 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
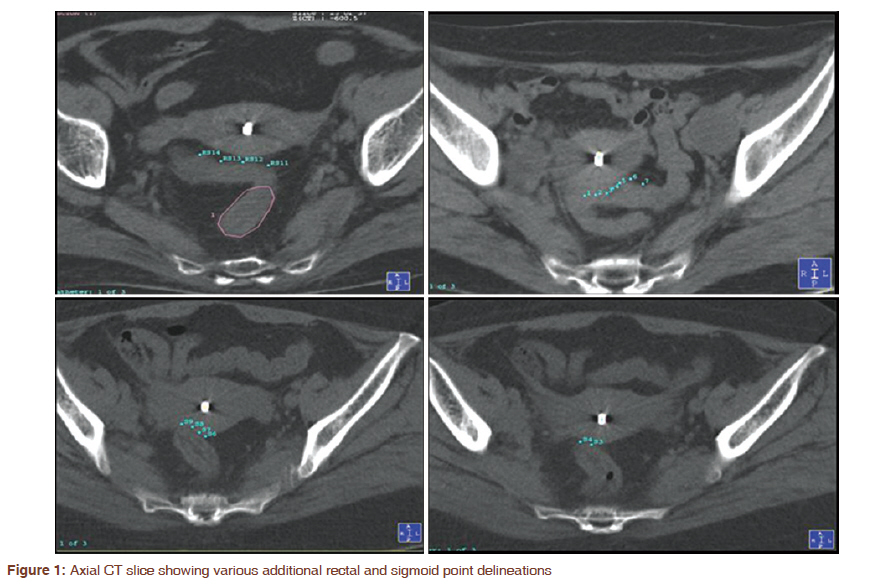
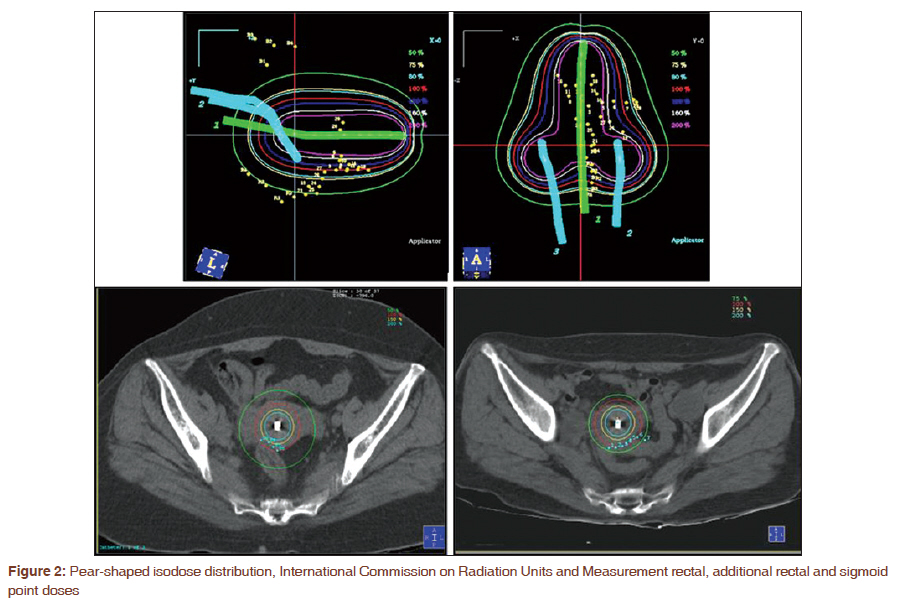
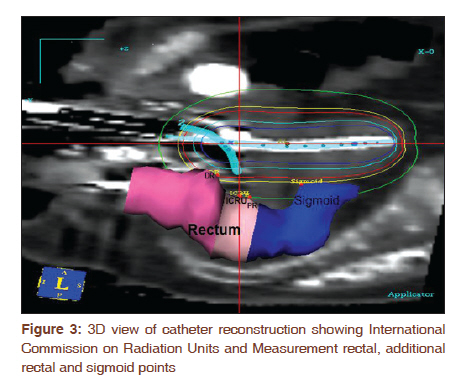
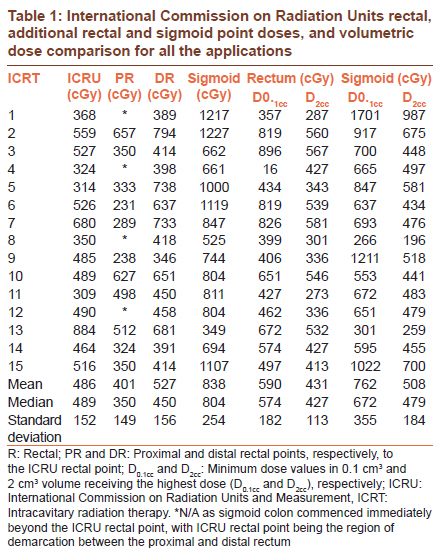
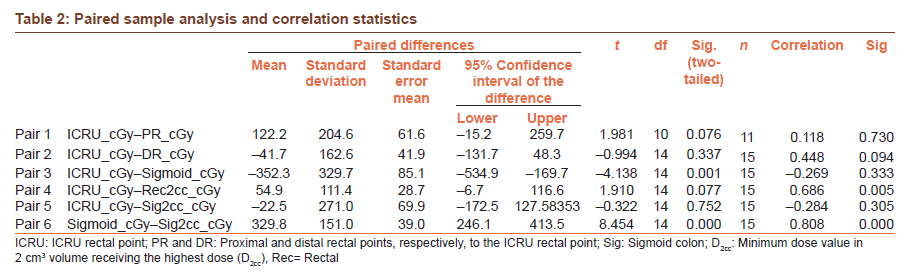
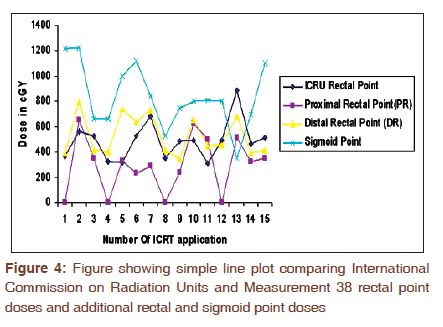
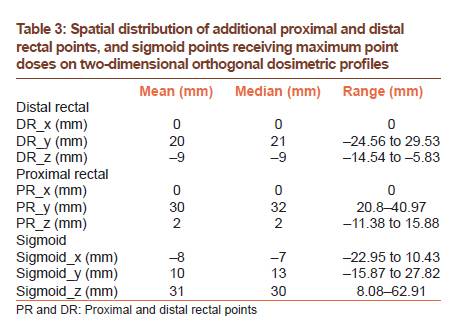
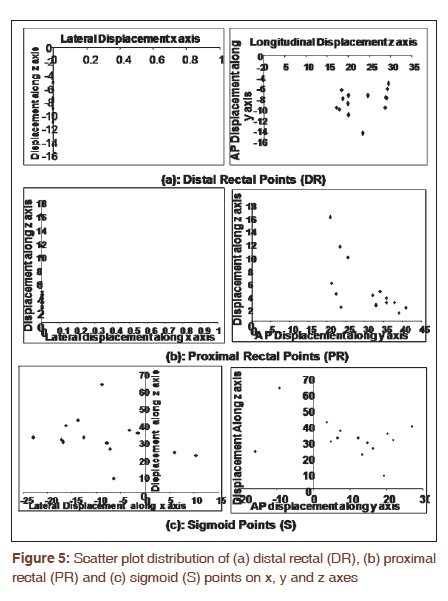
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 298-303 Original Article Additional rectal and sigmoid mucosal points and doses in high dose rate intracavitary brachytherapy for carcinoma cervix: A dosimetric study Umesh Mahantshetty1, Manpreet Singh Tiwana1, Swamidas Jamema2, Sanjib Mishra1, Reena Engineer1, Deepak Deshpande2, Shyamkishore Shrivastava1 1 Department of Radiation Oncology, Tata Memorial Hospital, Mumbai, India PMID: 22044811 DOI: 10.4103/0973-1482.87027 Materials and Methods : Fifteen high dose rate intracavitary brachytherapy (ICA-HDR) applications with conventional X-ray and computed tomography (CT) based planning were studied. In addition to International Commission on Radiation Units and Measurement (ICRU) rectal and bladder points, proximal and distal rectal and sigmoid points were digitized on CT scans and dose volume histograms' (DVHs') parameters were computed and correlated. Results: The mean ICRU, additional distal, proximal and sigmoid point doses were 486 ± 152 cGy, 527 ± 156 cGy, 401 ± 149 cGy and 838 ± 254 cGy, respectively, for a prescription of 700 cGy to point A. The mean sigmoid point dose was significantly higher than the ICRU rectal point doses (P=0.001). The high-dose sigmoid points were situated at a mean -8 mm (range -22.95 to 10.43 mm) lateral, 10 mm posterior (range -15.87 to 27.82 mm) and 31 mm (range 8.08-62.91 mm) cranial to the intracavitary applicator flange of central tandem. Conclusions : Our dosimetric study suggests that sigmoid points and 0.1 cm 3 receive significantly higher doses than rectal points during ICA-HDR in carcinoma of the uterine cervix. No definite conclusion on reproducible spatial distribution on orthogonal X-rays could be achieved. To document and reduce sigmoid doses, some form of 3D image-based planning is necessary. Keywords: Additional proximal and distal rectal point/s, dose volume parameters, high dose rate intracavitary brachytherapy, International Commission on Radiation Units and Measurement 38, rectal point, sigmoid points Introduction Carcinoma of the uterine cervix is the most common cancer in females. The mainstay of treatment is combined external beam radiotherapy (EBRT) and intracavitary brachytherapy (ICA), especially in the advanced stages. [1] Brachytherapy forms an integral part of radiation therapy and cornerstone for both the local control rates and toxicities. The International Commission on Radiation Units and Measurement 38 (ICRU 38) recommendations have been followed universally by the oncology community