerator-based Intensity Modulated Radiation Therapy (IMRT), either as step-and shoot (SS) or in dynamic mode, is now considered routine in the definitive management of head and neck squamous cell carcinoma (HNSCC). Helical TomoTherapy (HT) is a new platform to deliver IMRT. This study aims to compare step-and-shoot Intensity Modulated Radiation Therapy (SS IMRT) with dynamic Helical TomoTherapy (HT) dosimetrically in patients with head and neck squamous cell carcinoma (HNSCC).Materials and Methods: Twelve patients with HNSCC, previously treated with SS IMRT, were re-planned on HT using the same CT dataset. Plans were compared for target coverage and organs-at-risk (OARs) sparing. Sparing of parotids was assessed after stratifying for side (contralateral vs. ipsilateral) and site of disease (laryngopharynx vs. oropharynx). Normal tissue complication probabilities (NTCP) were also compared for the parotid glands. Results: All HT plans showed improvement in target coverage and homogeneity, and reduction in OAR doses as compared to SS IMRT plans. For PTV 66, the mean V 99 improved by 14.65% ( P = 0.02). Dose Homogeneity (D 10-90 ) was significantly better in the HT plans (mean 2.07Gy as compared to 4.5Gy in the SS IMRT plans, P = 0.02). HT resulted in an average reduction of mean parotid dose of 12.66Gy and 18.28Gy for the contralateral and ipsilateral glands ( P = 0.003) respectively. This translated into a 24.09% and 35.22% reduction in Normal Tissue Complication Probability (NTCP) for the contralateral and ipsilateral parotids respectively ( P < 0.01). Site of disease (laryngopharynx vs. oropharynx) did not have any significant impact on parotid sparing between SS IMRT and HT. The maximum dose to the spinal cord showed a mean reduction of 12.07Gy in HT plans ( P = 0.02). Conclusion: Helical Tomotherapy achieved better target coverage with improved OAR sparing as compared to SS IMRT. The significant reduction in mean parotid doses translated into meaningful reduction in NTCP, with potential clinical implications in terms of reduction in Xerostomia and improved quality of life in patients with HNSCC. Keywords: Dosimetric comparison, intensity modulated radiation therapy, normal tissue complication probabilities, tomotherapy Introduction The paradigm of conformal radiotherapy in contemporary radiotherapy practice has been ushered with widespread adoption of three-dimensional conformal radiotherapy (3D-CRT) and intensity modulated radiation therapy (IMRT) with their promise to improve the therapeutic index by increasing target volume coverage while reducing doses to surrounding organs-at-risk (OARs). [1],[2] IMRT has been credited with the ability to generate highly conformal including concave dose distributions, with particular relevance in head and neck squamous cell carcinoma (HNSCC) due to their complex target volumes, proximity to critical structures, and a well-defined dose-response relationship. Parotid-sparing IMRT has shown promising results in prospective studies by reducing the severity of xerostomia and maintaining quality of life parameters. [2] Even though IMRT plans are dosimetrically superior to conventional techniques, comprehensive long-term efficacy and toxicity data are still awaited. [3] Helical TomoTherapy (HT) has emerged as a promising and innovative technology platform for achieving highly conformal dose distribution to large and complex target volumes. A 6 MV linear accelerator (linac) mounted on a slip-ring gantry continuously rotates around the patient to deliver radiation in helical mode as the patient translates through the ring. The fan beam is modulated as a function of the gantry angle via a binary multileaf collimator (MLC) with 64-leaves, each of which projects 0.625cm at the iso-center. Due to large number of beam angles per gantry rotation (51 projections) and ultra-fast MLCs (20ms to open or close), a very high level of intensity modulation can be achieved. Xenon detectors, fitted opposite the linac, are used to acquire megavoltage computed tomography (MVCT) images for patient set-up verification, giving