 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 264-269 Review Article Chemotherapy, neurotoxicity, and cognitive changes in breast cancer Varsha Dutta Department of Radiation Oncology, ACRO, Dr. Balabhai Nanavati Hospital, S.V. Road, Vile Parle (W), Mumbai - 400 056, India Keywords: Breast cancer, chemotherapy, neurotoxicity, chemofog, frontostriatal dysfunction
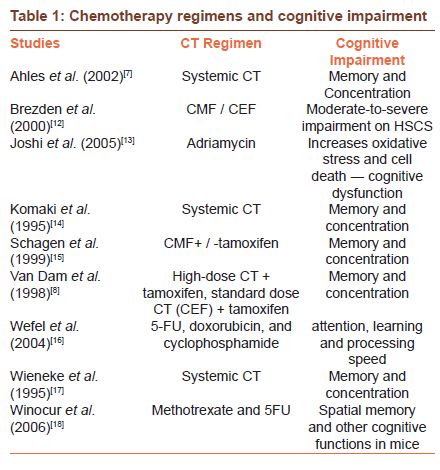
In the last few years, especially since the past decade, neurotoxicity related to the chemotherapeutic regimen has come under immense scrutiny. Witnessed in many forms, it has been authenticated by neuropsychological tests, which have been confirming the fears of most of the patients who have often complained of cognitive changes following chemotherapy. At present, the perseverant but unfortunate term ′chemobrain′ or ′chemofog′ finds itself unavoidably attached to it. Substantial literature reviews have been documenting this mutual predicament between chemotherapy and neurotoxicity, probing the assorted attributes of this complex neuropsychological manifestation in clinical populations undergoing distinctive therapies. Clinically, this mild cognitive impairment is being documented in patients with breast cancer undergoing adjuvant chemotherapy. Some of the commonly reported problems are difficulties with concentration, short-term memory, and planning. The improved life expectancy in cancer patients in the last 30 years has been attributed to the newer chemotherapeutic regimens that have minimized the risk patterns for recurrence and improved the survival rates in this group. Luckily, for most women undergoing therapy for breast cancer, a timely diagnosis and much-needed surgery along with adjuvant therapy have worked together in their favor. Most patients survive for decades following treatment and at present an increasing number of people have begun to complain of cognitive problems, which they associate with a "vague form of cloudiness that often comes in the way of daily planning of even routine chores" (patient′s account). These are the neurotoxic effects rendered by chemotherapeutic regimens that were sidelined as the inevitable consequences of a life-threatening condition. Newer research inquests are vehemently pointing toward the severity of these regimens, which begin early in the stage of treatment and then subsequently heighten to progression. It becomes imperative that such escalating risk factors are addressed and the associated symptoms identified early on. Extensive literature now surrounds this domain, with most research speculating about the quantitative aspects of the phenomenon. On inquiring, unavoidable methodological reservations accompany each practitioner from their chosen field of expertise. This inevitably clouds the full appreciation of the problem, as most of its contributory aspects then cannot be adeptly linked. Bearing this in mind, I have in this commentary, tried to focus on some of the select views that potentiate the need to accrue sound methodological reserves, while following the course and progression of chemotherapy. Chemotherapy-Induced Cognitive Changes Self-reported problems of cognitive decline are intricately linked with psychological stress, fatigue, and anxiety related to the diagnosis of breast cancer. [1],[2] Therefore, most times these perceived symptoms outweigh what can actually be assessed neuropsychologically. [1],[2] On studying the long-term toxicity effects on cognition and other functions, it becomes important to first examine the relation between the patient′s subjective perception of her cognitive loss and the objective scores received through neuropsychological testing. Most studies have shown a positive correlation between the two, but when controlled for depression, anxiety, and fatigue the correlation has often weakened. [3] Poeppelreuter and colleagues, [4] in their study, described a significant relation between self-perceived cognitive loss and objective scores on the tasks of learning and memory (P < 0.05) and mental flexibility (P < 0.01), in a sample of 119 breast cancer patients; but when the same was controlled for the affective variables that could have influenced the cognitive decline the correlation weakened. A similar study design was incorporated by Bender et al.[3] in 31 women with early-stage breast cancer (I / II). The women were also on hormonal therapy, which they received at an average of 19.9 months during the time of neuropsychological testing. The design incorporated was cross-sectional and controlled for affective variables like the previous study. A positive correlation was shown between the patient′s perceived cognitive deterioration and the objective test measures on verbal learning and memory, while the reverse was observed when the test scores on visual memory tasks, attention, and memory flexibility were correlated with perceived cognitive abilities. However, Castellion and group [5] found a significant relation between perceived scores on the cognitive failure questionnaire (CFQ) and the objective test scores on the visuospatial tasks, leaving only the other cognitive domains intact. Even as the studies by Poppelreuter and group [4] and Bender et al. [3] have shown poor performances in learning and verbal memory tasks, the reverse was seen in Castellion′s study. [5] To date, most studies have reported a mixed diffuse cognitive pattern in neuropsychological testing, with the majority accentuating compromised functioning in verbal learning and memory, and attention and concentration, underscoring a frontostriatal dysfunction. [3],[4],[6] Direct dose-dependent effects of chemotherapy on cognitive performance have also been examined. [7],[8] Most notably, Ahles et al.