for uniform reporting of ICA. [2] Assessment and planning of ICA in routine clinical practice continues to be dominated by orthogonal film dosimetry defined points, with point A corresponding to the tumor and the rectal and bladder points defining the dose distribution to critical structures. [3] Patients with symptomatic grade III radiation proctitis and cystitis are difficult to manage, and to date no standard treatment guidelines are available. So, it is imperative to identify and modify parameters, which directly predict or correlate with late toxicities in long-term survivors. In the past, there have been many reports critically reviewing and challenging the ICRU 38 recommendations. [4],[5] The advent of better imaging modalities and technological advances in the last two decades have paved the way for image-based brachytherapy, but logistics, conventional mindset and resource implications have been the major hurdles against its routine clinical application today. The incidence of mild to severe late rectal toxicities ranges from 5 to 30% in high dose rate brachytherapy (HDR) series. [6] This is dependent on doses to rectal point/s and the incidence is higher when the doses delivered are more than 100 Gy (BED). [7] However, despite rectal doses within tolerance limits and reduction in brachytherapy doses, many patients still develop symptomatic radiation proctitis. Endoscopy in these patients invariably shows telangiectasia or ulceration of rectal/recto-sigmoid mucosa of varying grades. [8] These changes are usually seen at a higher level than the ICRU 38 rectal point/s, challenging the conventional point-based ICA dosimetry practice. [9] This encouraged us to study and review our ICA dosimetry planning strategy and this report is one such attempt. We identified additional rectal and sigmoid points and document doses to these points on computed tomography (CT) based ICA-HDR brachytherapy planning which forms the basis of this report. Materials and Methods Patients Patients with stage IIB (three patients) or IIIB (four patients) cervical cancers treated with radical radiation therapy and HDR brachytherapy were studied. A total of 15 ICA-HDR applications that had undergone both conventional orthogonal X-ray and CT based planning were selected and studied. The external radiation and ICA-HDR doses were planned according to the stage and as per the institutional management protocols. [10] The external radiation doses ranged between 45-50 Gy and 1.8-2.0 Gy per fraction, followed by 3-5 fractions of ICA-HDR depending on the International Federation of Obstetrics and Gyneacology (FIGO) stage. Each ICA-HDR procedure was performed using Standard Fletcher Williamson Applicator (Nucletron, Veenendaal, The Netherlands) under short general anesthesia. Routine orthogonal radiographs were taken for planning and treatment. Planning was done conventionally and dose was prescribed to