 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
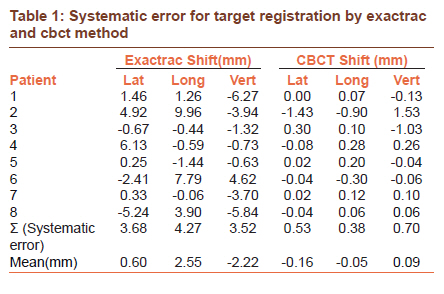
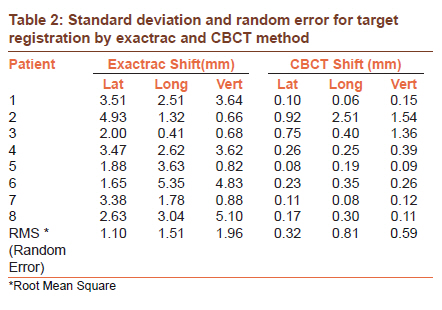
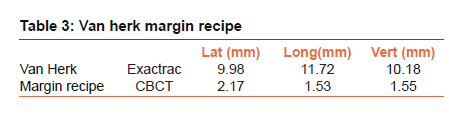
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 304-307 Original Article A comparative study to evaluate the efficacy of on board imaging with cone beam CT using target registration in patients with lung tumors undergoing stereotactic body radiation therapy and comparison with ExacTrac using skeletal registration on Novalis Tx Thomas S Ram1, Rajeev Badkul2, Sanjay Maraboyina2, Fen Wang2 1 Department of Radiation Oncology, Unit 1, Christian Medical College, Vellore, Tamil Nadu, India PMID: 22044812 DOI: 10.4103/0973-1482.87029 Aim: To evaluate the efficacy of ExacTrac and Cone Beam Computed Tomography (CBCT) for target repositioning while delivering Stereotactic Body Radiation Therapy (SBRT) for lung lesions and derive the population-based margin. Materials and Methods: All patients who had undergone SBRT for lung lesions from February to September 2009 were involved. Patients were immobilized using the BodyFix double vacuum immobilization system, indexed to the computed tomography (CT) simulator and treatment machine. Four-dimensional (3-D) scan was done to generate internal target volume (ITV) and a free breathing CT scan for planning was done on the BrainLab iPlan 4.1 software. During treatment, patient's position was verified using ExacTrac and CBCT. The resulting vertical, lateral, and longitudinal shifts were noted. The random and systematic error were calculated and the margin recipe derived using the Van Herk formula. Results: Sixteen patients had undergone SBRT for lung tumors from February to September 2009. Data from eight patients who had undergone 34 sessions of SBRT was analyzed. The systematic error for lateral, longitudinal, and vertical shifts for ExacTrac and CBCT were 3.68, 4.27, 3.5 mm and 0.53, 0.38, 0.70 mm, respectively. The random error were 1.10, 1.51, 1.96 mm and 0.32, 0.81, 0.59 mm. The lateral, longitudinal and vertical Van Herk margin recipe for ExacTrac were 9.98, 11.72, 10.18 mm, respectively, and for CBCT was 2.17, 1.53,1.55 mm. Conclusions: The systematic and random errors for CBCT were significantly lesser as compared to the errors with Exactrac. Keywords: Cone beam computed tomography, exactrac image guided radiotherapy, lung tumors, margins radiotherapy, set up error, stereotactic body radiation therapy
Introduction Lung cancer is a major health problem not only in North America and developed countries, but also in the developing countries. This is directly an implication of high prevalence of smoking and tobacco use. The age-adjusted male and female invasive cancer incidence rates of lung cancer in US is 68.1 per 100 000, [1] and is projected to be 222 000 overall cases in 2010. [2] With the increasing use of CT screening and 88% 10-year survival reported among patients with screen-detected stage I lung cancer in the international Early Lung Cancer Action Program screening study, there will be an increasing number of lung cancer diagnosed early and presenting early for the treatment. [3],[4] However, deaths due to lung cancer will be still the leading cause of cancer death according to American Cancer Society statistics for 2009. [5] Surgery remains the standard of care for Stage I/ II nonsmall cell lung cancer. According to the revised staging as proposed by the International Association for Study on Lung Cancer (IASLC) the 5-year survival rates for pT1 <2 cm is 77%; pT1 >2 cm but <3 cm is 71%; pT2 > 3 cm but < 5 cm 58%; pT2 > 5 cm, but < 7 cm is 49% and pT2 > 7 cm 35%. [6] There are about 20% of patients with early-stage lung cancer who are medically inoperable. [7] The reasons for inoperability could be poor pulmonary compliance, cardiovascular disease, or poor performance status. These patients though technically operable, are considered medically inoperable and some who refuse radical surgery. Such patients are often referred for radical radiotherapy. Conventional radiation therapy always had inferior results with regard to local control as compared to surgery. This could be due to the sub ablative doses prescribed in conventional radiation therapy. The dose prescription is more often guided by the dose constraints of the surrounding normal structures rather than ablative doses necessary for the target lesion. According to a Cochrane systematic review on radical radiotherapy for stage I/II nonsmall cell lung cancer in medically inoperable patients the 2-year survival was superior following continuous hyperfractionated accelerated radiotherapy (CHART) (37%) compared to conventional 60 Gy in 30 fractions over 6 weeks (24%), while cancer-specific survival was between 54-93% at two years, 22-56% at 3 years, and 13-39% at 