the system image-guidance capabilities. At our center, IMRT for HNSCC is being performed in the form of an ongoing randomized trial comparing inversely planned step-and-shoot IMRT (SS IMRT) with forward planned 3D-CRT. We have also recently commissioned the HT unit, Hi-ART II (TomoTherapy Inc., Madison, WI). This is a dosimetric comparison between the clinically utilized SS IMRT plans and corresponding HT plans in 12 patients with HNSCC. The aim of this study was to assess the potential of HT to improve the therapeutic ratio over conventional SS IMRT in HNSCC and report the dosimetric parameters thus obtained. Materials and Methods The CT datasets of 12 patients (six each with laryngo-pharyngeal and oropharyngeal primaries) previously treated with definitive SS IMRT on a prospective trial were selected for this dosimetric study. Patients had biopsy proven non-metastatic HNSCC (stages T1-3, N0-2b). Our process of planning SS IMRT has been described recently. [4] Briefly, patients were immobilized in supine position in a customized thermoplastic mask and planning axial CT images acquired with intravenous contrast using a slice thickness of 3 mm. Contouring was done on a third party contouring workstation (Coherence Dosimetrist version 2.2, Siemens Medical Solutions, USA). Target volumes including primary tumor, involved lymph nodes, and lymph node regions at risk of occult metastases were delineated according to consensus guidelines. [5] All surrounding critical normal structures, including both parotid glands and spinal cord, were contoured as OARs. The same target volumes and OARs delineated for the original SS IMRT plans were also used for HT planning. Complementary HT plans were generated by a planner blinded to the dosimetric parameters achieved by the SS IMRT plans. Linac-based SS IMRT Linac IMRT plans were realized on the inverse treatment planning (ITP) module of Plato Sunrise (version 2.7.4, Nucletron BV, Veenendaal, Netherlands). Plato Sunrise ITP used for planning has been configured and commissioned for 6 MV photons from Siemens Primus Linac (Siemens Medical Solutions, USA). The linac is equipped with a multileaf collimator (MLC) with 29 pairs of leaves (27 pairs project 1 cm and the peripheral two pairs project 6 cm at isocenter). It uses a convolution algorithm for dose computation and gradient-search algorithm for optimization. The chosen calculation grid size was 2 mm with inhomogeneity correction turned on. The primary aim during planning was to achieve clinically acceptable target volume coverage with optimal OAR sparing. The SS IMRT plans were generated with seven to nine equally spaced beams (angular spacing between beams was 40-51°). ICRU 50 guidelines for conformal radiotherapy were used to define our plan acceptance criteria for target coverage, viz. at least 95% of the PTV must be covered by 95% of the prescription iso-dose. The same acceptance criteria were used for HT planning as well. HT-based IMRT HT plans were generated on TomoTherapy treatment planning station (version 2.2.4, TomoTherapy Inc., USA), using identical CT dataset. The TomoTherapy planning system uses a convolution-superposition algorithm for dose calculation and a least squares minimization function for optimization during inverse planning. Treatment planning parameters unique to TomoTherapy are field width, pitch, and modulation factor. The field width is the thickness of the fan-beam selected for treatment. Most HT units are commissioned with three clinical field widths (1cm, 2.5cm and 5cm). The pitch is the distance traveled by the couch per gantry rotation as a fraction of the field-width. The modulation factor determines the speed of gantry rotation. For all 12 cases, a field width of 2.5 cm, pitch of 0.3, and maximum modulation factor of 3-3.5 was used during optimization. The main focus during planning was achieving acceptable target coverage with optimal organ sparing. Dose prescription The simultaneous integrated boost (SIB) technique was used for planning and delivery. The gross disease (primary site and involved nodes) with margins (PTV66) was prescribed a dose of 66 Gy in 30 fractions, while the elective high-risk volume (PTV60) received 60 Gy in 30 fractions in both linac-based as well as HT-based techniques. Plan evaluation The dosimetric outcome of the SS IMRT and HT plans were compared quantitatively in terms of target coverage, dose homogeneity, and OAR sparing. For the primary target volume (PTV66), the dose coverage was assessed by comparing the volume of the PTV66 that received 95%, 99% and 107% of the prescription dose of 66Gy (V 95% , V 99% and V 107% ). To quantify hot and cold spots (of a significant volume within the target), the dose to 1% and 99% of the PTV66 (D 1 and D 99 ) was also compared. The homogeneity of the dose coverage of the target was quantified by calculating the difference between the dose received by 10% and 90% of the PTV66 (D 10-90 ). Parotid sparing was compared using the mean dose and the dose to 33%, 66% and 100% of the parotid volume (D 33 , D 66 and D 100 ). The parotids were grouped as ipsilateral and contralateral, to ascertain sparing by laterality. For the spinal cord, maximum dose was compared. Apart from the parotids and the spinal cord, the doses to proximal critical structures were well within tolerance (or within the target volume) for both modalities, and thus we have concentrated on only the parotids and the spinal cord. For each technique, dosimetric data is reported as mean of all 12 datasets along with the Standard Deviation (Mean ± SD). Statistical significance testing was done using the Wilcoxon Signed rank test, considering the non parametric nature of the data. Overlap priority The target volumes were delineated such that PTV66 was completely contained within the PTV60 volume. This led to a situation wherein the PTV60 could not be compared for parameters related to quantifying homogeneity (D 10-90 ) and 'hot-spots' (D 1 and V 107% ). The two planning systems handle volume-within-volume differently and hence calculate such Dose-Volume Histogram (DVH) in a different manner. In TomoTherapy, one can assign priorities to overlapping volumes (PTV66 and PTV60) such that voxels contained in the overlap volume belong to the volume with higher priority. In Plato, voxels of the overlap volume are considered as part of both volumes, irrespective of overlap priority. Due to this fundamental difference in the way the planning systems consider overlapping volumes, it would be inappropriate to make a head-to-head comparison of several parameters of these overlapping structures. Normal tissue complication probability (NTCP) NTCP was calculated to assess the biological significance of parotid gland sparing. A DVH reduction scheme suggested by Niemierko [6] was used, where the DVH of a specific organ was reduced to a single dose, called Equivalent Uniform Dose (EUD). If the entire organ is irradiated uniformly to this EUD, it leads to the same NTCP as the actual non-uniform dose distribution and thus the EUD is representative of this non-uniform distribution. The dose-response of the parotids is considered to be sigmoidal and thus the Lyman-Kutcher-Burman (LKB) model was used to calculate NTCP. The parameters involved in NTCP calculations using the LKB model are TD 50 , n and m, where TD 50 is that uniform dose which when given to an organ results in 50% complication risk, m is a measure of the slope of the sigmoid curve and n is a parameter which represents the magnitude of the volume effect. [7] Di and vi are quantized points (bins) of the differential DVH of the particular organ. According to the LKB model, [8] NTCP is calculated by the following three equations.
The NTCP parameters used in this study were m = 0.53, n = 1 and TD 50 = 31.4, which yield the NTCP for the specific endpoint of reduction in stimulated salivary flow below 25% within 6 months of RT. They have been selected from a meta-analysis of radiation-induced complications in HN cancers by Semenenko et al. [9] For parallel organs like the parotid glands which have a value of n = 1, the above equation (1) for EUD gets simplified into equation (4) for mean organ dose.