point A with 7 Gy per fraction (21 - 35 Gy in 3-5 fractions). The doses to ICRU 38 rectal and bladder points was documented. Orthogonal radiograph based (two-dimensional) dosimetry All the patients were treated with a conventional radiography based treatment plan. On the orthogonal films, the dose points (point A, bladder and rectal points) were defined by the ICRU 38 recommendations, and the respective point digitization and brachytherapy planning was done using Sunrise Plato Planning System (Nucletron). The doses to the ICRU 38 rectal and bladder points were documented as percentages of the prescribed dose to point A. The dose prescribed was 700 cGy to point A per fraction every week for 3-5 fractions depending on the stage. The dose prescription was modified/reduced according to the rectal and bladder point doses. Computer tomography based dosimetry The CT-based (Somatom, Emotion, Siemens) planning protocol consisted of 3-5 mm axial slices of the pelvis to include the tandem superiorly and anal verge inferiorly. To reduce the artifacts caused by the non-CT compatible metal applicators, the images were transferred with appropriate CT window and level settings to the treatment planning system. Treatment planning was carried out on 3D PLATO Brachytherapy V 14, (Nucletron). After catheter reconstruction, for each application, the corresponding optimized dwell positions and dwell times used in 2D planning were duplicated for 3D planning and conventional planning was done as described above. The external contour of the organs at risk (OAR), viz. rectum and sigmoid in the pelvis, was delineated on each CT slice in the 3D PLATO Brachytherapy Treatment Planning System. In addition to the ICRU 38 recommended rectal and bladder points, additional proximal and distal rectal and sigmoid points in the high-dose regions on dose volume histogram (DVH) and in close proximity to the uterus were digitized randomly on each axial CT slice [Figure - 1]. Of all these points, the maximum dose point/s were identified, compiled and compared. The dose volume parameters (DVH) of all the OAR according to GEC-ESTRO recommendations were calculated and compared to the ICRU 38 and additional rectal and sigmoid points [Figure - 2]. [6] Spatial distribution of additional rectal and sigmoid points An attempt was made to identify the most commonly appearing high-dose region points in rectal (other than ICRU point) and sigmoid regions and document their spatial distribution in relation to the flange (at the level of external os) [Figure - 3]. The locations were tabulated in x, y and z axes, with the applicator flange as the origin of these three axes. The x axis represents left (+) or right (-) of the applicator central axis, the y axis denotes posterior (+) or anterior (-) to the uterine tandem, while the z axis represents cranial (+) or caudal (-) to the applicator flange. Statistical analysis Statistical