 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 286-291 Original Article Study of the cytogenetic and non-cytogenetic factors in cervical carcinoma in the Jammu region of J and K state Roopali Fotra1, Shashi Gupta2, Subash Gupta1 1 Institute of Human Genetics, University of Jammu, Jammu and Kashmir, India PMID: 22044809 DOI: 10.4103/0973-1482.87019 Results: Both the numerical and the structural chromosomal changes have been recorded in a majority of these growths. In most of the cases, numerical chromosomal changes (95%) outnumbered the structural aberrations. Discussion: Aneuploidy was the most common numerical chromosomal aberration recorded in the majority of the tumor growths. Structural aberrations included translocations and deletions. Non-cytogenetic factors like multiparity, early marriage, poor genital hygiene and rural background were highly prevalent in the present study. Keywords: Aberrations, aneuploidy, cervical carcinoma, parity Introduction Cervical carcinoma the most common gynecologic malignancy, constituting the best material for chromosome study. Approximately 5,00,000 new cases of this cancer are diagnosed worldwide each year, with a survival rate of only 40%. [1] In the developing countries, cervical carcinoma ranks second with a relative frequency of 15% of all cancers in women, whereas in the developed countries, it ranks fifth with a relative frequency of 4.4%. [2] About 1/5 to 1/6 of the total incidence of cervical carcinoma in the world occurs in India. [3] It is estimated that about 132,082 women die due to cervical cancer every year, accounting for 26.7% of the worldwide incidence, whereas the cumulative risk of the incidence of cervical cancer in women in India (age 0-64 years) is 2.4% compared with 1.3% for the world. [4],[5] Besides some identified risk factors, the epidemiological studies have shown the Human Papilloma Virus (HPV) to be the most important risk factor, and the virus is responsible for 99.7% of the invasive cervical cancer worldwide. [6] Young age, early marriage, multiple sexual partners, poor genital hygiene, recurrent miscarriages, high parity, tobacco chewing, oral contraceptive, cigarette smoking, race and low socioeconomic status have also been identified as significant risk factors for the development of CaCx. [7] There are several types of cervical cancer, classified on the basis of where they develop in the cervix. These are:
Approximately 80% of these tumors are SCCs and only 20% are adenocarcinomas. [8] SCC usually starts in the area of the squamocolumnar junction (transformation zone). Occasionally, however, it arises in the endocervix, sometimes deep to the lining. SCC of the cervix is seen in the microinvasive and invasive forms. Some invasive cancers of the cervix are hypertorphic or exophytic, producing a cauliflower-like mass, whereas others are mainly eroding and ulcerative or infiltrative. Histologically, these SCCs are large cell keratinizing, non-keratinizing and small cell types. Adenocarcinomas usually arise in the endocervix, and it is usually ulcerative and infiltrative, leading to hard, indurated, barrel-shaped cervix. [9] Pure adenocarcinomas arise from the endocervical-type cells and constitute about 5-20% of all cervical malignancies. The histopathological patterns include well-differentiated mucinous adenocarcinoma, papillary adenocarcinoma and a clear pattern that contains glycogen but no mucin. Materials and Methods The present study was aimed at:
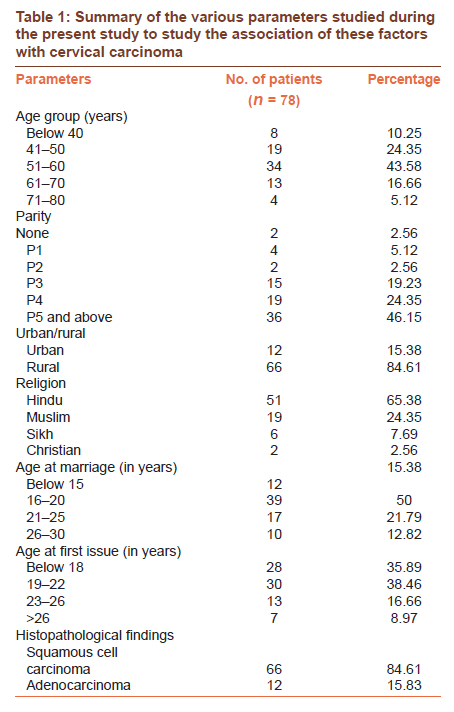