5 years. [8] With the improvement in technology and the ease of its availability and accessibility radiation oncology practice has undergone a significant improvement. Modern treatment units have now made it possible to deliver ablative dose to the target and at the same time keep the dose to the surrounding normal tissue within their tolerance limits. Stereotactic body radiation therapy (SBRT) is one of the recent technological innovations, initially developed at Sweden. [9] Since then it is increasingly being used in various centers across the world. SBRT uses very high doses of radiation in a single fraction or multiple hypofractionated schedules ranging from 3, 5, or more fractions. It uses multiple noncoplanar or coplanar beams, which is guided by a 3-D stereotactic co-ordinate system. Currently it is been widely used in various extra cranial sites such as spine, [10] liver, [11] retroperitoneal space, [12] pelvis, [13] and Lungs. [14] As SBRT requires very precise target definition and tight margins, the validation of repositioning of the patient is very crucial. Usually a CT scan is done just before the treatment delivery to verify the target position. In centers where CT is not an option orthogonal radiograph is taken for verification. There are treatment units which are capable of imaging directly on the treatment couch which enables not only to verify the tumor location, but also correlates the target with the treatment reference coordinates as derived from the planning system. Some of such units are cone-beam CT attached to the gantry, [15] tomotherapy, [16] and CT on rails. [17] With the improvement in onboard imaging on the treatment units, it is now becoming possible to deliver high-dose per fraction to lung lesions. The accuracy and reproducibility of the treatment has enabled the physicians to prescribe and deliver ablative doses to smaller lesions in the lung. However, this technology needs to be used with caution, as it is relatively new. Data on follow-up is being reported, side effects such as rib fracture, and chest wall pain following SBRT to peripheral lesions is noted. [18] SBRT for medically inoperable early stage lung cancer is being widely practiced in more and more academic centers in various countries like Japan. [19] With encouraging results for local control and clinically acceptable toxicities, the role of SBRT will be expanding in the coming years. While the technology will be readily available and utilized, a strict quality assurance protocol will be of uttermost importance to make the facility a success. As various onboard imaging modalities are available, more are evolving there need to be a consensus among at the users of having an optimal verification protocol established. Since SBRT is being used in this institution, it has been a policy to use both ExacTrac and CBCT for patient verification. This study will be evaluating the efficacy of both cone-beam CT and ExacTrac on board imaging devices in delivering SBRT for lung tumors. It will provide a baseline assessment of the current practice and give the direction to develop an optimal OBI protocol in treating lung lesions with SBRT. Materials and Methods This study was a retrospective cohort study evaluating the efficacy of on board imaging using CBCT and ExacTrac coupled to Novalis treatment unit, in SBRT of lung lesions and deriving the margin recipe. Eligibility criteria All adult, both male and female, patients between the age group of 18-75 years with medically inoperable Stage I/II primary lung cancer and lung secondaries that are <5 cm treated with lung SBRT from Feb 2009 to Sept 2009 were included. Simulation and planning Patients were immobilized in supine position with arms above the shoulder using a Body Fix double vacuum immobilization system (Medical Intelligence, Germany) which was indexed to the CT simulator and treatment machine. All patients included in this study underwent a 4-D simulation on a Philips CT simulator to generate ITV and a free breathing CT scan for planning. Planning was done on a BrainLab iPlan 4.1 software. The target and normal structures were delineated and then a stereotactic plan using multiple co-planar or noncoplanar beams was generated by optimizing the beam weight and the aperture. The Gross Tumor Volume (GTV) was delineated as visualized on the CT lung windows, if available the GTV seen on PET and with the GTV derived from all ten phases of respiratory cycle thus rendering a final GTV internal Target volume. Image-guided radiation therapy process After the patients were immobilized in the Body Fix system, the initial setup was done using the tattoo on the patient. The external fiducial were then fixed on the patient′s chest wall at predetermined site. The fiducials were automatically matched with the position