 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
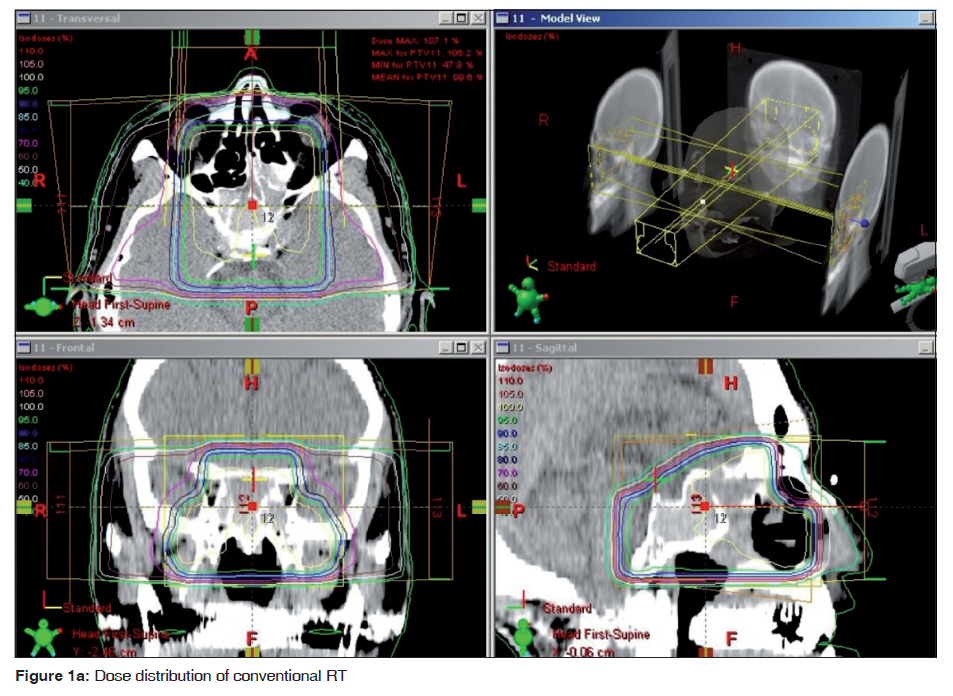
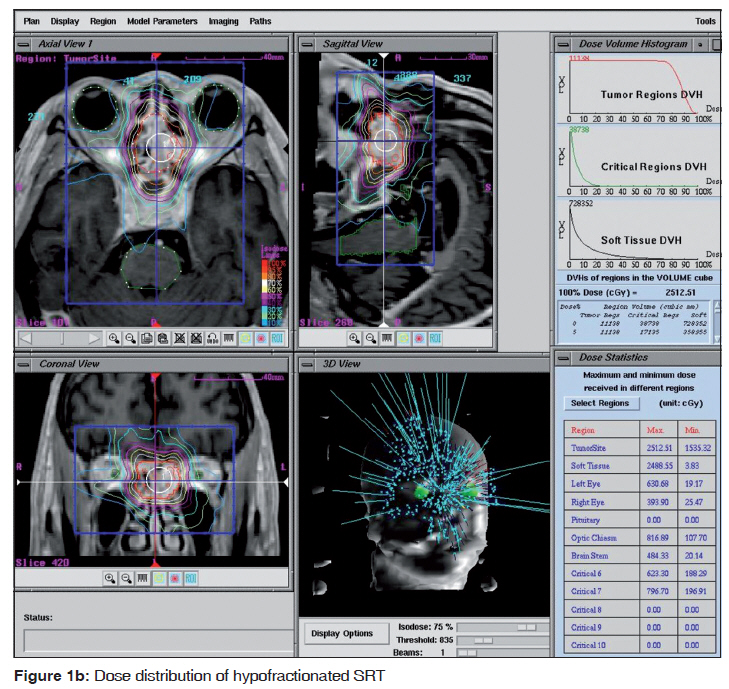
Journal of Cancer Research and Therapeutics, Vol. 6, No. 4, October-December, 2010, pp. 581-584 Case Report Advanced olfactory neuroblastoma treated with combined conventional and hypofractionated stereotactic radiotherapy Satoshi Nomoto1, Yoshiyuki Shioyama2, Saiji Ohga2, Katsumasa Nakamura3, Hiroshi Honda2 1 Department of Radiology, School of Medicine, Fukuoka University, 7-45-1, Nanakuma, Jyonan-ku, Fukuoka, Japan Correspondence Address: Satoshi Nomoto, Department of Radiology, School of Medicine, Fukuoka University, 7-45-1, Nanakuma, Jyonan-ku, Fukuoka 814-0180, Japan, satonomo@fukuoka-u.ac.jp Code Number: cr10145 PMID: 21358109 DOI: 10.4103/0973-1482.77088 Abstract Three patients with olfactory neuroblastoma (ONB) of the nasal and/or paranasal cavity were treated with a combination of conventional radiotherapy (RT) and hypofractionated stereotactic radiation therapy (SRT). Radiation doses of 30 to 50 Gy were delivered in 12 to 25 fractions using conventional RT, and then an additional 20 to 25 Gy was delivered in 5 fractions using SRT. Follow-up time was 42, 53, 65 months, three patients were alive, and local control was obtained in all, complete response (CR) in 2 and partial response (PR) in 1. Two patients had recurrence out of the radiation field and received salvage therapy. According to the Radiation Therapy Oncology Group (RTOG) acute/late radiation morbidity scoring criteria, there were no adverse effects of grade 3 or higher. The combined treatment with conventional RT and hypofractionated SRT achieved excellent local control without serious adverse effects. Keywords: Cyberknife, olfactory neuroblastoma, stereotactic radiotherapy Introduction Olfactory neuroblastoma (ONB) is a rare malignant tumor of the olfactory neuroepithelium in the upper nasal cavity and accounts for 3% of all tumors of the nasal cavity and paranasal sinus. [1] The optimal treatment method remains controversial. Recently, modern radiation therapy techniques have been reported. With the help of these radiation techniques, curative high-dose irradiation of the tumor can be achieved without increasing normal tissue toxicity. [2],[3] Additionally, excellent local control was reported by combining endoscopic surgery and stereotactic radiosurgery (SRS). [4] However, there are few data on clinical outcomes in patients with ONB, undergoing treatment with SRS and stereotactic radiotherapy (SRT). We present a case report of combined conventional RT and hypofractionated SRT for ONB as we experienced excellent local control at the treated site and no serious adverse effects in the long term. Case Report In two male patients and one female patient of age 77, 55 and 53 years, respectively, surgery was not an option because of the local advancement and/or patient refusal. ONB