A total of 78 clinically as well as histopathologically confirmed cases of Ca cervix were subjected to the chromosome study of the tumor growth. A standard questionnaire was prepared, which covered various factors associated with the cervical cancer, such as age of the patient, age at marriage, age at first issue, number of pregnancies, smoking/alcohol consumption, rural/urban distribution, ethnic background and use of oral contraceptives. Of the 78 growths, 66 were histopathology confirmed as SCC whereas 12 growths were adenocarcinoma [Table - 1]. A few bits of the tumor growth from each female constituted the material for the chromosome study. Bits of each growth were collected in hypotonic solution (0.075 M KCl) and subsequently processed for the preparation of the slides. One part of the excised tissue was immediately fixed in formalin for histopathological examination to the Pathology Department, Govt. Medical College, Jammu, and another part was transferred in a separate vial containing 0.0075 M KCl solution, and the same was transferred under strict aseptic condition to the Human Genetic Lab, SMGS Hospital, for the cytogenetic analysis. Cervical tissue of each patient collected in hypotonic solution was processed as follows:
The slides prepared by the in vivo technique were then processed for G-banding [10] with slight modifications. Karyotypes were prepared from some of the well-spread G-banded metaphase plates. Well-spread metaphase plates were selected in each case. Karyotypes were arranged manually and with the help of the software installed in the Automated Karyotyping Work Station (Olympus BX61). The chromosomes were paired following ISCN (1995) (International Seminar on Chromosome Nomenclature) [11] for further study. Results The present study was divided into two parts:
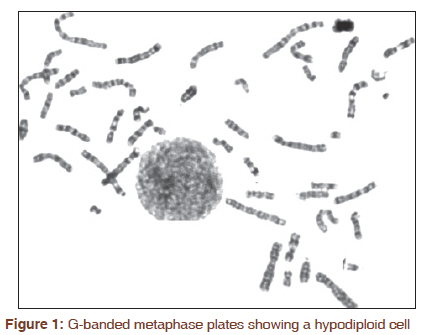
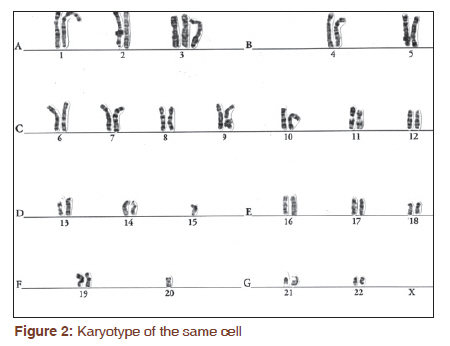
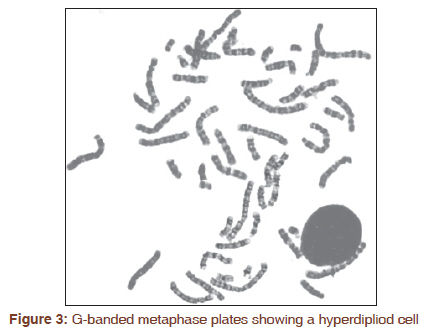
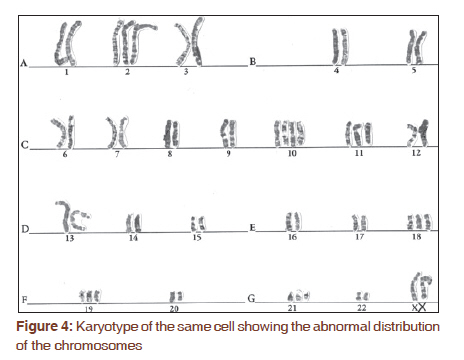
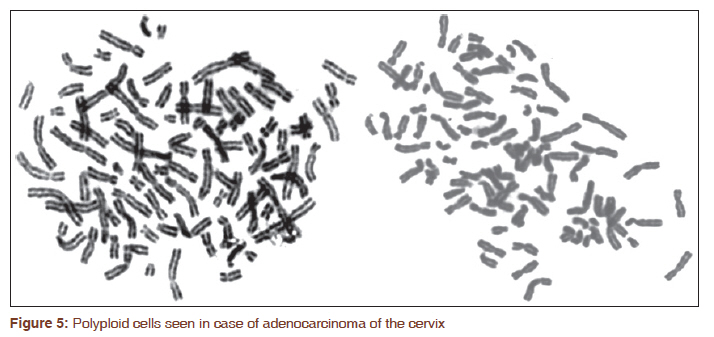
Cytogenetic A voluminous amount of the literature exists on the chromosomal changes in leukemia. But, the cytogenetic situation with solid tumors has lagged behind considerably. Leukemias constitute about 10% of the human neoplasia and make up the basis for more than 80% of available chromosomal data. A significant percentage of solid tumors have a very low mitotic index, necessitating culture of the cells, which may not be successful in all cases or may lead to overgrowth by normal (diploid) cells. The morphology of the chromosomes in solid tumors is more often fuzzy and less than optimal for detailed analysis than the cell morphology encountered in leukemias. During the present study, an attempt was made to obtain a more comprehensive picture of the histopathological type in pattern of chromosome number distribution by analyzing these cell populations according to their ploidy level. The modal range of the chromosomes was from 43 to 70 in case of SCC and from 45 to 92 in adenocarcinoma cases. In a majority of the metaphase plates, both the numerical and the structural chromosomal changes were recorded. Numerical chromosomal changes were comparatively more common (95%) than the structural changes (5%) [Figure - 1], [Figure - 2], [Figure - 3], [Figure - 4], and [Figure - 5]. Trisomy 3, 8, 11, 12, 13, 17, 18, 19, 20, 21 and 22 were the numerical changes recorded in SCC whereas monosomy of chromosome no. 3 and trisomy of chromosome 1, 3 and 17 were seen in the adenocarcinoma of the cervix. Besides chromosomal changes, micronuclei were also detected in both SCC and adenocarcinoma; however, the frequency of micronuclei was comparatively higher in the adenocarcinoma of the cervix. Non-cytogenetic findings Majority of the females in the present study (43.58%) were in the age group of 51-60 years [Table - 1]. Incidence of CaCx was higher (46.15%) in the females who were Para five or above [Table - 1] 84.61% females belonged to rural areas and only 15.38% belonged to an urban area [Table - 1] Females hailing from Hindu families showed a higher incidence of CaCx [Table - 1] Nearly 50% of the females in the present study got married at the age between 16 and 20 years [Table - 1] 35.89% of these females had first conception below 18 years of age [Table - 1]. Factors like multiple sexual partners, smoking, alcohol consumption and use of oral or barrier contraceptives