 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 275-279 Original Article Assessment of quality of life of cancer patients in a tertiary care hospital of South India Gopal Kannan1, Vanitha Rani1, Raja Madras Ananthanarayanan2, Thennarasu Palani1, Nidhi Nigam1, Vasantha Janardhan1, Uma Maheswara Reddy3 1 Department of Pharmacy Practice, Faculty of Pharmacy, Sri Ramachandra Medical Center and Hospital, Chennai, India PMID: 22044807 DOI: 10.4103/0973-1482.87013 Settings and Design: A prospective study in the medical oncology clinic of a tertiary care hospital of South India. Materials and Methods: Patients receiving chemotherapy for different types of cancer were subjected to a validated questionnaire and their responses to the factors of the questionnaire were scored and analyzed. A Chi-square test was performed to assess the effect of age and type of cancer on the QOL of patients. Pearson's correlation was done to assess the factors that had greater influence on the QOL. Results: A total of 32 (15 males; 17 females) patients were included and majority were in the age range of 61-80 years. Eleven types of cancer were identified. About 56% of the patients were assessed to have average QOL and 28% had below average QOL, 9% had above average, and 2 (6.25%) had significantly high QOL. The overall mean QOL score of the study population was 122.38 ± 13.86. Factors 1 (psychological well-being), 2 (self-adequacy), 3 (physical wellbeing), 4 (confidence in self-ability), 6 (pain), 7 (mobility), and 8 (optimism and belief) had significant influence on the QOL, while factors 5 (external support), 9 (interpersonal relationship), and 10 (self-sufficiency and independence) did not have a significant effect on QOL. Age (P=0.396) and type of cancer (P=0.371) did not have a significant effect on the QOL. Conclusion: The study showed that 80% of the total study population reported to have average and below average QOL, suggesting that an increasing importance is given to the incorporation of Quality of Life as an outcome, in addition to other clinical endpoints. Keywords: Cancer, chemotherapy, quality of life
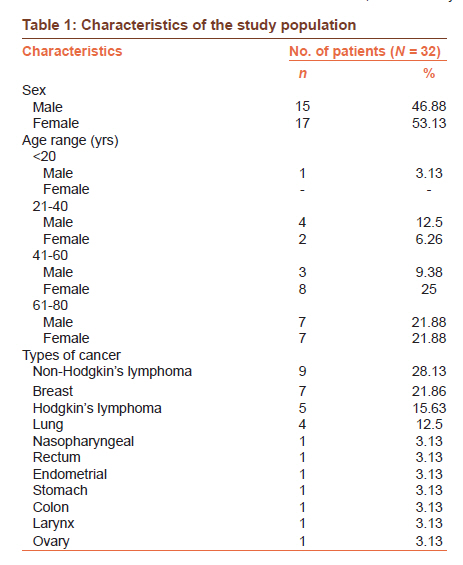
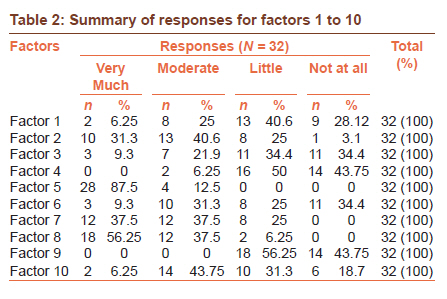
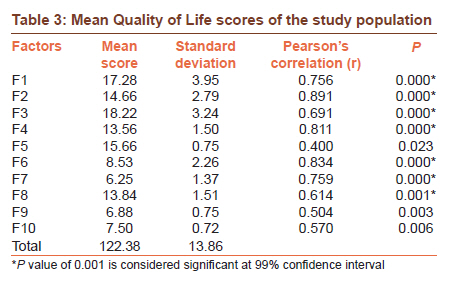
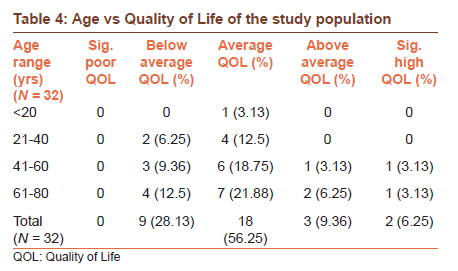
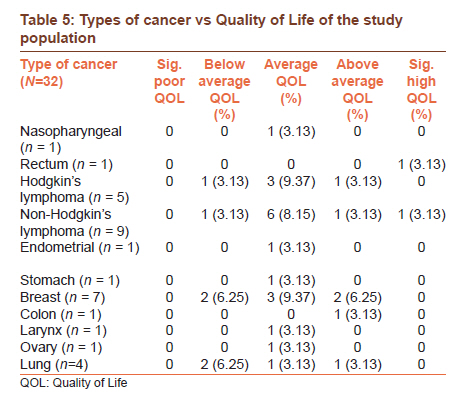
Introduction Incidence of cancer in India varies from 44-122 per 100,000 population in males and 52-128 per 100,000 population in females. It is estimated that, at present, nearly one million new cancer cases are being detected annually in the country. [1] For patients and their family, a diagnosis of cancer brings challenges to many aspects of daily life, with a major concern being maintaining the highest quality of life possible during and after the experience. [2] Quality of Life (QOL) is a descriptive term that refers to people′s emotional, social, and physical well-being as well as their ability to function in ordinary tasks of living. [3],[4] QOL assessment has become increasingly common in the field of cancer and has been identified as the second most important outcome with survival being the most important. [5],[6] QOL is measured using specially designed and tested instruments, which enable the carer to monitor and evaluate the effects of a treatment or condition from the patient′s perspective. [7] This study was carried out with the objective of measuring the quality of life of cancer patients during their cancer treatment. Materials and Methods The study was carried out for a period of 6 months in the oncology clinic of a 1,700-bed tertiary care teaching hospital in South India, after obtaining approval from the institutional ethics committee. Cancer patients of both sexes, aged above 18 years, receiving chemotherapy and consented to participate in the study were included. The data including patient demographics (age, sex), type of cancer, and duration of the disease at the time of assessment were obtained from patient history interview and case records, and entered in the data collection proforma designed for the study. The quality of life of patients was assessed using a QOL questionnaire designed and validated by Vidhubala E, et al., [8] with a reliability of Cronbach alpha of 0.90 and