 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
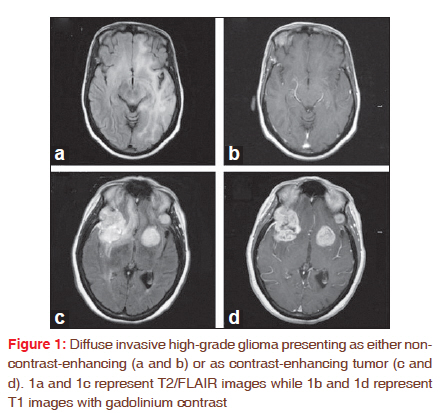
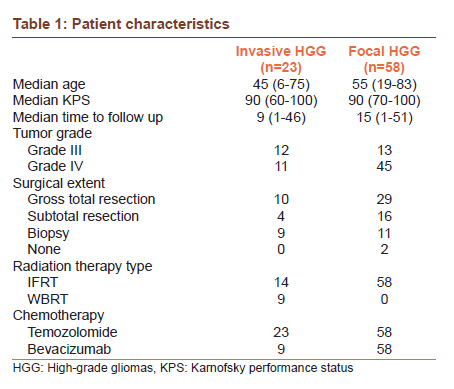
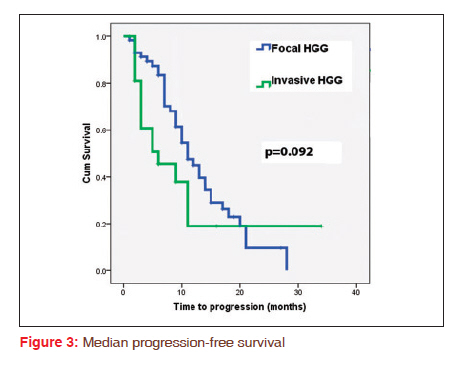
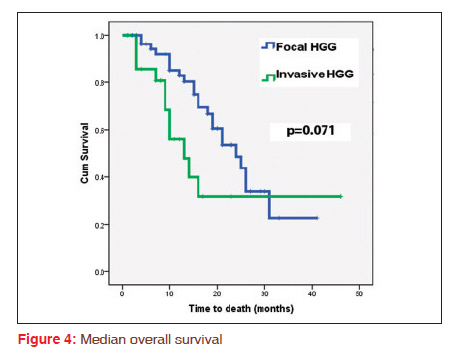
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 331-335 Original Article Invasion is not an independent prognostic factor in high-grade glioma Ashwatha Narayana1, Donato Perretta2, Saroj Kunnakkat2, Deborah Gruber3, John Golfinos4, Erik Parker4, Praveen Medabalmi5, David Zagzag6, RN Pat Eagan3, Michael Gruber3 1 Department of Radiation Oncology and Neurosurgery, New York University Langone Medical Center, New York, NY 10016, USA PMID: 22044816 DOI: 10.4103/0973-1482.87039 Materials and Methods: Twenty-three patients presented as newly diagnosed diffuse invasive HGG. All patients underwent surgical resection with radiation therapy and temozolomide for one year. Progression-free survival (PFS) and overall survival (OS) were compared to a control of 58 patients with focal high-grade glioma who received similar therapy, but that included bevacizumab at 10 mg/kg given every two weeks. Results: The patient characteristics were similar in each group. The median PFS and OS for invasive HGG patients were 6 and 13 months and for the focal HGG patients, 11 and 24 months, respectively (P=0.092 and P=0.071). In the subgroup of invasive HGG that showed significant angiogenesis, the median PFS and OS were 3 and 9 months, respectively. 56% of the focal HGG patients recurred as diffuse invasive relapse. For patients with focal HGG who recurred as invasive disease, the median PFS and OS were 9 and 21 months respectively. Conclusions: Presence of diffuse invasive disease not accompanied by angiogenesis either prior to therapy or subsequent to anti-angiogenic therapy does not seem to have prognostic significance. However, invasion accompanied by angiogenesis in newly diagnosed HGG may confer a poor prognosis. Keywords: Angiogenesis, bevacizumab, high-grade glioma, invasion, multifocal glioma
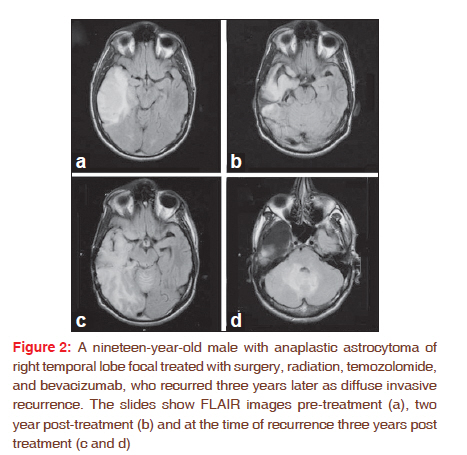
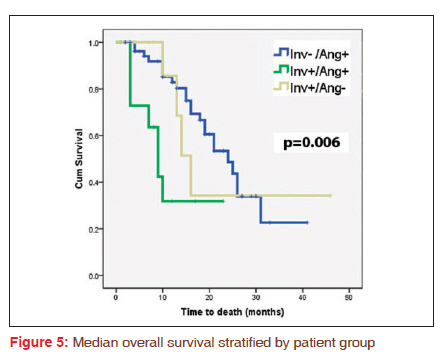
Introduction High-grade gliomas (HGG) are the most common primary brain tumors with a majority of the tumors presenting as localized/ focal disease. [1] For these tumors, treatment generally involves maximal safe surgical resection followed by radiation therapy and chemotherapy with a progression-free survival (PFS) of 6.9 months and overall survival (OS) of 14.6 months in a prospective phase III trial. [2] Age, histologic grade and Karnofsky performance status (KPS), among other covariates, were found to be significant in predicting outcomes in HGG based on the results of three successive Radiation Therapy Oncology Group trials that employed recursive partitioning analysis. [1] Invasive HGG involving multiple lobes is a rare entity at presentation seen in 2-10% of patients. [3],[4],[5],[6] These tumors can vary widely in phenotype, ranging from diffuse, non-enhancing tumor to multiple, discrete, contrast-enhancing lesions. Given the low incidence of invasive HGG, there have been no prospective studies to date. However, based on existing retrospective studies, the prognosis tends to be generally poor, with a PFS of 3-4 months and OS of 7-18 months. [4],[5],[7],[8] A difference in survival appears to exist in this patient population, where patients with gliomatosis were found to have a median overall survival of 16-18 months, compared to 7-9 months in patients with multicentric tumors. [4],[5],[7],[8] Along with increased mitosis and angiogenesis, invasion is a hallmark of HGG as with all other cancers. [9] While invasion may not be readily apparent on conventional imaging early on, it becomes more pronounced with time. [1] The autopsy studies have shown that tumor infiltration occurs up to 2 cm beyond the gross tumor in a majority of the patients. [10] In an effort to improve the outcome, anti-angiogenic therapy is being explored in the treatment of HGG, with bevacizumab (Avastin®; Genentech, South San Francisco, CA) being the most studied agent at this time. [11],[12] Despite impressive radiological responses, both in-vitro and in-vivo studies have demonstrated that bevacizumab tends to increase the incidence of diffuse invasive recurrence (DIR). [13],[14],[15] At this time, it is not clear whether invasion has any prognostic significance on HGG, whether in focal HGG or invasive HGG. The aim of this study is to look at the effect of invasiveness on survival either at the time of original diagnosis or at the time of