analysis was done using SPSS 15.0 software package (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to calculate the mean, median and standard deviation of the ICRU rectal, the additional rectal and sigmoid point doses. Paired sample statistics (two-sided t-test) were used to compare the doses calculated to the above-mentioned points. They were correlated to the rectum D 2cc and sigmoid D 2cc volumes generated through three-dimensional CT-based planning. Results All 15 ICA-HDR applications had both conventional and CT-based planning done. Since the dose (700 cGy) was normalized and prescribed to point A, the pear-shaped distributions were identical in conventional and CT-based planning. International Commission on Radiation Units and Measurement rectal and additional rectal and sigmoid point correlation The mean ICRU rectal point dose was 486 ± 152 cGy (median 489 cGy; 309-884 cGy), mean proximal (PR) and distal rectal (DR) point doses were 401 ± 149 cGy (median 350 cGy; 231-657 cGy) and 527 ± 156 cGy (median 450 cGy; 346-794 cGy), respectively, for a prescription of 700 cGy to point A. The mean ICRU rectal point dose did not significantly differ from the PR and DR point doses (P=0.076 and P=0.337, respectively). However, the mean sigmoid point dose of 838 ± 254 cGy (median 804; 349-1227 cGy) was significantly higher than the ICRU rectal point doses (P=0.001), the PR (P=0.000) and DR point doses (P=0.000). [Table - 1] and [Table - 2] illustrate the comparison between ICRU rectal, PR, DR and sigmoid points, and their paired sample analysis, respectively. Further, a line chart of various point doses comparing ICRU rectal with the additional rectal (PR and DR) and sigmoid points is shown in [Figure - 4]. The plot clearly suggests significantly higher sigmoid point doses in 14 of 15 (93%) intracavitary applications as compared to the rectal points. Comparison of International Commission on Radiation Units and Measurement rectal and volumetric doses of rectum and sigmoid [Table - 1] shows the comparison between the point dose and volumetric doses of the OAR being studied. The mean ICRU rectal point dose of 486 ± 152 cGy (median 489 cGy; 309-884 cGy) did not differ significantly from the mean D2cc rectal doses of 431 ± 113 cGy (median 427 cGy; 273-581 cGy) and mean D2cc sigmoid doses of 508 ± 184 cGy (median 479 cGy; 196-987 cGy) (P=0.07 and P=0.752, respectively). However, the mean sigmoid point dose of 838 ± 254 cGy was significantly higher than the mean D2cc sigmoid dose of 508 ± 184 cGy (P=0.000) and the mean ICRU rectal point dose (P=0.02), but was comparable to 0.1 cm3 doses of 762 ± 355 cGy (median 672 cGy, 266-1701 cGy). In our volumetric dosimetry analysis, sigmoid was the most frequent organ receiving the higher D2cc dose in 9 of 15 (60%) ICA-HDR applications, while rectum followed in the remaining 6 of 15 ICA-HDR (40%) applications. [Figure - 2] and [Figure - 3] show