Split-half reliability of 0.74 (using Alpha coefficient and Guttman Split-half reliability method). The questionnaire consisted of 10 factors: Factor 1 (F1) evaluated the psychological well-being of the study population. It consisted of six items ranging from F1.1 to F1.6 (F1.1-Sadness or depression interfering with everyday functioning; F1.2- Feeling lonely or remote; F1.3- Feeling depressed; F1.4- Physical condition reducing economic status; F1.5- Feeling of nothing important to do, in spite of too much free time; and F1.6- Feeling of low performance compared to one′s ability). Factor 2 of the QOL questionnaire evaluated the self-adequacy of patients, and it consisted of five items from F2.1 to F2.5 (F2.1 - Feeling of adequacy toward working capacity; F2.2 - Feeling of comfort in attending functions; F2.3 - Feeling of satisfaction with the body looks; F2.4 - Feeling of satisfaction with present health status; and F2.5 - Feeling of satisfaction with overall Quality of Life). Factor 3 consisted of six items stating the physical well-being of patients (F3.1 - Need of rest; F3.2 - Satisfaction with sex life; F3.3 - Sleep problems; F3.4 - Losing temper and regretting; F3.5 - Effects on bowel movement; and F3.6- Difficulty in remembering things). Factor 4 (F4) evaluated the confidence in the self-ability of study population. It consisted of four items: F4.1 to F4.2 (F4.1 - One′s efficacy in managing financial needs; F4.2 - Ability to fulfill family needs; F4.3 - Satisfaction in fulfilling responsibilities; and F4.4 - Ability to concentrate on daily activities). Factor 5 assessed the external support attained by the patient. It consisted of four items: F5.1 to F5.4 (F5.1 - Support of doctor and informational support; F5.2 - Treatment adequacy; F5.3 - Support of family and spouse; and F5.4 - Support of friends and relatives). Factor 6 evaluated the extent of pain experienced by the study population and consisted of three items: F6.1 to F6.3 (F6.1 - Experience of pain; F6.2 - Interference of pain in day to day life; and F6.3 - dependency on medication). The two items (F7.1 and F7.2) of factor 7 assessed the mobility of the patients (F7.1 - Ability to interact with people; and F7.2 - Ability to move around as usual). Factor 8 (F8) evaluated the optimism and belief of study population and it consisted of four items F8.1 to F8.4 (F8.1 - Expectation of good things to happen; F8.2 - Self-importance; F8.3 - normal appetite; and F8.4 - personal beliefs/religious belief). Factor 9 (F9) and factor 10 (F10) assessed the interpersonal relationship and self-sufficiency and independence of the study population, respectively, and consisted of two items each (F9.1 - Interference of medical treatment in sexual life; F9.2 - Relationship with family members; and F10.1 - Sharing of problems with family; F10.2 - Requirement of assessment in day-to-day activities). Scaling technique Likert-type four-point rating scale was added to elicit responses from the respondents ranged from 1-4. For example, Do you feel depressed? [Scale 1] A few items were scored in reverse so as to make the questionnaire unidirectional and to yield a global QOL score. For example, ′Are you satisfied with your working capacity?′ If the answer is ′very much′, it will be scored in reverse, ie, 4 as 1 and 1 as 4 to obtain a positive QOL index. The direct and reverse scoring items are given below. Direct Scoring: 1, 2, 3, 5, 6, 7, 8, 11, 14, 17, 18, 16, 19, 21, 26, and 32. Reverse Scoring: 4, 9, 10, 12, 13, 15, 20, 22, 23, 24, 25, 27, 28, 29, 30, 31, 33, 34, 35, 36, 37 and 38. The factors of the questionnaire were explained to the patients and they were given sufficient time to answer the items. The responses obtained from the patients were scored as stated in the questionnaire and QOL was measured. Interpretation of QOL scale 88 and below=significantly poor QOL 89-108=below average QOL 109-132=average QOL 133-144=above average QOL Above 144=significantly high QOL Statistical analysis Data were entered prospectively in a computerized database and analysis was done with SPSS statistical software (10.0 version). Chi-square test was performed to assess the effect of age and type of cancer on the QOL of the patients and P<0.05 was considered significant. Pearson′s