 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
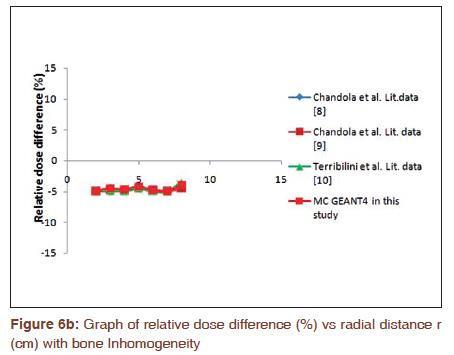
Journal of Cancer Research and Therapeutics, Vol. 7, No. 1, January-March, 2011, pp. 29-34 Original Article Monte Carlo study of dosimetric parameters and dose distribution effect of inhomogeneities and source position of GammaMed Plus source Rakesh M Chandola1, Samit Tiwari2, Nirmal K Painuly3, Vivek Choudhary1, Surendra K Azad1, Manjula Beck1 1 Department of Radiotherapy, Pt. J.N.M. Medical College and Dr. B.R.A.M. Hospital, Raipur, Chhattisgarh, India Correspondence Address: Rakesh M Chandola, Department of Radiotherapy, Pt. J.N.M. Medical College and Dr. B.R.A.M. Hospital, Raipur, Chhattisgarh, India, rakemohachan@rediffmail.com Code Number: cr11007 PMID: 21546739 DOI: 10.4103/0973-1482.80453 Abstract Background: The conventional treatment planning system (TPS) gives analytical calculations with approximately ±15?20% dose uncertainty, which may lead to over exposure of critical organs or under dose of target as well as the presence of inhomogeneities, and the position of source affects the exact dose calculation like in breast and intraluminal brachytherapy.Aim: To obtain dose distribution parameters of GammaMed Plus high dose rate (HDR) 192 Ir source using Monte Carlo (MC) EGSnrc and GEANT4 codes as well as to find the effect on dose distribution due to source position, and due to presence of air and cortical bone by using MC GEANT4 code, and to find the similarity of both studies with any past study of any HDR brachytherapy source for either as input to TPS or verification of TPS calculations. Settings and Design: It is done using different software of the computer, e.g., excel, MS word, etc. Materials and Methods: The source, source position for different studies, water phantom, water characteristics, points of measurements, air and cortical bone inhomogeneities, and position of inhomogeneities were simulated. Statistical Analysis Used: For uncertainties calculation, mean and probability are used. Results: The calculated dose rate constant, radial dose function, and 2D anisotropy function of the source show similarity with published data. Calculated dose distribution differences due to presence of air and cortical bone, and position of source in water phantom also show similarity with published data. Conclusion: These results can either be implemented in TPS or can be used for verification of TPS calculations. Keywords: 2D anisotropy function, dose rate constant, Monte Carlo simulation, radial dose function Introduction Radiation therapy using discrete sources kept in close proximity to the lesion of interest is referred as brachytherapy. The aim of radiotherapy is the maximum dose delivery to the tumor with minimum dose to the surrounding healthy tissues. To achieve this goal, brachytherapy is proved as an effective and popular modality for localized tumors. The main advantage of brachytherapy technique is the high conformal energy deposition in the target volume, and sparing of the organs at risk due to the influence of combination of inverse square law and volume averaging effect on the dose distribution around the source. Monte Carlo (MC) simulation is now becoming an accepted dose calculation methodology in brachytherapy. [1],[2],[3] It is recommended in American Association of Medical Physicists (AAPM) Task Group TG-43U [4] and TG-43U1 [5] state that dose distribution data of the brachytherapy sources in use should be obtained either by experimental measurement or by MC simulation using appropriate code respectively, which then to be used as input data in TPS for planning of exact dose delivery in brachytherapy treatment. The AAPM introduces several dose distribution parameters based on direct dose distribution in water medium. These parameters are: the dose rate constant (∧), the geometry factor G(r,θ), the radial dose function g(r) and the 2D anisotropy function F(r,θ). With the exception of the geometry factor, all others are measured. Moreover, for low energy radioactive sources, e.g., 125 I and 103 Pd seeds. Due to unique character of MC simulation calculations, these calculations give much reliable dosimetric system data to be used in treatment planning of the patient. Meanwhile, considering the patient′s body as a homogeneous water medium, the study of Anagnostopoulos et al.