a portion of the sigmoid receiving higher point and volumetric doses compared to the rectum. Spatial distribution of additional rectal and sigmoid points In an attempt to define the high-dose point regions with respect to the ICA-HDR applicator, we compiled and extracted these points receiving maximum dose for proximal rectal (PR), DR and sigmoid for each application [Table - 3]. The exact geometrical location of these points with reference to the flange of the uterine tandem was estimated from the planning system and scatter plot generated [Figure - 5]. The additional DR points were located in the median position without any lateral displacement, 20 mm (mean) (range -24.56 to 29.53 mm) posterior to the applicator axis and -9 mm (range -14.54 to -5.83 mm) caudal to the flange of uterine tandem. Similarly, the additional PR points were situated within a mean of 30 mm (range 20.8-40.97 mm) posterior to the uterine axis and 2 mm (range -11.38 to 15.88 mm) cranial to the flange without any lateral displacement, while the sigmoid points were at a mean of -8 mm (range -22.95 to 10.43 mm) lateral, 10 mm (range -15.87 to 27.82 mm) posterior and 31 mm (range 8.08-62.91 mm) cranial from the applicator flange. Discussion Although ICRU 38 recommendations have been followed universally by the community for uniform prescribing and reporting of ICA, [2] there have been many reports critically reviewing and challenging the ICRU 38 recommendations for ICA in cervical cancer. [4],[5] As detailed in the section "Introduction," the late radiation changes in the rectal mucosa are at a higher level than the ICRU 38 rectal points, challenging further the validity of conventional point-based ICA dosimetry practice for predicting toxicity. Post-radiation endoscopic changes are routinely visualized in areas of high-dose region proximal to the traditional rectal points. [8] Radiation-induced recto-sigmoid complications graded according to the system based on SOMA scales do not distinctly define the injured site, whether rectum or sigmoid. [9] This encouraged us to study and review ICA dosimetry planning and this report is one such attempt. In an effort to identify additional dosimetric points which may better forecast rectal complications on CT-based ICA-HDR brachytherapy planning, we undertook this study. In our study, we tried to identify additional set of proximal (PR) rectal, DR and sigmoid points, apart from the ICRU reference point and correlated them with GEC-ESTRO dose volume parameters. The mean ICRU rectal point dose did not significantly differ from the PR and DR point doses (P=0.076 and P=0.337, respectively). However, the mean sigmoid point dose was significantly higher than the ICRU rectal point doses (P=0.001), the PR (P=0.000) and DR point doses (P=0.000). This pattern can be explained by the relative fixed anatomy of rectum and close anatomical proximity of sigmoid to the intrauterine