[7] confirmed this after their study on long-term breast cancer and lymphoma survivors, five years post their diagnosis. The authors found that the patients who received CT scored poorer than the ones who did not receive CT. Among the breast cancer survivors, the women who were on systemic chemotherapy scored less than those who were on local chemotherapy (P < 0.04) in verbal memory (P < -01) and psychomotor function (P < 0.03). In fact, the systemic CT group also scored less on the overall neuropsychological performance index (NPI), (P < 0.01) and reported more problems on the Squire Memory Self Rating Questionnaire (P < 0.02). The authors showed that more cycles of CT are associated with decreased NPE scores (P < 0.02). No significant difference was found between the groups who had or had not taken tamoxifen. There are certain limitations in this study, all the women taken in the study were post menopause, and moreover none of them underwent cognitive testing prior to CT. Schagen et al., [9] corroborated the present study with their earlier findings of 1998, a cross-sectional study done on patients receiving high-dose cyclophosphamadide, thiotepa, and carboplatin (CTC) therapy and ones receiving standard dose cyclophosphamide, epiribucin, and 5 flurouracil (CEF) therapy. The CTC group showed a greater cognitive decline in cognitive performance than the healthy controls. This was a longitudinal study performed on three groups of BC patients; the first group of 28 women were on a high dose of CTC; the second group of 39 women were on a standard dose therapy of CEF, and the third group of 57 early-stage women did not receive any chemotherapy. All three groups were compared with 60 age-matched healthy controls. The neuropsychological testing for patients were conducted prior to and after six months of their therapy, whereas, the controls underwent cognitive testing at a repeat interval of six months. The group on CTC performed worse than the control group (25 vs. 6.7%; odds ratio (OR) - 5.3, 95% CI = 1-3-21.2, P = 0.02). The authors also did not report any difference in the group on CEF and the group without any CT, when their performances were compared with the controls. One important advantage of this study was its longitudinal design and the incorporation of neuropsychological testing for both pre- and the post-treatment phases and also the comparison of different chemotherapy regimens. The study also had several limitations; the use of tamoxifen was not controlled, all the patients on CT were also on tamoxifen, whereas, the no-CT group was not. Therefore, the influence of tamoxifen on cognitive functions could not be clearly determined. Moreover, both the high-dose CTC group and the standard-dose CEF group showed a difference in their cognitive test performance; this itself confounds the test results as it cannot be solely attributed to either the CT regimen or the use of tamoxifen, or the combination of both. Also, the practice effects of the tests were modified based on the re-testing results of the healthy group, although the re-testing intervals for these groups were different. This in itself could downplay the underlying cognitive impairments in the patient groups. Some studies have demonstrated no changes in cognitive abilities after adjuvant CT or the use of tamoxifen for six months. Patients on CT and tamoxifen were in fact more likely to self-rate themselves as being cognitively impaired than the healthy controls, after six months. [10] More prospective studies are required in this regard to ascertain the effects of CT on cognition. A meta-analysis on six studies, of which five were cross-sectional and one was prospective, was done on 208 patients who were on adjuvant CT. The authors found that women on adjuvant therapy were affected by cognitive impairments, but the severity of the cognitive decline depended on the type of design used (cross-sectional vs. prospective). [11] [Table - 1]. Effects of Anxiety and Depression The effects of psychological distress on patients diagnosed with cancer are immense. [16],[19] A rigorous CT regimen intensifies the patient′s distress, further causing extreme anxiety and depression related to the adjustment and coping strategies. A few studies have in fact shown that coping strategies are directly influenced by the stage and severity of the disease and sociocultural confluence coupled with the patient′s own emotional disposition. [20],[21] Chintamani et al., [22] assessed the levels of anxiety and depression in a group of 84 BC patients on neoadjuvant CT (CAF regimen) at each stage, with the Hospital Anxiety and Depression Scale (HADS). The patients were mostly uneducated. The authors found that it was the women who failed to respond to CT suffered from depression (70.5%), when compared to the women who had shown positive improvement after CT (22%). The study also confirmed that depression was higher in literate (25, 54.3%) and employed (14, 53.8%) patients. Another significant contributor was the presence of family support as the women who came from a large supportive family systems coped better with the illness than the ones who were from smaller families. The patients′ subjective perceptions were not included and the small sample size limited this study. Similar prospective studies can be conducted to learn about the CT influence on cognitive functions. Neuropsychological Assessments Chemotherapy-induced cognitive changes are subtle and most