of fiducials generated from the planning CT scan thus producing the first shift for the ExacTrac. However, the skeletal registration is verified by a physician and if required some minor shifts are done manually before registering. Once the fiducials were matched, ExacTrac was then utilized to capture the orthogonal x-rays. These were then used to do bone registration based on the DRR-generated from planning CT. The vertebrae closest to the target were considered for bone registration. This matching produced a shift from the matching done using the fiducials. Once the bone registration is satisfactory, a CT was done using the on board CBCT on the treatment unit. The CT images were then used to accomplish the target/soft tissue registration, which also produced couch shift. The 3-D couch shifts using bone and target registration with CBCT and ExacTrac were documented for all the patients. From these values the mean, standard deviation of systematic error and random error were calculated. The random and systematic error was then used to calculate the population based margins using the Van Herk formula. [20] Results Sixteen patients had undergone SBRT for lung tumors from February to September 2009. Data of eight patients who had undergone 34 sessions of SBRT was taken for analysis. The systematic error for lateral, longitudinal, and vertical shifts for ExacTrac and CBCT were 3.68, 4.27, 3.5 mm and 0.53, 0.38, 0.70 mm, respectively, [Table - 1]. While the random error were 1.10, 1.51, 1.96 mm and 0.32, 0.81, 0.59 mm [Table - 2]. Based on the errors the lateral, longitudinal, and vertical Van Herk margin recipe derived for ExacTrac was 9.98, 11.72, and 10.18 mm, respectively, and for CBCT was 2.17, 1.53, and 1.55 mm, respectively, [Table - 3]. Discussion This was a preliminary study that we undertook to evaluate the efficacy of two onboard image-guided therapy methods the ExacTrac and CBCT. The first method used was the bone registration method (ExacTrac) while the second one used was the target registration method (CBCT). Our data for ExacTrac concurred with earlier published studies, which reported target positional errors upto 10-20 mm. [21] The margin recipe for the local patient population was also derived using the Van Herk formula, which suggested that we could provide narrow margins when CBCT is used for target registration. CBCT-based soft tissue registration may be more appropriate for peripheral lesions as there is more chance of target mobility. While for the centrally located lesions matching with spine may suffice as there is not much movement expected. However, this hypothesis needs to be tested in a larger number of patients undergoing SBRT. Further, subvariate analysis of the site of tumor, distance of lesion from midline and comorbid pulmonary conditions may help to develop further guidelines on choosing the appropriate target verification systems. Repositioning and target registration data of ExacTrac and CBCT from various centers offering SBRT and using a similar immobilization protocol can be compared to develop local margin recipes for such lesions. Such a larger series will perhaps give a better estimate of the systematic and random error of the two methods. With the encouraging results of SBRT for operable early stage lung cancer a randomized control trial, comparing SBRT versus radical surgery will be an interesting alternative for patients who are not keen for surgery for personal reasons. However, SBRT is still evolving and there is a need to develop stringent protocols and have a regular and long follow up of these patients. Translational research identifying the molecular markers of response and toxicity will be useful in choosing the appropriate patients who will benefit from this therapy. Data on acute and late effects of SBRT needs to be documented and analyzed to evaluate the clinical efficacy of this modality. Conclusions Our findings suggest that for SBRT of lung lesions, which are considered soft tissue targets, skeletal registration with a system like ExacTrac, or soft tissue target registration with onboard CBCT can be utilized as an acceptable target verification systems. However, when treatment delivery involves high doses per fraction with minimum errors, soft tissue target registration with CBCT should be considered more appropriate. CBCT not only will improve the target verification but also allow for narrower margins and improve the therapeutic index. Acknowledgements This work was possible because of the CMC-Kansas Modale Fellowship Program initiated between Christian Medical College, Vellore, India and Kansas University Medical Center, Kansas City, KS, USA. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11076t3.jpg] [cr11076t1.jpg] [cr11076t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}