recurrence following anti-angiogenic therapy. Materials and Methods Institutional review board approval was obtained for the retrospective analysis of 81 consecutive newly diagnosed HGG patients treated at New York University Langone Medical Center and Overlook Hospital from March 2006 to September 2010. All patients had either invasive HGG at initial presentation (n=23), or focal HGG at initial presentation that was treated with bevacizumab-based therapy (n=58). All patients except two with brain stem involvement underwent maximal safe surgical resection at the time of initial diagnosis. Patients with invasive HGG received radiation therapy as either involved field (IFRT) to 59.4 Gy at 1.8 Gy/fraction or whole brain (WBRT) to a dose of 40.05 Gy at 2.67 Gy/fraction. Those who were initially diagnosed with focal HGG received IFRT to a dose of 59.4 Gy at 1.8 Gy/fraction. All patients were treated with concomitant temozolomide at 75 mg/m 2 during radiation, followed by up to 12 months of treatment with temozolomide at 150 mg/m 2 given day 1-5 of 28 day cycle. Focal HGG patients received additional therapy with bevacizumab given intravenously at 10 mg/kg on days 14 and 28 during radiation therapy, and every two weeks thereafter. Diffuse invasive disease at presentation was defined as diffuse T2 or fluid attenuated inversion recovery (FLAIR) changes with involvement of more than two lobes of brain with or without associated contrast enhancing lesions [Figure - 1]. Modified MacDonald′s criteria were used to determine progression, using maximal cross sectional T1 contrast-enhanced images, along with (FLAIR) sequences. [16] A 25% increase in the size of a lesion or the appearance of a new lesion defined progression. In patients with focal HGG, a diffuse invasive disease was defined as an increase in FLAIR changes with or without contrast-enhancement that involved more than two lobes with or without crossing the midline following therapy [Figure - 2]. Local recurrence (LR) was defined as recurrence within a 2 cm margin of the original, primary tumor and/or confined to the lobe. All patients underwent magnetic resonance imaging (MRI) in every two months during follow-up. Kaplan-Meier estimates were used to determine the PFS and OS, and the log rank test was used to compare the survival distributions. Multivariate Cox proportional hazard models were used to determine the extent of the effect of having invasive HGG versus focal HGG in relation to known prognostic factors. Age, KPS, surgical extent, and tumor grade were considered covariates in the Cox model. Patients who were alive at the last follow-up were considered as censored events. A P-value of 0.05 was considered as statistically significant. All calculations were made using the PASW software program (Version 18; PASW Inc., Chicago IL). Results Patient characteristics The patient characteristics are shown in [Table - 1] for the entire patient population. The median age at the time of presentation was 54 years. The median KPS for all patients was 90. Fourteen patients with invasive HGG presented as diffuse non-contrast enhancing disease while 9 patients presented with contrast enhancing multi-centric disease. In the focal HGG group, 20 patients experienced a DIR while 16 failed as an LR. The median time to follow-up was 15.5 months. Local control Fifty patients have experienced a recurrence at the time of analysis. The median PFS was 6 months and 11 months for patients with invasive HGG and focal HGG disease respectively (P=0.092), [Figure - 3]. The median PFS for patients with focal HGG who recurred as DIR compared to those who did not was 9 months and 11 months respectively (P=0.816). In the subgroup of invasive HGG that showed significant angiogenesis, the median PFS was 3 months compared to 9 months in those who did not (P=0.088). Survival Thirty-four patients have died at the time of analysis. The median OS was 13 months and 24 months for patients with invasive HGG and focal HGG, respectively (P=0.071), [Figure - 4]. The median OS for patients with focal HGG who recurred as DIR compared to those who did not was 21 months versus 26 months, respectively (P=0.257). In the subgroup of invasive HGG that showed significant angiogenesis, the median OS was 9 months compared to 16 months in those who did not (P=0.145). For the entire group, the patients who showed both angiogenesis and invasion had the worst survival (P=0.006), [Figure - 5]. Discussion Diffuse invasive disease at the time of diagnosis has a wide spectrum that extends from gliomatosis