 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
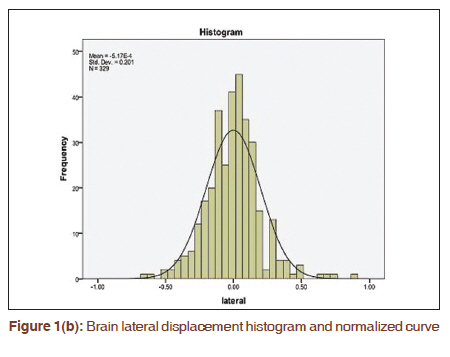
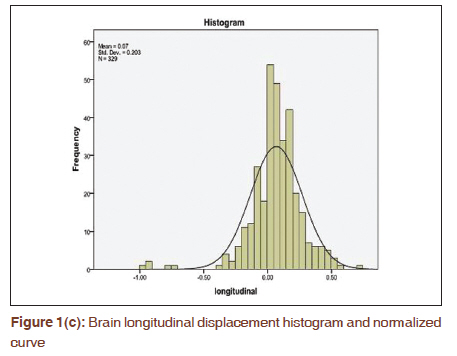
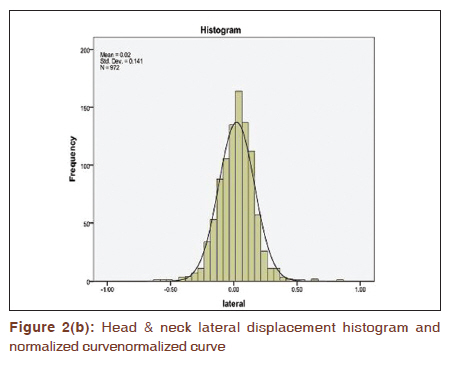
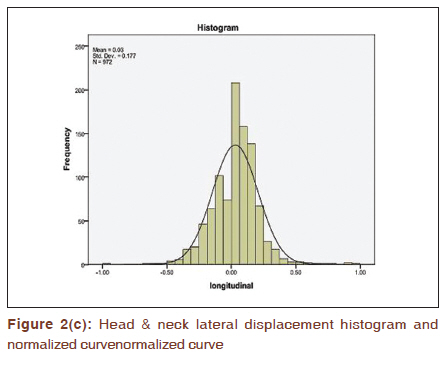
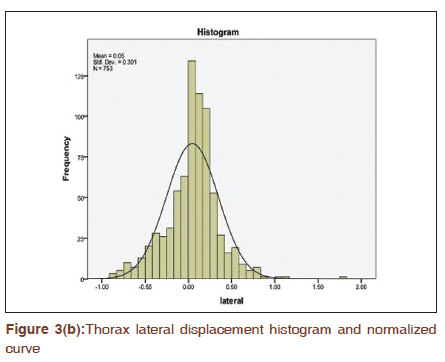
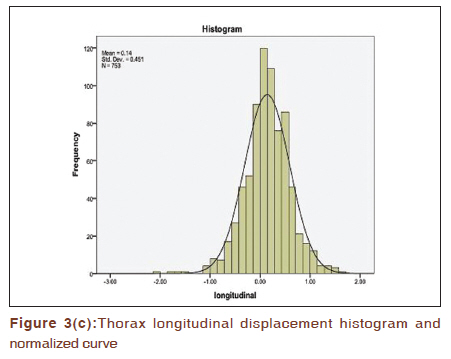
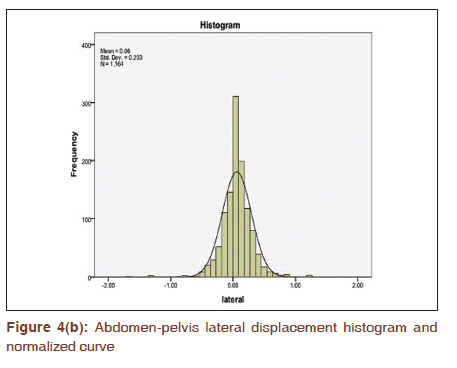
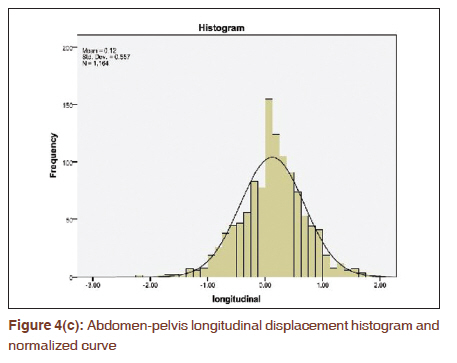
Journal of Cancer Research and Therapeutics, Vol. 7, No. 1, January-March, 2011, pp. 40-46 Original Article Set-up uncertainties: Online correction with X-ray volume imaging Tejinder Kataria, Ashu Abhishek, Pranav Chadha, Janardhan Nandigam Division of Radiation Oncology, Medanta Cancer Institute, Medanta-The Medicity, Sector-38, Gurgaon, Haryana-122 001, India Correspondence Address: Tejinder Kataria, Division of Radiation Oncology, Medanta Cancer Institute, Medanta-The Medicity, Sector-38, Gurgaon, Haryana-122 001, India, teji1960@gmail.com Code Number: cr11009 PMID: 21546741 DOI: 10.4103/0973-1482.80457 Abstract Aim: To determine interfractional three-dimensional set-up errors using X-ray volumetric imaging (XVI).Materials and Methods: Between December 2007 and August 2009, 125 patients were taken up for image-guided radiotherapy using online XVI. After matching of reference and acquired volume view images, set-up errors in three translation directions were recorded and corrected online before treatment each day. Mean displacements, population systematic (Σ), and random (σ) errors were calculated and analyzed using SPSS (v16) software. Optimum clinical target volume (CTV) to planning target volume (PTV) margin was calculated using Van Herk's (2.5Σ + 0.7 σ) and Stroom's (2Σ + 0.7 σ) formula. Results: Patients were grouped in 4 cohorts, namely brain, head and neck, thorax, and abdomen-pelvis. The mean vector displacement recorded were 0.18 cm, 0.15 cm, 0.36 cm, and 0.35 cm for brain, head and neck, thorax, and abdomen-pelvis, respectively. Analysis of individual mean set-up errors revealed good agreement with the proposed 0.3 cm isotropic margins for brain and 0.5 cm isotropic margins for head-neck. Similarly, 0.5 cm circumferential and 1 cm craniocaudal proposed margins were in agreement with thorax and abdomen-pelvic cases. Conclusion: The calculated mean displacements were well within CTV-PTV margin estimates of Van Herk (90% population coverage to minimum 95% prescribed dose) and Stroom (99% target volume coverage by 95% prescribed dose). Employing these individualized margins in a particular cohort ensure comparable target coverage as described in literature, which is further improved if XVI-aided set-up error detection and correction is used before treatment. Keywords: Mean displacement, random error, set-up errors, systematic error, X-ray volumetric imaging Introduction Geometric uncertainties in radiotherapy are a well-known fact and substantial data, information, and knowledge have accumulated in the last decade on this subject. [1] Set-up errors, a component of uncertainties, are inherent in the radiation treatment process and there exists a difference in the actual vs the intended position of the patient. The set-up errors can be mathematically divided into random and systematic errors. The systematic errors represent the deviations that are same for each fraction of the treatment, and random variations vary on day-to-day basis. Coverage of target volume is a direct function of set-up margins, which should be optimized to prevent inadvertent irradiation of adjacent normal tissues. Planning target volume (PTV) that encompasses the clinical target volume (CTV) with some margins to account for such uncertainties in patient positioning, organ motion, and beam geometry is universally accepted today as the benchmark for radiation dose prescription. [2],[3] The increasing use of intensity-modulated radiotherapy (IMRT) inherent with steep dose gradients