sources, as evident in [Figure - 2] and [Figure - 3]. The sigmoid point doses were higher in more than 90% of the applications, suggesting a need to optimize the ICA plans to reduce sigmoid doses. Further, these point doses were correlated with GEC-ESTRO dose volume parameters for rectum and sigmoid for better understanding and dosimetric correlation. Several investigators have clearly demonstrated that OAR like rectum and sigmoid volume doses are significantly higher than the ICRU reference point estimate doses. [5],[11] Similarly, in our study, the mean ICRU rectal point dose of 486 ± 152 cGy did not differ significantly from the mean D2cc rectal doses of 431 ± 113 cGy and mean D2cc sigmoid doses of 508 ± 184 cGy (P=0.07 and P=0.752, respectively). But the mean sigmoid point dose of 838 ± 254 cGy was significantly higher than the mean D2cc sigmoid dose of 508 ± 184 cGy ( P = 0.000). We also attempted to identify the exact location and reproducibility of these sigmoid points in relation to the flange for extrapolation to orthogonal radiographs. In our dosimetric analysis, the sigmoid points were at a mean of -8 mm (range -22.95 to 10.43 mm) lateral, 10 mm (range -15.87 to 27.82 mm) posterior and 31 mm (range 8.08-62.91 mm) cranial from the applicator flange. But the wide variation [Figure - 5] and no specific reproducible point limits our endeavor to extrapolate these on orthogonal planning radiographs. Identification of these sigmoid points on conventional orthogonal X-rays still remains a challenge. None of the reports in the literature address the issue of sigmoid points, their doses and spatial distribution on X-ray based dosimetric studies although it has been addressed to some extent by DVH parameters and clinical outcome recently. [12],[13] There is no literature addressing the issues of sigmoid motion, its impact on brachytherapy dosimetry and correlation with late effects. More number of applications and mature clinical data in the future may result in defining the sigmoid points. To validate our findings of high doses to these additional rectal and sigmoid points, we are doing a retrospective analysis of detailed endoscopic findings of patients with grade III radiation proctitis and ICA planning details. Conclusion Our dosimetric study suggests that ICRU rectal point doses correlate with additional rectal points and 2 cm3 rectal doses during high-dose rate ICA in carcinoma of the uterine cervix. Sigmoid points receive significantly higher doses. No definite conclusion on reproducible spatial distribution on orthogonal X-rays could be achieved. To document and reduce sigmoid doses, some form of 3D image based planning for ICA-HDR is necessary. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11075f1.jpg] [cr11075t2.jpg] [cr11075f2.jpg] [cr11075f5.jpg] [cr11075f3.jpg] [cr11075t3.jpg] [cr11075f4.jpg] [cr11075t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}