Results Quantitative dosimetric parameters related to target-coverage, homogeneity and organ sparing from the two techniques are presented in [Table - 1] and [Table - 2] . HT plans for all 12 patients showed equivalent or better target coverage and homogeneity, and a significant reduction in OAR doses as compared to SS IMRT plans [Figure - 1]. For PTV66, target coverage achieved by HT was comparable to SS IMRT for most parameters, though HT plans did show significantly improved dose homogeneity (D 10-90, p = 0.002). Among the other parameters related to target coverage, V 99 showed a statistically significant improvement of 13.21% and 10.41% in the HT plans for PTV66 and PTV60 respectively. Parotid sparing was substantially better in the HT plans, with an average reduction of mean parotid dose by 12.66 Gy and 18.28 Gy for the contralateral and ipsilateral glands (p = 0.003) respectively. D 33 and D 66 also showed a considerable and statistically significant reduction for both parotid glands. This translated into a 24.09% and 35.22% reduction in NTCP for the contralateral and ipsilateral parotid glands respectively (p < 0.01). The maximum dose to the spinal cord showed a mean reduction of 12.07Gy in HT plans (p = 0.02). Parotid sparing was also analyzed according to site of primary (oropharynx versus laryngopharynx). The benefit of HT over SS IMRT was similar for both subsites. Discussion HT-generated plans showed superior target coverage, homogeneity and parotid sparing. Though both treatment modalities achieved clinically acceptable treatment plans, HT plans yielded significantly superior sparing for the parotids and the spinal cord. Some parameters were only marginally superior with HT (V 95 , D 1 , D 99 for the target and D 100 for the parotids). Three dosimetric comparisons of linac IMRT (using different treatment planning systems) and HT for HNSCC have been previously published in the indexed medical literature. [10],[11],[12] The first such comparison [12] was reported in five patients with oropharyngeal cancers previously planned with five-field SS IMRT (Plato version 2.6.2) and treated to a dose of 54 Gy in 30 fractions (1.8 Gy/fx) to the elective high-risk volume with SIB to gross disease with margins to 69 Gy in 30 fractions (2.3 Gy/#) using specified dose objective of minimizing doses to the parotids glands without compromising on PTV coverage. For all five patients, HT plans were also generated (field-width 2.5 cm, pitch 0.3, and modulation factor 3) applying the same dose-objectives. All HT plans realized sharper dose-gradients and compared favorably to SS IMRT plans in terms of OAR sparing keeping equivalent target coverage, homogeneity, and tumor control probability. The average reduction in mean parotid dose with HT was 6.5 Gy (range - 4 to 14 Gy, p = 0.0002). The reduction in NTCP in favor of HT was dependant on the parotid model used (-3 to 32%). Sheng et al.[11] compared the two techniques in 10 patients with oropharyngeal carcinoma (five base of tongue and five tonsillar cancers). Each plan was independently optimized using CORVUS treatment planning system with seven-field coplanar arrangement to a dose of 50 Gy in 25 fractions with standard dose-constraints. HT plans were optimized using a field width of 2.5 cm, pitch of 0.3, and nominal modulation factor 2.5. The resulting treatment plans were evaluated by comparing the DVH, EUD, dose uniformity, and NTCP. HT plans showed improvement of critical structure avoidance and target dose uniformity for all patients. The average equivalent uniform dose (EUD) reduction for OARs surrounding base of tongue and tonsil was 17.4% and 27.14% respectively. HT plans achieved 80% reduction in normal tissue complication probability for the parotid glands relative to linac IMRT plans. In a recent report, Fiorino et al. compared linac IMRT technique (inversely optimized on Helios/Eclipse system) against two different HT planning approaches in five patients with advanced HNSCC (10). In the first HT approach (TOMO-a), the dose-constraints used for linac IMRT technique were applied for HT also; in the second approach (TOMO-b), sparing of parotids and mandible was attempted while keeping PTV coverage and spinal cord maximum dose similar to TOMO-a plan. Linac IMRT and HT plans were optimized to deliver 54 Gy in 30 fractions to PTV1 and 16.2 Gy in nine fractions to PTV3; in the case a PTV2 was defined, 15 Gy was concomitantly delivered while delivering 16.2 Gy to PTV3. Separate plans for the two phases (Phase 1 - first 30 fractions; Phase 