makes it vital to detect, quantify, and to correct these errors. In addition, dose constraints used in inverse planning of IMRT are based on organs derived from treatment planning scan, implying that any variation in organ volume or position during treatment delivery may significantly alter the dose delivered to both the target and surrounding normal tissue to an even greater extent than analogous changes occurring during conformal treatment delivery. The measurement of position and shape of soft-tissue target structures at the point of treatment delivery has been the subject of study by a number of investigators. [4] This technology has progressed considerably but is fundamentally limited by detector sensitivity, which means imaging doses are as high as 5% of the fraction dose and the inherent inability of megavoltage X-rays to discriminate the contrast due to density differences between soft-tissue structures such as muscle and fat. [5] Jaffray et al., Siewerdsen et al., and Groh et al. mounted a kilovoltage source, with an opposed amorphous silicon flat-panel detector onto the gantry of a treatment linear accelerator. [6],[7],[8],[9],[10] Rotation of the kilovoltage source around the patient allows acquisition of a series of images that can be reconstructed to provide three-dimensional (3D) volumetric data. Phantom and animal studies suggest that soft-tissue contrast is achievable with this system using reduced doses as low as to 0.01 to 0.03 Gy. [10] This technology therefore provides the means to acquire 3D X-ray volumetric imaging (XVI), with soft-tissue definition, of patients on the radiotherapy couch at the time of treatment delivery. It has immense potential both to revolutionize treatment verification, ensuring accurate treatment delivery, and facilitate new methods of radiotherapy treatment planning and delivery using image-guided radiotherapy (IGRT). The present prospective study was aimed at determining the set-up errors/uncertainties utilizing the process and utility of XVI, including the dose delivered. Materials and Methods Study Design The present study was planned to determine the set-up errors for CTV-PTV for different anatomical sites employing a kilovoltage Cone beam computed tomographic scanner (kv-CBCT) inbuilt within the linear accelerator and to judge the feasibility of the process workflow. Online set-up errors were determined and rectifications made accordingly on a daily basis prior to treatment. Patient characteristics Between December 2007 and November 2008, 125 patients of tumor locations confined to 4 different anatomical regions of the body, namely brain, head and neck, thorax, and abdomen, were treated by IGRT [Table - 1]. Equipment and process 3D reference data of each patient were imported from the Precise-Plan TM Treatment Planning System (Elekta, Crawley, UK) through DICOM to Synergy-S TM Linear Accelerator (Elekta, Crawley, UK) console. Patient was positioned for treatment in the same position as on the day for planning CT image acquisition matching the set-up fiducials. X-ray volume image was acquired for each patient everyday by a full 360 o rotation, requiring 3 to 5 minutes for complete acquisition. The acquisition time averaged 2 to 3 minutes with a radiation dose of 8 to 16 mGy, depending on site being treated. A 3D Volume View TM reconstruction was obtained and matched to the individual reference CT images in the "grey value" mode. An automatic match for the tissue densities in reference images with that of the acquired images was carried out. The translational errors thus obtained after an automatic match were calculated and these errors were converted to couch correction in lateral, longitudinal, and vertical directions. Patients were treated after couch repositioning, if required, based on couch correction procured. Set-up errors obtained for each patient, daily in all three