[6] on esophageal brachytherapy shows that if the patient′s inhomogeneities are not taken in to account, the spinal cord dose is overestimated of the order of 13% and sternum dose is underestimated of the order of 15%. Pantelis et al. [7] show that if the source position near or far from the surface of patient is not taken into consideration, the central breast dose is overestimated of the order of 5%, and all other points of the breast is overestimated 10% in HDR brachytherapy of breast. Similarly, the effect of inhomogeneities like cortical bone and air, and source position on dose distribution is done by Chandola et al. [8],[9] and Terribilini et al. [10] Apart from radiation−tissue interaction study, MC simulation is used to solve various physical problems. MC simulation calculations are based on random sampling techniques and are capable to collect the information based on large number of histories. [11] In this study, the MC technique is used to calculate the dosimetric parameters of GammaMed Plus HDR 192 Ir source and also MC simulations have been employed to investigate the effect on dose distribution due to source position, and presence of air and cortical bone. Finally, the authors compared the calculated results by the previous published data. Materials and Methods The GammaMed Plus 192 Ir brachytherapy source geometric design is derived here from Ballester et al. [12] and is illustrated in [Figure - 1]. The active core material composition of the source is of 70% Ir and 30% Pt with an effective density of 21.76 g/cm 3 . It has 3.5 mm active length with active diameter of 0.60 mm. The active core remains covered by the stainless steel AISI 316L capsule of density 8.06 g/cm 3 . The lateral and top sides of the active core are hollow. The inner and outer diameters of stainless steel encapsulation are 0.07 and 0.09 cm, respectively. The tip of the encapsulation is a conical section with an opening angle of 68°. The tip of the source with conical shape was simulated as three cylindrical slices of thicknesses 0.005, 0.005, and 0.006 cm with corresponding radii of 0.012, 0.03, and 0.035 cm, respectively. The distance of the tip from the active end of the source is 0.62 mm leading to total length of the source of 4.52 mm. In this study, the cable made of stainless steel AISI 304 of density 5.6 g/cm 3 and of length 6 cm are also MC simulated. In this study, the MC simulation of source position, water phantom and its water, applicator, points of calculation, and inhomogeneities were done considering the set up of the experimental or measured study. The source was modeled inside the applicator and at the centre of said water phantom along Z-axis with the tip of the source toward +Z axis. The centre of the source acting as the centre of the co-ordinate axes and the points of measurement were modeled at different positions. For radial dose function study, the points of calculation were modeled at the transverse axis of the source from 1 to 12 cm. The value obtained at different points were made normalized to the value obtained at 1 cm. While for 2D anisotropy function study, the points of calculation were modeled at fixed radial distance of 5 cm and polar angles of θ = 0° to 178° with a sector angle of 10° between them. The value obtained at different polar coordinates were made normalized to the value obtained at polar coordinates (r = 5 cm, θ = 90°). To obtain the dose rate in Cartesian co-ordinates D(X,Y) a grid system having 0.04 cm thick and 0.04 cm high cylindrical rings concentric to the longitudinal axis of the source have been simulated for MC calculation of dose distribution parameters. The applicator modeled was made of stainless steel 1.4401 (equivalent to AISI/SAE 316) of density of 8.0 g/cm 3 with wall thickness of 0.15 mm and with inner and outer diameters of 1.35 ± 0.02 mm. and 1.65 ± 0.02 mm, respectively. The value of effective attenuation coefficient was taken as 0.030 ± 0.002 (ANSI 303/304). [13] The unit of the effective attenuation coefficient was taken as cm 2 /g. As the source diameter is 0.9 mm, which means that source could be displaced maximum of ± 0.22 mm from the central axis of the applicator. Therefore, the uncertainty in positioning source inside the centre of the applicator is also considered here during dose parameters calculations. The water phantom modeled was of dimension 30 × 30 × 30 cm 3 that acts as an unbounded phantom up to 20 cm of radial distance. [14] The density of the water used in the simulation was 0.997 g/cm 3 at 22 °C, as is recommended in TG-43U1. [4],[5] For inhomogeneities