2- last nine fractions) were compared in terms of DVH and dose statistics on PTVs and OARs. When considering Phase 1, HT improved the homogeneity of the dose distribution within PTV1 while delivering the same prescribed dose (assessed to be the median dose to PTV). The fraction of PTV1 receiving> 95% of the prescribed dose (V95%) increased from 90% (linac IMRT) to 96-97% for HT. Maximum dose within PTV1 decreased from 60.3 Gy (Linac IMRT) to 57.4 Gy (TOMO-a) and 58.7 Gy (TOMO-b). Maximum spinal cord dose decreased from 31.6 Gy (linac IMRT) to 26.5 Gy (TOMO-a) and 24.6 Gy (TOMO-b). Mean dose to the parotids decreased from 26.1 Gy (linac IMRT) to 25.1 Gy (TOMO-a) and 20.8 Gy (TOMO-b). Mandible was also significantly better spared with HT. When considering Phase 2, the average gains (TOMO-b vs. linac IMRT) were more modest and depended on the location of PTV2/PTV3. In the present study, a substantial improvement in parotid sparing was achieved, to some degree, at the cost of target coverage, though it was deemed clinically acceptable and the acceptance criteria for the HT plans was identical to that employed for the SS IMRT plans. Therefore, this improvement could be attributed to the fact that our planning objectives may have differed from other studies, as we put a much larger emphasis on parotid sparing. In our study, the ipsilateral and contralateral parotid glands were considered separately and not as one structure, and a conscious effort was made to spare the contralateral parotid to a greater extent. This was particularly true for SS IMRT planning as seen by the mean parotid doses of 28.8 Gy and 38.8 Gy for the contralateral and ipsilateral parotids respectively. Another area that was not addressed in previous studies was organ sparing according to laterality. We analyzed the parotids as ipsilateral and contralateral to quantify any difference in the degree of sparing between HT and SS IMRT, depending on the side of the disease. The ipsilateral side showed an average reduction in mean parotid dose, of 18.28 Gy compared a mean reduction of 12.66 Gy for the contralateral side. The D 33 and D 66 values showed a similar trend, with a higher magnitude of sparing for the parotid near the high dose region. This suggests that HT could achieve a higher degree of sparing for critical organs abutting the target, due to its capability of producing sharper dose gradients. The site of the disease could also play a role in the degree of parotid sparing. Data was analyzed by site to identify any differences in the degree of parotid sparing. The reduction in parotid dose for the contralateral parotids was similar, regardless of the site. An improvement in parotid sparing was seen for the ipsilateral parotid in the case of laryngopharyngeal tumors as compared to oropharyngeal tumors. The difference did not show statistical significance although it may be clinically relevant. The reduction in parotid gland dose, achieved by HT, was reflected in the significant reduction in NTCP. As a logical sequel to dosimetric promise, clinical outcome data of patients with HNSCC treated on HT has recently started to emerge. In a longitudinal assessment of parotid function using salivary scintigraphy in seven patients treated definitively on HT, Voordeckers et al.[13] observed a significant dose-response relationship between mean parotid dose (< 31 Gy) and salivary function (> 75% recovery). The first single-institution clinical outcome data on 77 consecutive HNSCC patients treated on HT has recently been reported. The two-year estimates of loco-regional control and acute toxicity were very similar to previously published institutional IMRT series. We have also launched a prospective phase II study, which should help validate the results of previous dosimetric studies. This would also help provide baseline data for designing a phase III randomized controlled trial in the future to assess the real clinical benefit with HT. Conclusion Tomotherapy improves dose homogeneity and target coverage as compared to SS IMRT, while significantly improving organ sparing. The magnitude of sparing we could achieve reflected the emphasis put into reducing the dose to the OARs. Whether this translates into a clinical benefit remains to be seen. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10042t2.jpg] [cr10042t1.jpg] [cr10042f1.jpg] |
| |||||||||


![[Table - 1]](/showimage?cr/photo/cr10042t1.jpg){kind=link}
![[Table - 2]](/showimage?cr/photo/cr10042t2.jpg){kind=link}
![[Figure - 1]](/showimage?cr/photo/cr10042f1.jpg){kind=link}