translational directions, were tabulated and mean error calculated for each. Mean errors with standard deviation, along with systematic and random errors, were thus obtained for each subgroup. Statistical Methods Margins generated from the recipes of Stroom and Van Herk were compared for the set of patients and then each subset. Percentage of patient-generated CTV-PTV margins within the Van Herk and Stroom′s margins was calculated. Systematic errors were the standard deviation of mean errors as calculated for each patient in various sub groups. Random errors were the root mean square values of the standard deviation of errors recorded in all three directions for each patient in a sub group. Results A total of 125 patients were sub grouped into tumors of brain, head and neck, thorax, and abdomen-pelvis, consisting of 13, 37, 32, and 43 patients, respectively [Table - 1]. The total number of 9 653 set-up errors was noted for entire cohort. The errors for individual cohort were 987 for brain, 2 915 for head and neck, 2 259 for thorax, and 3 492 for abdomen-pelvis [Table - 2]. [Table - 3] shows mean set-up errors in all the three directions for various sub-cohorts. For cases with brain tumor, the mean errors noted were 0.14 ± 0.08 cm in lateral dimension, 0.15 ± 0.05 cm in longitudinal dimension, and 0.11 ± 0.02 cm in vertical dimension. For head and neck cases, mean errors were 0.12 ± 0.05 cm laterally, 0.12 ± 0.04 cm longitudinally, and 0.12 ± 0.05 cm vertically. For thorax cases, mean set-up errors were 0.29 ± 0.11 cm laterally, 0.43 ± 0.20 cm longitudinally, and 0.22 ± 0.10 cm in vertical direction; whereas for the abdomen-pelvis sub-cohort, the mean set-up errors were 0.19 ± 0.06 cm laterally, 0.46 ± 0.15 cm longitudinally, and 0.20 ± 0.09 cm in the vertical direction. [Table - 4] shows systematic and random errors as calculated from the individual errors documented for all 125 patients. [Figure - 1]a, b ,c [Figure - 2]a, b, c, [Figure - 3]a, b, c and [Figure - 4]a, b, c depict mean errors as recorded in various sub-cohorts of patients in lateral, longitudinal, and vertical directions. [Figure - 5] shows the maximum set-up errors as recorded in various directions for each cohort of the patients. The mean vector displacement recorded were 0.18 cm in the brain, 0.15 cm in head and neck, 0.36 cm in thorax, and 0.35 cm in abdomen-pelvis sub-cohort. Stroom′s margins in anteroposterior (AP), mediolateral (ML), and superoinferior (SI) directions were calculated for brain (0.34 cm [AP], 0.36 cm [ML], 0.31 [SI]), head-neck (0.23 cm [AP], 0.25 cm [ML], 0.31 cm [SI]) thorax (0.48 cm [AP], 0.57 cm [ML], 0.76 cm [SI]), and abdomen-pelvis (0.39 cm [AP], 0.35 cm [ML], 0.94 cm [SI]) [Table - 5]. Similarly, Van Herk′s margins were calculated for brain (0.40 cm [AP], 0.42 cm [ML], 0.35 cm [SI]), head-neck (0.26 cm [AP], 0.30 cm [ML], 0.36 cm [SI]), thorax (0.57 cm [AP], 0.66 cm [ML], 0.87 cm [SI]), and abdomen-pelvis (0.46 cm [AP], 0.40 cm [ML], 1.09 cm [SI]) [Table - 5] Analysis of individual mean set-up errors revealed good agreement with the proposed 0.3 cm isotropic margins for brain (100% cases ≤0.30 cm [AP], 100%≤0.18 cm [ML], 100%≤0.21 cm [SI]), and 0.5 cm isotropic margins for head-neck (97.3% cases ≤0.20 cm [AP], 100% ≤0.20 cm [ML], 100% ≤0.24 cm [SI]). Similarly, 0.5 cm circumferential and 1 cm craniocaudal proposed margins were in agreement with thorax (100% cases ≤0.37 cm [AP], 100% ≤0.45 cm [ML], 100% ≤0.59 cm [SI]) and abdomen-pelvic cases (97.7% cases ≤0.28 cm [AP], 100% ≤0.26 cm [ML], 97.7% ≤0.58 cm [SI]) [Table - 6]. Discussion The existence and effects of set-up uncertainties on final dose delivery has long been known to all radiation oncologists. Various groups have studied these errors in detail to estimate the exact magnitude, factors responsible, methods for reduction of these errors, and the requirement for a PTV that is