cerebri with diffuse permeation, minimal contrast enhancement and near normal preservation of neural architecture to multifocal disease with contrast-enhancing lesions scattered throughout the brain in the background of underlying invasive disease. [4],[7] Such a presentation tends to compromise the extent of surgical resection as well as the volume and dose of radiation therapy. However, the impact of such a presentation on survival is not clear. The incidence of diffusive invasive disease at diagnosis is very low, and few publications exist that assess the outcome in these patients. While some small retrospective studies have shown a poor outcome, [5] others have reported outcomes that are not different from focal HGG. [7],[8] It is possible that the poor outcome may not be related to sub-optimal therapy alone and may have more to do with underlying biology that includes both angiogenesis and the invasiveness of the tumor. These results have important implications even in the context of focal HGG, with respect to invasion. Invasion in gliomas is a complex process that involves changes in adhesion characteristics of the tumor cell, degradation of the extracellular matrix and alterations in cytoplasmic contractility that promote tumor cell motility. [17] Untreated HGG generally invades normal brain tissue by infiltrating as single cells into the brain parenchyma, migrating along basement membranes and blood vessels. [18] VEGF, a powerful stimulus that drives angiogenesis, has been shown to block invasion both in vitro and in vivo. [18] In murine glioblastomas derived from transgenic mice that lacked VEGF expression, there was promotion of invasion along blood vessels instead of through parenchyma. [19] A similar mechanism has been noted following bevacizumab therapy with tumor cells migrating as multicellular layers along normal blood vessels using them as conduits into normal tissue or infiltrate through the extracellular matrix. [19] In cases where invasion is a dominant feature at diagnosis, such as in multifocal tumors, the loss of function of p53 in particular can be linked in part to greater invasion observed in this subset due to uncontrolled activation of the proto-oncogene Ets-1. [20],[21],[22] The loss of function of p53 can also cause overexpression of HIF-1α , leading to the upregulation of VEGF and other angiogenic factors. [23],[24] Angiogenesis with contrast enhancement as a surrogate marker is one of the most important prognostic indicators in HGG. [25],[26] While in the context of all HGG, invasion is not necessarily dominant at diagnosis, it does become dominant over time, especially in the setting of anti-angiogenic therapy. In our series as well as others, the subgroup of patients with contrast enhancement and dominant invasion pattern fared the worst. [5] We have also shown that diffuse disease at recurrence does not adversely affect survival. This indicates that invasion by itself is not an independent prognostic factor in HGG, although it potentiates the angiogenesis when present at diagnosis. Though the sample size for this study is small, given that diffuse invasive disease at diagnosis is very rare and that this was not a prospective trial, the numbers were sufficient enough to conclude that invasion is not a prognostic factor. This has an impact on the choice of anti-angiogenic agent and how potential anti-invasive compounds are introduced into therapy. Currently cilengitide-an anti- avb3 and anti- avb5 integrin inhibitor-is being investigated for its efficacy in the treatment of both newly diagnosed and recurrent malignant gliomas. [27],[28] Lithium, which blocks glycogen sythase kinase 3, has shown the ability to block invasion in both spheroid and animal models and is being explored in a phase II clinical trial. [29] Since it is likely that after recurrence the mechanisms for invasion are already active, it may be more efficacious to introduce anti-invasive therapy at diagnosis to maximize the potential benefit. Conclusion The presence of diffuse invasive disease not accompanied by angiogenesis either prior to therapy or subsequent to anti-angiogenic therapy does not seem to have prognostic significance. However, invasion accompanied by angiogenesis appears to confer a poor prognosis. This has an impact on the choice and the timing of anti-angiogenic therapy used in HGG. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11080f4.jpg] [cr11080t1.jpg] [cr11080f1.jpg] [cr11080f3.jpg] [cr11080f5.jpg] [cr11080f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}