correlation test was done to assess the factors of the questionnaire that had mostly affected the QOL. Results A total of 32 cancer patients were included in the study, of which 15 (46.88%) were males and 17 (53.13%) were females. A majority of the patients were in the age range of 61-80 years (7 males and 7 females). At the time of assessment, 29 patients (90.63%) were under treatment, 2 (6.25%) were newly diagnosed, and 1 (3.13%) was under remission. The study population had different types of cancer, of which 9 patients (28.13%) had non-Hodgkin′s lymphoma and 7 female patients (21.86%) had breast cancer [Table - 1]. The QOL questionnaire consisted of 10 factors, each consisting of items summing up to 38. The responses given by the study population for all items were summed up and the average responses for all the factors were calculated [Table - 2]. The responses obtained for the QOL questionnaires were scored and tabulated [Table - 3]. The mean scores of the patients were as follows: 72% patients scored 17.28 ± 3.95 for factor 1; 73.3% patients scored 14.66 ± 2.79 for factor 2; 75.91% patients scored 18.22 ± 3.24 for factor 3; 84.87% patients scored 13.56 ± 1.50 for factor 4; 97.87% patients scored 15.66 ± 0.75 for factor 5; 71.08% patients scored 8.53 ± 2.26 for factor 6; 78.12% patients scored 6.25 ± 1.37 for factor 7; 86.5% patients scored 13.84 ± 1.51 for factor 8; 86% patients scored 6.88 ± 0.75 for factor 9; and 93.75% patients scored 7.50 ± 0.72 for factor 10. The overall mean score of the 80% of the study population was found to be 122.38 ± 13.86. Based on Pearson′s correlation, all factors except factors 5, 9, and 10 were found to be the most affecting factors of the QOL of the study population. Of the 32 patients, 18 (56.25%) were found to have average QOL, 9 (28.13%) had below average QOL, 3 (9.36%) had above average, and 2 (6.25%) had significantly high QOL. The study showed that 56% of the patients had average QOL and 28% of population had below average QOL. It also indicated that no patients had significantly poor QOL. [Table - 4] shows the QOL distribution in various age groups. There were no significant changes in the QOL in different age groups (P=0.396). Similarly, types of cancer also did not have a significant effect (P=0.371) on the QOL of the study population [Table - 5]. Discussion Quality of life is the state of well-being that is a composite of two components: the ability to perform everyday activities that reflect physical, psychological, and social well-being; and patient satisfaction with the levels of functioning and control of the disease. [9] Until recently, extremely less attention was paid to cancer patients′ quality of life. Clinical trials have suggested that one can measure quality of life as an independent predictor of survival. [10] QOL assessment has become increasingly common in the field of cancer. The trend reflects a growing appreciation of the need to evaluate cancer treatments more broadly than just by tumor response or survival. In cancer treatment, survival is the most important outcome and QOL assessment has demonstrated clear research value as a secondary outcome measure. Multidimensional approach of QOL assessment reflects the patient′s situation and presents important information for the process of treatment evaluation. [11],[12] For the first five items of Factor 1, up to 80% of the study population reported that they were little or not affected by the feeling of depression or loneliness and their physical condition has not reduced the economic status. The results suggested that a major percentage of the study population had significantly lower satisfaction with their performance ability. Therefore, efforts should be made to increase their performance ability by supporting and educating them. The second factor was "Self-adequacy", which had five items. A major percentage of the study population considered themselves adequate regarding their working capacity and did not feel any discomfort while attending functions. The results showed that most of the participants were moderately or little satisfied with their body looks and none of the participants were fully satisfied with overall QOL. This clearly indicates that efforts should