responsible to provide extra margins to the final target volume to ensure no target volume miss during radiation delivery due to the daily unavoidable set-up errors. Errors that result in geographical miss of target volume may occur at any step from initial patient immobilization to final set-up before treatment delivery. Although errors in estimation of gross tumor volume may significantly alter the dose to the final intended tumor volume, these errors may be controlled and minimized, using better imaging tools. [11] Set-up uncertainties, being unavoidable and directly influencing the CTV-PTV margin, play a major role in decision of the final volume to be irradiated for adequate coverage of the intended target. Various margin recipes have been documented in literature. These margins differ depending on the proposed population coverage, different target volume coverage possible and also varied contribution of the systematic and random errors in patient set-up. Most published margin recipes ignore the importance of simultaneous contribution of both systematic (preparation) and random (execution) errors to the final PTV margin. Usually, systematic errors are specific for a subset of patients in a particular institution and thus will not differ through the course of the therapy for a patient. On the other hand, random errors keep changing for every fraction. It is thus evident that both the errors are responsible for the final set-up error and with a bigger contribution from systematic and a smaller contribution of random errors to the final calculated set-up error. Therefore, among the various margin recipes from the literature, those of Van Herk′s and Stroom′s have been used widely and with greater acceptance. Van Herk′s and Stroom′s margin estimates are based on varying contribution of systematic error (SE) and random errors (RE) depending on percentage population, CTV, or dose level coverage. As per Van Herk′s estimate, contribution of systematic errors determine population coverage and thus 2.16 Σ, 2.31 Σ, 2.50 Σ, 2.79 Σ, and 3.36 Σ is required for 80%, 85%, 90%, 95%, and 99% population coverage, respectively. Similarly, linear addition of varied contribution of random errors will result in different dose level coverage, e.g., 0.4 σ (80% dose level), 0.5 σ (85%), 0.6 σ (90%), 0.7 σ (95%), and 0.95 σ (99%). Thus, the commonly used CTV-PTV margin estimate of 2.50 Σ + 0.7 σ ensures 90% population coverage for 95% prescribed dose. Similar estimates of Stroom ensure percentage coverage of CTV volume by a particular dose and thus 2Σ + 0.7 σ recipe of Stroom aims at coverage of 99% of CTV volume by 95% of the prescribed dose. Among the various methods of estimation of 3D set-up errors, X-ray volume imaging using kVCT has shown better acceptance with freedom of daily usage considering low dose delivered per fraction as compared with the available port films and megavoltage CT (MVCT). We have presented only translational set-up errors as our Hexapod system had not been installed at the time of the study. Within this study, we established and validated the 3D volume imaging of an on-board cone-beam CT scanner for the evaluation of set-up errors. Our study has limitations in several aspects. Most notably, we only corrected for shifts in the translational dimensions, not in rotational space. Although this was not an ideal optimization given the inability to correct in all six dimensions, we were limited by the registration algorithm to correct solely in translational space. Guckenberger et al. suggested that rotational shifts could result in significant dose shifts in selected patients. Hanley et al. reported that out-of plane rotations of ≥2 o introduced significant errors to two-dimensional image registration and had dosimetric consequences. [12],[13] Kim et al. showed that when rotational displacement was unadjusted, dose-volume histogram