were doubtful and, therefore, these were not considered during the present study. Discussion Conventional cytogenetic analysis is a powerful tool, established technique that can provide a picture of the human genome at a glance. Most laboratories use G-banding using Trypsin and Giemsa stain (GTG-banding) for conventional cytogenetic analysis. Chromosomal aberrations in cervical cancer have been extensively characterized by cClassical Cytogenetic. During the present study, numerical chromosomal changes, especially trisomy 1, 3 and 17, remained to be frequent in both the SCC of the cervix and the adenocarcinoma of the cervix. Our findings on the numerical chromosomal changes are by and large similar to those of the earlier reports. [12],[13] Chromosomal instability, as manifested by an increase in aneuploidy and structural chromosomal changes, is believed to play a critical role in the intermediate to late stages in the development of cervical malignancies. [14] Aneuploidy and tetraploidy have earlier been reported in women diagnosed with pre-cancerous and cancerous cervical lesions. The presence of elevated levels of trisomy and aneusomy in the cervical carcinomas recorded during the present study are consistent with the previous findings. [15],[16] Carcinogens affect the cells by altering genetic material and thus causing instability. Chromosomal instability, manifested by increased aneuploidy and structural chromosomal aberrations, is believed to play a critical role in the intermediate to late stages of the development of cervical malignancies. [17] Chromosomes or chromosome segments that fail to be incorporated into nuclei during cell division configure micronuclei. Thus, micronuclei represent a measure of both chromosome breakage and chromosome loss and can function as a sensitive indicator of genetic damage. [18] The formation of micronuclei in the dividing cells could be the result of chromosomal breakages due to unrepaired or misrepaired DNA lesions, or chromosome malsegregation due to mitotic malfunction. These events may be induced by oxidative stress, exposure to clastogens or aneugens, genetic defects in cell cycle checkpoint and/or DNA repair genes as well as deficiencies in nutrients required as co-factors in DNA metabolism and chromosome segregation machinery. [19] All these events can cause the formation of micronuclei through chromosomal rearrangements, altered gene expression or aneuploidy effects associated with the chromosome instability phenotype often seen in cancer. [20],[21] Genetic changes in the form of the micronuclei have also been reported in case of cervical cancers by workers like (Widel et al, 2001 & Gandhi et al, 2005. [21],[22] The number of micronuclei MN correlates with the severity of the genetic damage. Cells containing several MNs present greater genetic damage than do cells that present only one MN. In the present study, it was found that the number of micronuclei increased with the severity of the cervical cancer. It was observed that the number of micronuclei was higher in the higher grades of cervical cancer (I < II < III < IV stages). Our results were in accordance with the studies conducted by Campos et al, 2008. [23] This evidence shows the importance of the MN test as a biomarker for malignancy. A study by Guzman et al, [24] showed an association between lesion severity and MN frequency in epithelial cells, which contributes toward validating MN frequency as a possible biomarker for cancer risk. Probable risk factors like early marriage, multiparity socioeconomic status, etc. associated with the development of cervical carcinoma detected in the present study have also been analyzed. Carcinoma of the cervix is reported to be more common in females in the age group of 51-60 years. [25],[26] Present findings on the age factor are akin to the earlier reports. Although cancer of the cervix can develop in women of all ages, it usually develops in women aged 