be made to increase overall QOL by supporting them physically and emotionally. The third factor was "Physical well being". The results showed that the disease condition had moderately affected the physical condition of the major percentage of the population. Most of the participants felt that they were little or not at all affected by a condition of losing temper and poor remembrance, while almost 50% of study population felt that they needed more rest. The results clearly indicate that proper nutritional supplement should be provided to patients, which could increase their working capacity. The results of the fourth factor indicate that on an average, the whole study population is confident about their self-ability. Only a few participants were less confident about their efficacy in managing financial and family needs and less satisfied with their fulfilled responsibilities. The results of the fifth factor indicate that all participants felt that they had complete support of their doctor and that their treatment was adequate. Up to 80% of the study population felt that they had complete support of family, spouse, friends, and relatives, while only a few participants felt that they had moderate support of family and friends. This indicates that efforts should be made to educate the care givers and family and ask them for full support. The results for the sixth factor showed that a major percentage of the study population experienced moderate or severe pain, which interfered in day-to-day life. Most of the patients found themselves to be dependent on medications. The results indicate that efforts should be made to decrease painful episodes with the help of pharmacological and non-pharmacological therapy. The seventh factor was "Mobility". The results showed that most of the participants were moderately and satisfied with their ability to interact with people as well as to move around as usual. This indicates that major percentage of study population was little affected by the factor of mobility. The eighth factor "Optimism and Belief" and the responses obtained from the patients showed that a major percentage had their personal or religious beliefs, which gave them strength to fight with the disease condition and they believed and expected a complete and good recovery. Only a few participants expressed a lack of appetite while most of them had normal appetite. The results of the ninth factor clearly indicate that the study population had little or no interference of medical treatment in sexual life and were satisfied with their relationship with family members. The tenth factor was "Self sufficiency and independence". The result showed that all participants completely or moderately shared their problems with family and a major percentage of the study population did not require assistance in day-to-day activities. The scores obtained for the study population showed that none of the patients had significantly poor QOL and about 56% of patients were assessed to have average QOL and 28% of the population had below average QOL. Also, 16.5% of the patients had above average and significantly high QOL. Improving patient QOL is an important goal in healthcare [13],[14] and cancer clinical trials, [15],[16] and it is the cornerstone for delivery of good palliative medicine. [17] A physician′s goal is to be an agent of beneficence, which involves giving patients the opportunity to make personal choices in directing their own care to ensure quality of life. [18],[19] Quality of life, survival, and tumor regression are endpoints that physicians and other health professionals are striving for. The ultimate goal is to provide a total patient care to assist cancer patients in achieving the desired endpoints through effective treatment and palliation. [20],[21]
Conclusion The study had shown that the external support given by the physician and family members had a greater influence on cancer patients to adapt well to the situation of having had a life-threatening disease and to undergo their treatment more positively. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11071t5.jpg] [cr11071t2.jpg] [cr11071t1.jpg] [cr11071t4.jpg] [cr11071e1.jpg] [cr11071t3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}