of the existing test batteries lack methodological consistency, thereby making assessments a tricky affair. Currently, most researchers have settled on three prominent methods of assessing CT-induced cognitive changes, which are, neuropsychological tests, neuroimaging, and phenomenological perspectives. [23],[24] The difficulty of assessing cognitive changes with comprehensive neuropsychological batteries is that they take long hours to administer. Most often, their applicability becomes cumbersome when considering them for clinical trials or prospective studies. Among the cognitive studies discussed, most authors adhered to the verbal and the visual components of the Wechsler Memory Scale (WMS) along with some parts of the Wechsler Adult Intelligence Scale (WAIS). Both these tests are highly sensitive and can detect the slightest deviation in cognitive status. Most researchers agree that the best way to detect specific changes in cognitive functioning would be to evaluate multiple cognitive domains. [24] Extensive, yet brief and highly sensitive tests that can determine CT-induced cognitive changes are recommended. [24] Moreover, a significant determinant of CT-induced cognitive change is the progressive assault of neurotoxicity, which makes following its subtle course of cognitive changes necessary. Selected cognitive tests should be competent enough to track these changes over a period of time, right from CT initiation till its cessation and the subsequent time afterward to track its long-term changes. The tests mentioned are adept in determining the long-term effects of certain chemotherapy regimens, [25] but are restricted in several ways, particularly the re-testing validity. As the clinical setting demands more than a single timeframe for assessment, the concern is how to protect against the practice effects of repeated neuropsychological testing. [25] Gaining popularity these days are some of the computerized versions of neuropsychological test batteries owing to their brief administration time, easy applicability, and compactness. Some of these batteries reviewed in literature are the CogState, which comprises of psychomotor speed and dexterity, learning and memory tasks, along with executive function assessment (Collie et al..), [26] The CANTAB (Fray and Robbins), [27] holds a superior edge here because of its suite of cognitive tests, designed to assess multiple cognitive domains. What accentuates its significance is its competent applicability across race and culture and also its re-usability. Neuroimaging Findings A recent systematic review [28] was done in 12 studies on brain anomalies in breast cancer patients, using both structural and functional neuroimaging techniques. The studies so far have shown a wide variability, with different areas of the brain being susceptible to susceptible to the onslaught of CT. Here, studies were structured according to the findings of different brain areas concerned. Six studies involved the limbic areas of the brain. All of them had a mixed prevalence of women with neuropsychiatric symptoms associated with depression and post-traumatic stress, in combination with patients on tamoxifen, estrogen therapy, and adjuvant chemotherapy. Most authors reported a decrease in the gray matter volume in the amygdala [29],[30] and the hippocampus. [31],[32],[33] Although, the study by Inagaki et al., [34] showed that the breast cancer patients on adjuvant CT showed decreased gray matter volume in the parahippocampal gyrus. [35] Two other studies that showed the involvement of the basal ganglia were those on BC patients on tamoxifen and estrogen therapy [36] and CT with tamoxifen. [37] The study by Inagakai and group [34] also showed reduced gray matter volume in the prefrontal cortex (PFC) and precuneus in BC patients who were on CT and those without CT, whereas, [37] their findings on patients on tamoxifen and CT showed decreased glucose metabolism in the frontal cortex and the cerebellum. Patients undergoing major depression too showed a similar decreased state in the PFC. [38] Some negative findings too were reported, in fact, like the study by Yoshikawa et al,. [39] on BC patients on CT, who found no change in the hippocampus. The differences in most of the studies reviewed were attributed to methodological inconsistencies like study design, test batteries used, comorbid drug therapy, and the control groups. Chemotherapy, Neurotoxicity, and Cognitive Decline Chemotherapy regimens used in BC have a direct dose-dependency effect on cognitive status and functioning. [40] Subsequent cognitive disturbances are caused as these drugs act by targeting the nerve fibers, altering the brain metabolism. [41] In fact, long-term neuronal injury has also been attributed to a proinflammatory cytokine environment that incites plasma TNF Alpha levels during chemotherapy use, [42] and psychological distress [43] that could begin even before the use of CT. Persistent stress elevates the level of glucocorticoids [44] caused by hypothalamo-pituitary-adrenal (HPA) axis dysregulation. [45] Increased glucocorticoids trigger damage to the structural and functional areas of the brain. [46] Within the hippocampus itself, which comprises mostly of the glucocorticoid receptors, the damage is profound; experimental studies on animals too confirm this phenomenon, where elevated glucocorticoids often have a detrimental effect in the form of heightened susceptibility to neurotoxic stress, obstructed neuronal growth, and increased cell death within the hippocampus. [46],[47],[48] As one reviewer noted, [6] most studies