 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
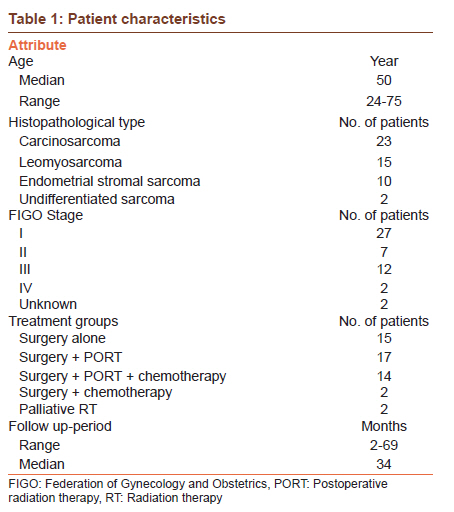
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 270-274 Original Article Clinical outcome of patients with uterine sarcomas Daya Nand Sharma1, Goura Kisor Rath1, Sunesh Kumar2, Lalit Kumar3, Neerja Bhatla2, Ajeet Kumar Gandhi1, Roopa Hariprasad3 1 Department of Radiation Oncology, All India Institute of Medical Sciences, New Delhi, India PMID: 22044806 DOI: 10.4103/0973-1482.87011 Materials and Methods: We retrieved the information regarding the patient's demography, clinico-pathological details, treatment given, survival, and complications of all the US patients treated at our center between the years 2000-2008. The three-year overall survival (OS) was determined with respect to various prognostic factors like age, stage of disease, histopathological type, adjuvant RT etc. Results: A total of 50 case records were retrieved for this retrospective analysis. Age ranged from 24 to 75 years with a median of 50 years. Carcinosarcoma was the commonest histopathological type (23/50 patients). FIGO stage distribution was: stage I, 27; stage II, 7; stage III, 12; stage IV, 2; and unknown stage, two patients. Forty-eight patients underwent surgery; 31 received postoperative radiation therapy (PORT) and 16 received chemotherapy therapy. Median follow-up period was 34 months (range 2-69 months). The three-year OS for the entire group of patients was 42%. Stage of the disease, histopathological type, and use of PORT were found significant prognostic factors for survival. Conclusion: Although limited by small sample size and retrospective nature, ours is the only study on US being reported from India. Our results have demonstrated FIGO stage of the disease, histopathology and use of PORT to be the significant prognostic factor for survival. Use of chemotherapy in future trials is warranted. Keywords: Clinical outcome, retrospective analysis, uterine sarcoma
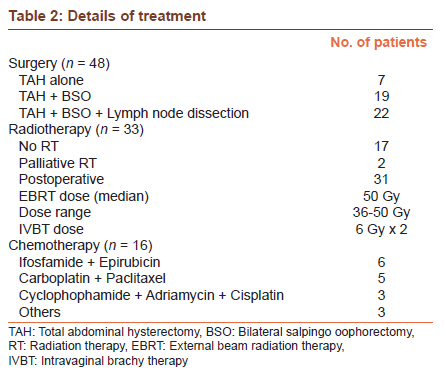
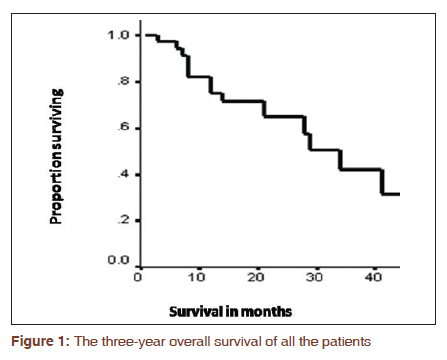
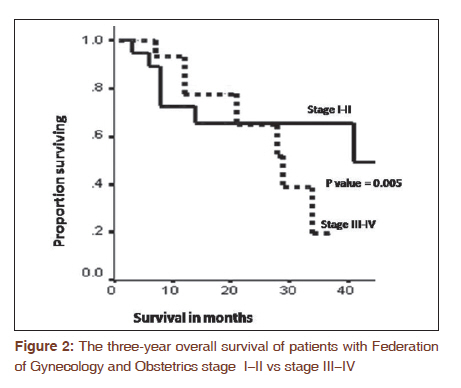
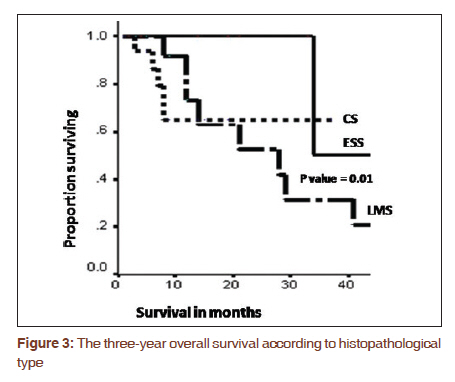
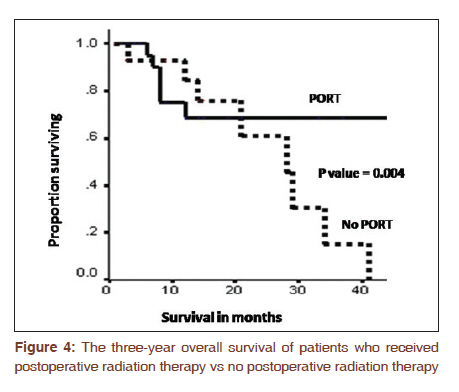
Introduction Uterine sarcomas (US) are rare tumors comprising 1-3% of all gynecologic malignancies and 4-9% of all uterine malignancies. [1],[2] They usually have aggressive clinical behavior with propensity to local recurrence and distant metastases. Common histological types of US are malignant mixed mullerian tumors (MMMT), also known as carcinosarcomas (CS), leiomyosarcomas (LMS) and endometrial stromal sarcomas (ESS). Recently, CS has been reclassified as a de-differentiated or metaplastic form of endometrial carcinoma (EC). Despite this, and probably because it behaves more aggressively than the ordinary (EC), CS is still included in most retrospective studies of US. ESS is low grade, indolent tumor with favorable prognosis. CS and LMS together account for about 85% of all cases, and ESS accounts for the remaining 15% of cases. US occur primarily in women aged 40 to 60 years. [2],[3] Abnormal uterine bleeding, abdominal or pelvic mass and pain are the most common symptoms of patients. The most frequent prognostic factors include tumor stage, histological subtype, grade, lymphovascular invasion, and menopausal status. [3],[4] The staging of US is based on the International Federation of Gynecology and Obstetrics (FIGO) staging system for uterine corpus cancer. Till FIGO′s revised staging system [5] in 2009, all US were staged like endometrial carcinoma but in the revised system, they have a separate staging system, although CS is still staged like EC. All US carry a poor prognosis with an overall survival of less than 50% at two years, even when presenting at an early stage. [6] Standard treatment for early-stage patients is hysterectomy and surgical staging. About half of these patients develop recurrent disease within five years of initial therapy. [7] Postoperative radiation (PORT) seems to improve local control without a significant impact on overall survival. [3],[8] There is emerging evidence in the literature regarding the role of adjuvant chemotherapy. The rarity of US and their aggressive clinical course has resulted in a relatively limited amount of literature. Our present study, the first being reported from India, is a retrospective analysis of 50 patients treated at our center. The aim of this study was to study the treatment results of US and to share our experience with literature. Materials and Methods For this retrospective analysis, we retrieved the case records of all the histopathologically proved US patients treated at our center between the years 2000 and 2008. From each case record, we extracted the information regarding the patient′s demography, clinicopathological details, treatment given, survival, and complications. The initial pretreatment work-up of the patients consisted of detailed clinical examination in the gynecologic oncology clinic by a team comprising of gynecologist, radiation oncologist, and medical oncologist. Each patient was subjected to various routine hematological and radiological investigations. Computed tomography (CT)/Magnetic resonance imaging (MRI) scan of the abdomino-pelvic region and cysto-sigmoidoscopy were done, if necessary. Staging was done according to FIGO system. [9] The selection of treatment modality was decided by the gynecologic oncology clinic team. Surgery in the form of total abdominal hysterectomy (TAH) and bilateral salpingo oophorectomy (BSO) with or without pelvic lymph node dissection was usually contemplated for all the operable patients. Depending upon the various clinical and surgico-pathological factors, decision of adjuvant therapy with radiation therapy (RT) and or chemotherapy was taken by gynecologic oncology clinic team. Adjuvant RT consisted of combination of external beam radiation therapy (EBRT) to whole pelvis followed by intravaginal brachytherapy (IVBT) to vault. The prescribed dose of EBRT was 45-50 Gy with conventional fractionation (1.8-2.0 Gy per fraction, 5 days a week) with four field box technique (2 AP-PA and 2 lateral fields). Treatment was carried out on either cobalt-60 or linear accelerator. After the completion of EBRT, IVBT was performed to treat vaginal cuff using intravaginal cylinders. The dose of IVBT was prescribed at a depth of 0.5 cm from the surface of the ovoids. A dose of 6 Gy × 2 (weekly) by high dose rate (HDR) was delivered using remote after loading unit. Follow-up was done every one month for the first three months and then every three months till one year. Subsequently, they were followed-up every three-six months. At every visit, clinical examination was performed and, if necessary, CT/MRI scans, to assess the disease status. Annual X-ray chest was done to rule out lung metastases. Positron Emission Tomography (PET) scan was also done if there was a suspicion of disease on clinical/radiological examination. Statistical analysis was performed using the statistical software SPSS, version 11.5. The overall survival (OS) was calculated by Kaplan-Meier survival method. [10] Late toxicity was assessed as per the Radiation Therapy Oncology Group (RTOG) criteria. [11] Each patient, who lost follow-up after a certain period was censored at that point of time for survival analysis. OS was determined with respect to histopathological type, stage of disease, treatment group, etc. Due to small sample size, only univariate analysis was done rather than multivariate analysis. Log rank test was used to find out the P value and a value of <0.05 was considered significant. Results A total of 50 case records were retrieved for this retrospective analysis. Various patient characteristics are given in [Table - 1]. Age ranged from 24 to 75 years with a median of 50 years. CS was the commonest histopathological type. Most patients (27 out of 50) belonged to stage I disease. Two patients had distant metastases, 