35-55 years, with the peak age for incidence varying with populations. [27] In India, the peak age for cervical cancer incidence is 45-54 years [Table - 1]. The incidence of CaCx is higher among the multiparous females (Para 5 or above). [28],[29] Similar observations have been made during the present study. Pregnancy may produce some dysplastic lesions of the cervix, which regress, persist or progress to carcinoma. Pregnancy could exert an adverse effect on cervical cancer. Trauma to the cervix is one of the possible explanations that warrant explorations, including increased susceptibility to infection through immunosuppression, hormonal influence and dietary deficiencies. [30] However, the linkage of multiparity with CaCx needs to be worked out further for making the final conclusion. Females from the rural background have been found to have a higher incidence of CaCx. In the present study, 84.61% of the patients were from the rural areas [Table - 1], suggesting, thereby, that CaCx largely affects the females from rural areas. Similar observations have been made earlier. [31] In rural areas, women′s health problems are often linked to nutritional deficiencies, excessive workload and frequent pregnancies coupled with inadequate prenatal and birth care. The primary reason given for this is lack of access to screening and health services and lack of awareness of the risk factors of cervical cancer. HPV infection and precancerous lesions go unnoticed and develop into full-blown cancer before women realize that they need to go for medical help. [32] Religion has been associated with CaCx. All the 78 females in the present study were Hindus. The incidence of cervical malignancy has been reported to be lower in the Muslim women. The present findings [Table - 1] have been found to be similar with the earlier reports. Circumcision, as practiced by the Muslim, is believed to be the preventive factor that accounts for the lower incidence of cervical carcinoma as compared with that in the Hindu community. [33] The incidence of cervical cancer has also been studied by various workers in case of the Muslim population, such as Bhurgi et al., 2007, Howyada et al., 2007 & Yasmeen et al., 2010. [34],[35],[36] Yasmeen et al. conducted a study with the aim of finding the prevalence of cervical cancer in a rural ethnically Muslim community of the state of J and K, which is the first community-based screening done for cervical cancer in Kashmir. The frequency of this malignancy has been found to be higher in the females who got married between 16 and 20 years of age [Table - 1]. Our findings are consistent with the earlier reports. 37 Early age at marriage indicates an early exposure to sexual activities and early pregnancy, which are well-known etiological factors for cancer cervix. These factors result in a longer duration of married life, with greater opportunities for sexual activities and increased chances of becoming pregnant. According to Varghese (2004), carcinoma of the uterine cervix is predominantly a disease of married women, especially occurring in those who marry at an early age and have a long, active sexual life. Chromosome analysis in a tumor tissue may provide an additional tool for the diagnosis of the tumor; however, cytogenetic study if supplemented with fluorescent in situ hybridization will aid further in pinpointing the exact location of the gene/genes involved in the origin and progression of the tumor. Present work is an addition to the existing literature on the study of cervical carcinoma. To determine the role of chromosomal changes in the origin and progression of cervical carcinoma and also to make a correlation of the non-cytogenetic factors with the cervical carcinoma, further studies are required. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11073f4.jpg] [cr11073f1.jpg] [cr11073f3.jpg] [cr11073t1.jpg] [cr11073f5.jpg] [cr11073f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}