analysis demonstrated an increase in the dose to the spinal cord dose (6.4%) and contralateral parotid (2.7%). [14] Our results are in agreement with the published data on set-up errors in various sites and are also explained by the anatomical differences in body structure and rigidity and type of immobilization methods currently being used. Set-up uncertainties as expected are lesser in brain and head-neck cases as compared with thorax and abdomen due to possible minimal daily changes due to respiratory movement and effect of varying daily nutrition and hydration on body shape. Moreover, errors recorded in longitudinal direction in a subset of patients are more as compared with lateral and vertical direction, as explained by the present day immobilization casts that are open at both ends, craniocaudally allowing possible translation and rotational movement of the patient in longitudinal direction. Although possible to minimize these displacements, it is important to understand that residual errors remain with daily variation even after rigid immobilization. Using XVI to determine these uncertainties helps in determining individual PTV margins required to adequately negate the effects of these daily variations. Although XVI helps in precise estimation of set-up errors in a sub-group of patients and subsequent calculation of adequate PTV margins, whether it can be used to reduce the PTV margins still needs to be answered. Theoretically, it may be possible as the daily set-up error recorded are also corrected before treatment as per the online error estimation and correction protocol of XVI. Although residual errors remain even after table correction, they are lesser than initial error recorded for the day before correction. This can be commented with confidence only if XVI is done initially before set-up error estimation and then after table correction to determine residual error. The residual errors once estimated can be used to calculate the new PTV margins, and the difference thus may indicate the reduction in existing PTV margins that may be possible in particular cohort of patients. Conclusions Within this study, we established the kv-CBCT for the evaluation of set-up errors and the feasibility of its use in day-to-day clinical practice. kv-CBCT also acts as a tool to further reduce the CTV-PTV margins if daily online correction and determination of residual errors are made. The next steps at our institute will be the correction of both translational and rotational setup errors using the Hexapod treatment couch. Acknowledgments The authors wish to acknowledge the compassion and dedication of the paramedical staff and all radiation technologists in assisting with the completion of this study. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11009f4b.jpg] [cr11009f3a.jpg] [cr11009f3c.jpg] [cr11009t3.jpg] [cr11009f2c.jpg] [cr11009f2b.jpg] [cr11009f1a.jpg] [cr11009f4a.jpg] [cr11009t2.jpg] [cr11009f2a.jpg] [cr11009f3b.jpg] [cr11009t4.jpg] [cr11009f5.jpg] [cr11009t5.jpg] [cr11009t6.jpg] [cr11009f4c.jpg] [cr11009f1b.jpg] [cr11009t1.jpg] [cr11009f1c.jpg] |
| |||||||||

![[Table - 1]](/showimage?cr/photo/cr11009t1.jpg){kind=link}
![[Table - 2]](/showimage?cr/photo/cr11009t2.jpg){kind=link}
![[Table - 3]](/showimage?cr/photo/cr11009t3.jpg){kind=link}
![[Table - 4]](/showimage?cr/photo/cr11009t4.jpg){kind=link}
![[Figure - 1]a](/showimage?cr/photo/cr11009f1a.jpg){kind=link}
{kind=link}
{kind=link}
![[Figure - 2]a](/showimage?cr/photo/cr11009f2a.jpg){kind=link}
{kind=link}
{kind=link}
![[Figure - 3]a](/showimage?cr/photo/cr11009f3a.jpg){kind=link}
{kind=link}
{kind=link}
![[Figure - 4]a](/showimage?cr/photo/cr11009f4a.jpg){kind=link}
{kind=link}
{kind=link}
![[Figure - 5]](/showimage?cr/photo/cr11009f5.jpg){kind=link}
![[Table - 5]](/showimage?cr/photo/cr11009t5.jpg){kind=link}
![[Table - 6]](/showimage?cr/photo/cr11009t6.jpg){kind=link}