1 in lung and 1 in bones. Two patients had unknown stage, both were operated outside before coming to our hospital. Forty-eight of 50 patients underwent surgery with or without adjuvant therapy. Remaining two patients were not considered for surgery since both of them had distant metastases. [Table - 2] shows the treatment characteristics of the patients. TAH + BSO + lymph node dissection was the commonest surgical procedure (22 of 48 patients). Thirty-one patients received PORT, while 17 were not considered for RT at all. Three of 31 patients could not complete the prescribed course of pelvic EBRT and received a dose of 36-40 Gy. Two patients received palliative RT in view of the metastatic disease. Sixteen patients received chemotherapy with different regimes. Ifosfamide + epirubicin combination was the commonest chemotherapy regimen followed by carboplatin + paclitaxel [Table - 2]. Median follow-up period was 34 months (range 2-69 months). Out of 50 patients, 33 (66%) had no evidence of disease and 17 (34%) had failure. Of 17 failures, 10 were confined to pelvis rest 7 to extra pelvic sites (lungs 4, para-aortic nodes 2, liver 1, bones 1, supraclavicular node 1). The three-year OS for the entire group of patients was 42% [Figure - 1]. There was no significant difference in three-year OS between the patients <50 years of age and older (47% vs 39%; P value 0.7). As shown in [Figure - 2], the three-year OS in stage I-II and III-IV was 65% and 19%, respectively (P value 0.005). As depicted in [Figure - 3], the three-year OS for CS, ESS, and LMS was 65%, 50%, and 21%, respectively. LMS patients had significantly poorer three-year OS (P value 0.01) but the difference in survival between CS and ESS was not significant (P value 0.8). Adjuvant RT had significant impact on the survival. The three-year OS of the 31 patients, who received PORT, was 66% as compared to 17% of the 17 patients who did not receive PORT (P value 0.004) [Figure - 4]. Although patients receiving chemotherapy had poor three-year OS (27%) but it had no significant impact (P=0.18). Delayed toxicity was observed in five patients (three in PORT patients and two in non-PORT patients). The pattern of delayed toxicity was: sub acute intestinal obstruction, two patients; lymphoedema, radiation cystitis, radiation proctitis; one each. Discussion US is relatively a rare and aggressive gynecological malignancy. Due to lack of large randomized controlled trials; most treatment guidelines are based on small and retrospective studies in the literature. Though our study has a limited sample size but it is the only one being reported from India. Therefore, the results of our study may reflect the Indian scenario and possibly generate interest among the readers for further research. Since the median follow-up in our series was close to three years (34 months), we chose three-year OS statistics to correlate the various possible prognostic factors. Our study has revealed a decent three-year OS rate of 42%. The results of our study may not be strictly comparable to that in the literature due to small population of patients. Livi et al.,[3] in their series have shown three-year survival rate (41.8%), almost similar to ours. Our results have demonstrated FIGO stage of the disease, histopathological type and use of PORT to be the significant prognostic factor for survival. Age of patient and use of chemotherapy failed to show impact on survival. It is not clear from the literature whether histological type is an independent prognostic factor. Several authors [12],[13],[14] have reported the significant impact of histological type on clinical outcome while others [4],[15],[16],[17] have failed to demonstrate so. ESS has the best prognosis followed by CS and LMS. Though LMS in our series had worst survival but, ESS has slightly inferior outcome than CS, though statistically insignificant. Stage of the disease has been found to be significant prognostic factor in most series, including