had been pathologically proven in all the patients before their initial treatments. The location of the tumors was from the nasal cavity to paranasal sinuses in two patients, and from the nasal cavity into the anterior cranial fossa in one. All patients were staged in accordance with the Kadish staging system. [5] Detailed information on the patients is shown in [Table - 1]. Conventional RT treatment planning was accomplished using version 7.3.10 of the Eclipse treatment planning system (Varian, Palo Alto, CA, USA). Treatment planning was performed using computed tomographic (CT) scans (slice thickness: 3 mm). The head and neck of each patient were immobilized with a thermoplastic head mask. The clinical target volume (CTV) was defined as the gross tumor volume (GTV) plus a 1 cm margin. The planning target volume (PTV) contained an automated 0.5-1 cm expansion of the CTV to account for immobilization and repositioning accuracy. The covering dose for the isocenter of the PTV was 30-50 Gy and the daily fraction size was 2-2.5 Gy. Hypofractionated SRT treatment planning was accomplished using the CyberKnife-II treatment planning system (Accuray, Sunnyvale, CA, USA). The treatment planning was performed using enhanced-contrast CT scans and gadolinium-enhanced magnetic resonance images (MRI) (slice thickness: 1.3 mm). CT images were integrated to MRIs. The head and neck of each patient were re-immobilized with a thermoplastic head mask on the planning CT after conventional RT. Twenty to 25 Gy was prescribed to the isodose line of D 95% of the PTV and the daily fraction size was 4-5 Gy. The photon energy of 6 MV was used in all. Other structures considered to be critically at risk included the optic chiasm, optic nerve, eyeballs and brainstem. The dose distributions of conventional RT and hypofractionated SRT are shown in [Figure - 1a & b], and the treatment parameters are shown in [Table - 1]. Gadolinium-enhanced MRI has been performed every 3-6 months after radiotherapy. The adverse effects were graded according to the Radiation Therapy Oncology Group (RTOG) acute and late radiation morbidity scoring criteria. Local control for the treated sites was achieved in all: complete response (CR) in two and partial response (PR) in one. Patient 2 experienced metastasis of Rouviere′s lymph node outside the radiation fields at 24 months after radiotherapy. Additional radiotherapy and chemotherapy were performed for the metastasis, and the patient is alive with stable disease. Patient 3 experienced right temporal bone metastasis; additional SRT was performed by CyberKnife-II and the patient is alive. Three patients experienced grade 1 or 2 dermatitis and mucositis in the acute phase. Patient 1 experienced a grade 1 cataract and grade 2 lacrimal duct stenosis 36 months after radiotherapy. Discussion Combined modality therapy with surgery followed by radiotherapy has been generally accepted for