effect study on dose distribution, the inhomogeneities air and cortical bone MC simulated were having the composition as recommended in TG-43U1 with 40% relative humidity, and by International Commission of Radiological Protection (ICRP), respectively. The volume of each inhomogeneity was 1 × 2 × 2 cm 3 placed at 1 cm from the centre of source at transverse axis (X-axis) of the source as illustrated in [Figure - 2]. For study of source position effect on dose distribution, the source was simulated at 1 cm from the surface of water phantom with the tip of the source along +Z-axis, and with the center of source as the center of coordinate axes as shown in [Figure - 3]. The gamma spectrum of the 192 Ir HDR radioactive source used in this study has been obtained from NuDat database. [15] The gamma rays have been simulated considering that 192 Ir is uniformly distributed in the source core. The beta spectrum has not been considered in simulation since it′s contribution to the dose rate distribution for distances greater than 1 mm from the source is negligible due to the encapsulation of the source and the catheter in which the source is introduced. [16] However, the models for the processes of Compton scattering, Photoelectric effect and Rayleigh scattering have been used simulated in the low energy package of EGSnrc. The cross-section tabulation with uncertainty was taken from the EPDL 97. [17] The air kerma strength, S k, was calculated in a separate simulation of 10 8 histories. The source was positioned at the centre of an air volume of 4 × 4 × 4 m 3 with a composition and density as recommended in TG-43U1 of air of 40% relative humidity. It was calculated along the transverse axis of the source from 0 to 150 cm using 1 × 1 cm cylindrical voxels/cells. This configuration was chosen in order to simulate a real experimental measurement with a therapy level detector calibrated in water. These scoring voxels/cells assure volume averaging artifacts <0.1% for distances greater than 5 mm from the source. [18] The scored energy in water was converted to air kerma by multiplication of the ratio of mass attenuation coefficients of air and water. Air attenuation and scattering was corrected with the factor 1.012. [19],[20] About 10 8 histories are traced here to perform the simulation for evaluation of the effects of inhomogeneities and position of source in water phantom on dose distribution. The energy scored was taken to be in cubiodal 2 × 2 × 2 cm 3 scoring voxels, as very small voxels increases the uncertainty and as the rotational symmetry around the source axis is discontinued by inclusion of dry air and cortical bone inhomogeneities and by placing the source very near to the surface of water phantom. Results MC calculated dose rate constant reported here 1.109 ± 0.033 cGy h -1 U -1 using MC GEANT4 code and 1.116 ± 0.033 cGy h -1 U -1 using EGSnrc code. Both dose rate constants agree within relative differences of 0.81% and 0.18%, respectively, with literature value of 1.118 003 of Ballester et al.[12] The radial dose functions of said source are presented in [Table - 1] and their graphs are illustrated in [Figure - 4]. Both MC calculated radial dose functions show similar nature and also have the similarity with literature study. [12] The 2D anisotropy functions (r = 5 cm) of said source are presented in [Table - 2] and their graphs are illustrated in [Figure - 5]. Both MC calculated 2D anisotropy function also show similarity with each other and with literature data. [12] The percentage relative difference between dose in presence of air and cortical bone inhomogeneties and dose in absence of respected inhomogeneity is shown in [Table - 3] and illustrated in [Figure - 6](a) and (b), respectively. Behind air inhomogeneity, the dose was found to be increased by 5.35 to 7%, and behind cortical bone, the dose was found decreased by 4.22%−4.81%. These results are found in good agreement with literature data. [8],[9],[10] [Table - 4] and [Figure - 7] illustrates the data and graph between the ratio of the dose (D1 ) when the source was at 1 cm distance from the surface of water phantom to the dose (Dc) when the source was at center of water phantom vs radial distance. The results show that the near points between 1 and 2 cm from the source were 2.2%−3.6% underdose and the far points more than 3 were 5.7%−16.3% underdose. These results also show similarity with literature data. [8],[9],[10] Discussion Each