ours. We have combined the stage I-II (early stage) and stage III-IV (late stage) to calculate the survival since the number of patients in individual stages is very small. We observed significantly better survival in early stage than in late stage [Figure - 2]. Complete surgical resection is the standard treatment for all types of uterine sarcomas. CS and ESS require the same extended surgical staging as is done for endometrial adenocarcinoma. The pelvic lymph node metastasis in CS and ESS is about 15%. LS tend to disseminate hematogenously and the incidence of nodal spread has been reported to be less than 5%. [18] Therefore, TAH with or without BSO is an adequate surgical procedure for LS. The role of adjuvant RT is debatable. Adjuvant pelvic RT appears to improve local control without any significant impact on overall survival however several authors [1],[14],[19],[20] have noticed improved survival with PORT. We have observed a statistically significant better survival in patients who received RT than who did not [Figure - 4]. In general, PORT should be recommended in those patients with adverse features like positive surgical margins higher grade, pathologically positive nodes, or evidence of gross residual disease. Livi et al.,[3] reported their 27 years of experience (1974-2001) of treating 141 patients with US. They found that PORT with a total dose higher than 50 Gy (EBRT + brachytherapy) significantly (P = 0.001) reduced the local recurrence. They further opined that decrease in local recurrence rate in a large number of patients might translate into a survival advantage. Sampath et al.,[8] recently reported the largest retrospective analysis, so far, from a National Oncology Database of 3,650 patents with US. The primary goal of their study was to analyze the impact of PORT on clinical outcome. This study revealed that PORT significantly improved local control, with a 53% reduction in the risk of local-regional failure at five years compared to surgery alone. However, it did not significantly improve OS. IVBT alone or more often with pelvic EBRT has been tried in some studies [3],[8],[19],[21] to improve results specially for reducing vaginal recurrence rate. Livi et al.,[3] observed best results with adjuvant therapy in the form of EBRT + IVBT. They used various adjuvant therapies: EBRT + IVBT, (27 patients); EBRT alone, (37 patients); no further therapy, (36 patients); and chemotherapy alone, (20 patients). They reported three-year local recurrence rates of 28%, 31%, 62%, and 71%, respectively (P=0.0008). Regarding adjuvant chemotherapy, there is little evidence in the literature supporting its use except for CS. We observed no significant impact of chemotherapy on survival probably because of less number of patients in chemotherapy group (16 patients). Slight inferior three-year OS with the use of chemotherapy in our series is mainly due the fact that patients with higher stage of disease were considered for chemotherapy. More trials are needed to address these issues, especially, their sequential application. Based on some recent, albeit limited data, combinations such as paclitaxel and carboplatin in CS, as well as gemcitabine and docetaxel in LS merit further evaluation in prospective trials of adjuvant treatment. Conclusion Ours is the only series on US being reported for the first time from India. Although limited by small sample size and retrospective nature, it reveals certain important findings. Our results have demonstrated FIGO stage of the disease, histopathology, and use of PORT to be the significant prognostic factor for survival. Age of patient and use of chemotherapy has no impact on survival. Since distant metastases is a concerned site of failure, use of chemotherapy in future trials is warranted. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11070t1.jpg] [cr11070f1.jpg] [cr11070t2.jpg] [cr11070f2.jpg] [cr11070f3.jpg] [cr11070f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}