the treatment of ONB with radiation doses ranging from 50 to 60 Gy for the tumor sites, using photons. These radiation doses were thought to be insufficient to be curative for ONB; however, the doses did spare the neighboring organ at risk (OAR). Intensity modulated radiation therapy (IMRT) could lead to significant improvements in local control of ONB and adverse effects. Proton-beam therapy (PBT) for ONB resulted in excellent local control with a low incidence of adverse effects. Nishimura et al. reported a 5-year local progression-free survival rate of 84% using 65Gy of total dose with 2.5Gy daily fractionations by PBT alone or combined therapy with surgery or chemotherapy. [3] Resto et al. reported a 5-year local control rate of 69-100% using 71.6 Gy of median total dose with combined proton and photon radiation. [6] The adequate doses for local control of advanced ONB may be more than 70 Gy. Our treatment enables higher tumor doses, good target coverage and spares neighboring OARs. Unger et al. showed that the local control of all the 14 patients with ONB, who were treated with combined endoscopic surgery and SRS, was achieved for 58 months of median follow-up. [4] The single high dose using SRS was adequate for the tumor but exceeded the limits for OAR exposure. The hypofractionated SRT could increase the daily single dose compared to 3D-conformal radiotherapy and deliver less than the fraction dose of SRS. In this study, the biologically effective dose (BED) of combined conventional RT and hypofractionated SRT was 121-130 Gy and 75-88 Gy at alpha/beta ratios of 3 and 10, respectively. When converted to a daily single dose of 2Gy, the total delivery doses were equivalent to 73-78 Gy and 66-73 Gy at alpha/beta ratios of 3 and 10, respectively, according to the linear quadratic model. And this report showed low incidence and grade of acute and late toxicities in long term. The hypofractionated SRT could reduce the irradiated doses to neighboring OARs. Two patients suffered recurrence. The Kadish staging system is demonstrated to correlate with prognosis, and cervical nodal and distant relapse has a significant adverse impact on prognosis. [7] Most patients with locally advanced and recurrent ONB have been treated with a cisplatin-based regimen. [8],[9] Cisplatin-based chemotherapy is generally accepted and considered effective. Because chemotherapy has been an effective treatment for advanced ONB, induction chemotherapy to decrease PTV and irradiated doses of OAR followed by radiotherapy may represent a promising option for locally advanced ONB. We have presented here a case report of ONB treated with combining conventional RT and hypofractionated SRT. References
Copyright 2010 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr10145t1.jpg] [cr10145f1b.jpg] [cr10145f1a.jpg] |
| |||||||||

![[Table - 1]](/showimage?cr/photo/cr10145t1.jpg){kind=link}
{kind=link}
{kind=link}