dose parameter measurement is subjected to some uncertainty estimated 5% for S k, ∧, F(r, θ) and g(r). [5] In this calculated study, the uncertainties of dose rate have been evaluated according to the recommendations of TG-43U1 considering the type A or statistical uncertainty due to the MC simulation of photon histories in dose rate and air kerma strength simulation and the type B uncertainty due to the contribution of underlying cross section data and that arising from the source geometrical model. In the simulation in water, the uncertainty in dose rate along the transverse axis is approximately equal to 0.5 % except along the longitudinal axis where it has reached to more or less 1%. For the simulation of the air kerma strength, the uncertainty is more or less 0.5%. Thus, the maximum type A uncertainty in calculated study may be taken as 1.5% for all points. To estimate the uncertainty due to the variations of the geometry from one source to another in the manufacturing process, the uncertainty is evaluated keeping the worst possible situation for the core and capsule dimensions of the source. First, the thinner capsule and thickest core possible, and second, the thicker capsule and thinner core possible are assumed here. The MC calculations showed that 0.5% variation is to be considered compared to the case of normal dimension source. The MC EGSnrc and GEANT4 calculated radial dose functions show very good agreement for distances up to 5 cm with literature data. [12] For distances greater than 5 cm, the relative difference between both calculated data and literature data [12] are slightly larger, which may be due to different uncertainties and effect of size of water phantom. The MC calculated 2D anisotropy functions show fair agreement with literature data [12] for polar angles 20 0 < θ < 160 0 . However, at angles θ < 20 0 and θ > 160 0 deviations are larger, which may be due to uncertainties, volumetric averaging effect, and due to the cause that in these two regions very small voxel/cell sizes were chosen to have high resolution for dosimetric parameters calculation, which may have increased the statistical uncertainty. For study of effects of air and cortical bone inhomogeneities on dose distribution, the deposited energy was determined by using 10 9 histories in simulation, which yielded 0.2% near the source and 0.5% for distances greater than 4 cm from the source. Behind air inhomogeneity, the dose was increased, which may be due to decreased attenuation of radiation, and its less density. However, behind cortical bone inhomogeneity, the dose was decreased, which may be due to increased attenuation of radiation, and its high density. When the source is placed very near to surface of water phantom, the different distant points get less dose, which may be due to lack of backscattering material. However, the nearer points go less underdose than the more distant points, which may be due to the cause that the primary dose may overlap missing scatter function for near points from the source. Conclusion The results show that there is a strong correlation ship between both MC calculated dosimetric parameters and with previous study. Similarly, the MC calculated dose differences due to presence of air and cortical bone inhomogeneities, and MC calculated dose difference due to source position also have similarity with the past studies. Therefore, this study results can be used either as input data in TPS or to verify the calculations of TPS for exact brachytherapy treatment planning. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11007f6a.jpg] [cr11007f5.jpg] [cr11007f3.jpg] [cr11007t1.jpg] [cr11007f4.jpg] [cr11007t4.jpg] [cr11007t2.jpg] [cr11007f2.jpg] [cr11007t3.jpg] [cr11007f7.jpg] [cr11007f1.jpg] [cr11007f6b.jpg] |
| |||||||||

![[Figure - 1]](/showimage?cr/photo/cr11007f1.jpg){kind=link}
![[Figure - 2]](/showimage?cr/photo/cr11007f2.jpg){kind=link}
![[Figure - 3]](/showimage?cr/photo/cr11007f3.jpg){kind=link}
![[Table - 1]](/showimage?cr/photo/cr11007t1.jpg){kind=link}
![[Figure - 4]](/showimage?cr/photo/cr11007f4.jpg){kind=link}
![[Table - 2]](/showimage?cr/photo/cr11007t2.jpg){kind=link}
![[Figure - 5]](/showimage?cr/photo/cr11007f5.jpg){kind=link}
![[Table - 3]](/showimage?cr/photo/cr11007t3.jpg){kind=link}
](/showimage?cr/photo/cr11007f6a.jpg){kind=link}
{kind=link}
![[Table - 4]](/showimage?cr/photo/cr11007t4.jpg){kind=link}
![[Figure - 7]](/showimage?cr/photo/cr11007f7.jpg){kind=link}