have concentrated on the hippocampus and its role in new learning and memory consolidation while examining the effects of chemotherapy. [13],[18],[49],[50] The most prominent complaints are in the areas of attention and concentration and short-term memory retrieval; [3],[4],[6] problems with memory consolidation have hardly been reported, implicative of frontal-subcortical white matter involvement. [6] Research by Noble and colleagues [51] has shed new light on the cognitive problems marked by the use of CT and its persistence even years after CT was discontinued. The authors highlighted the role of 5-fluorouracil (5-FU), one of the potential CT drugs used extensively to treat breast and colon cancer and its lasting damage to myelin. When extended to mice, the authors found a brief, yet sharp, elevation in apoptosis in several brain regions, which gradually subsided. Suppressed proliferation, essential for the normal functioning of the brain, too was reported in several regions including (the subventricular zone, the dentate gyrus of the hippocampus, and the corpus callosum). Furthermore, the auditory brain stem response revealed a slowdown in the impulse conduction between the ear and the brain, suggestive of myelin loss. Similar findings were reported on BC survivors, three to six years post CT treatment, where 5-FU was a part of the treatment regimen. Here too the survivors showed abnormalities in auditory processing. [52] Future Considerations One million new cases of breast cancer are reported in the world each year, making it the most common form of malignancy in women, covering 18% of all female cancers. [53] India too has witnessed a steep rise in the incidence of breast cancer patients in recent years. [54] An approximate of 100, 000 new cases are currently reported each year. [54] The epidemiological study [19] done in Haryana on 304 patients reported the average age as 47 years, a difference of 10 years from their Western counterpart, chiefly due to the younger age structure of our population. Rise in the screening and awareness programs too have contributed to the incidence rate. [55] A critical need for this populace is longitudinal prospective studies. As our population is mixed, a good combination of both urban and rural samples should be considered for study designs. Patients from the lower socioeconomic background have a poorer compliance toward continuing with a multimodal therapy. In many parts of India, early diagnosis is rare and most patients are well advanced in their disease stages before diagnosis is made. [19] As one study reported, [22] patients who were not responding to CT were clinically more depressed than the patients who were compliant with the therapy. Also, depressive features were more common among the literate. Thus, confounding variables like psychological stress, fatigue, and anxiety have to be considered. The subjective perception of the patient′s own problem should be compared with the objective scores, as was discussed in the studies by Castellion et al., Poppelreuter et al., and Bender et al. [3],[4],[5] Findings can only be accurately verified in longitudinal designs where cognitive performance of patients is assessed over time and matched with the pretreatment performance. Prior to CT initiation, a cognitive and psychological assessment is essential, to rule out any pre-existing cognitive or / and psychiatric disorders. Prospective studies should also consider larger sample sizes as smaller sample studies pose severe limitations. Test batteries that can be generalized and are non-culture specific, easy to administer, less time consuming, and yet highly sensitive should be considered [24],[25] and the confounding effects of repeated testing should also be monitored. [25] Another important aspect is comparing the different types of neurotoxic CT regimens. Direct dose- dependent effects of CT regimens on cognitive performance were discussed. [7],[9],[15] Schagen et al.[9] in fact adhered to cognitive testing for both pre- and post-therapy phases. The use of the anti-estrogen therapy, tamoxifen, in patients who are on CT regimen should also be considered when designing a study. The link between BC and Estrogen Replacement Therapy (ERT) is controversial, owing to various methodological inconsistencies and the varying prevalence rate in different countries. [56] A study reported by Meherishi et al., [56] on the use of menopausal hormonal therapy (MHT) in Jaipur, India, stated that most practitioners currently use HT only as a reserve against menopausal symptoms. A dotted rural and urban population only aggravates the problem, where the level of education and socioeconomic distribution contribute to awareness. Physician awareness plays an important role here, particularly during clinical examinations, which most often are incomplete, with most symptoms going unreported. Patients when they come for therapy are oblivious of the cognitive side effects of chemotherapy, and so it becomes imperative that the physician safeguards the former′s interests by addressing these problems and coming to a shared understanding when drawing out a plan for continued cognitive and emotional rehabilitative support, even after the cessation of chemotherapy. To enable clinicians to follow the onset and progression of neurotoxicity from the inception of CT itself, an extensive suite of methods that will guide the clinical examination is required. This will help harmonize their decisions during the chemotherapy course. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11069t1.jpg] |
| |||||||||

{kind=link}