 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
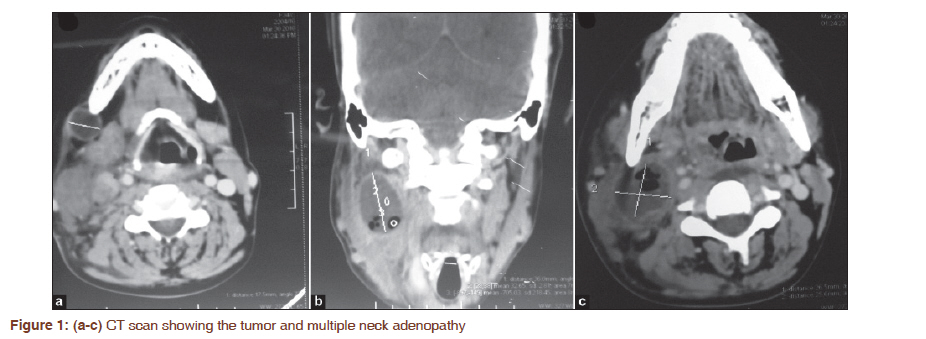
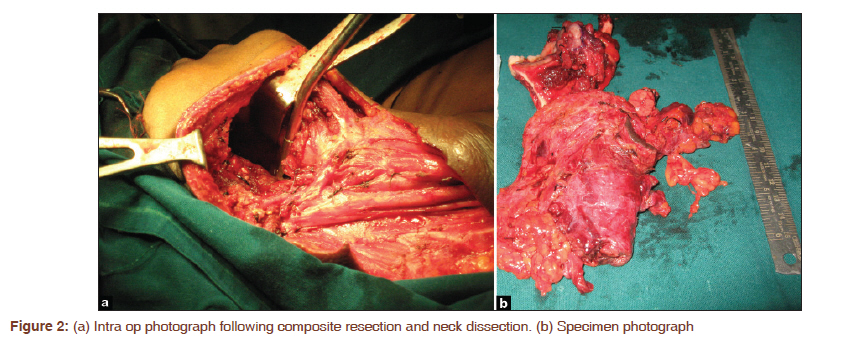
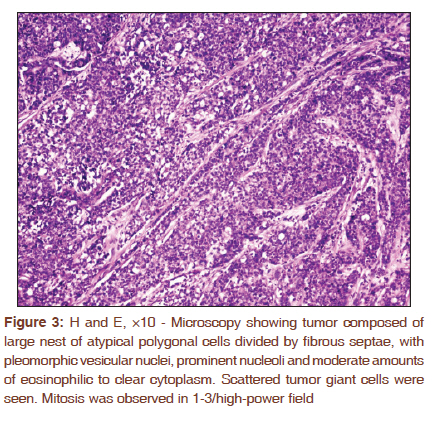
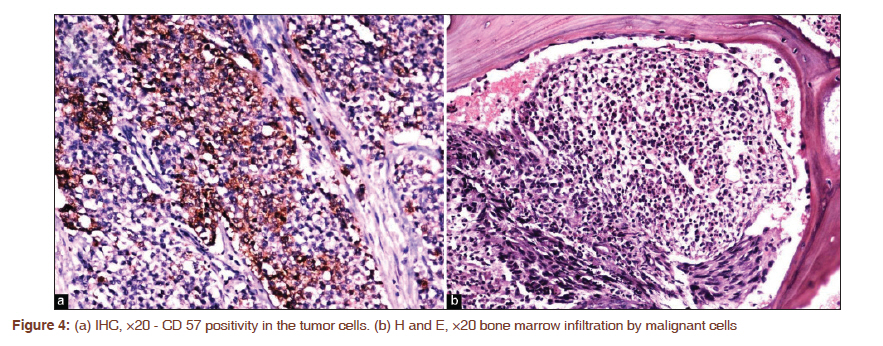
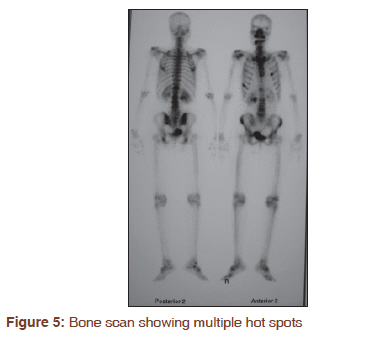
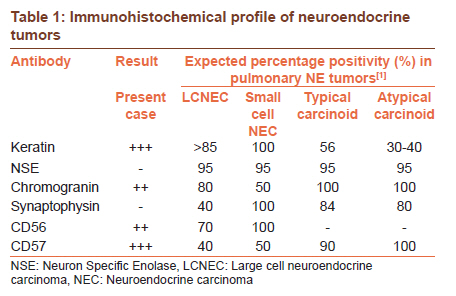
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 343-346 Letter to the Editor - Documenting a Case Large cell neuroendocrine carcinoma of the retromolar trigone Arvind Krishnamurthy1, Anitha Vaidhyanathan1, Urmila Majhi2 1 Department of Surgical Oncology, Division of Pathology, Cancer Institute (WIA), Adyar, Chennai, India Sir, Large cell neuroendocrine carcinoma (LCNEC) is a poorly differentiated and high-grade neuroendocrine neoplasm that has several morphological and biologic features between atypical carcinoid and small cell carcinoma (SCC). [1] Since recognition of LCNEC as pulmonary pathology, several authors describe the incidence of pulmonary LCNEC to range between 2 and 3% of patients diagnosed with lung cancer, with an overall 5-year survival as low as 15%. [1],[2] There are reports of these tumors arising in head and neck subsites, the commonest being the larynx. The salivary glands are perhaps the second most commonest site, the intraoral mucosa is one of the rarest sites for a primary NECs. [3],[4],[5],[6],[7] To the best of our knowledge, this is perhaps the second reported case of a LCNEC with a primary in an intraoral location and the first to manifest with distant metastases and bone marrow infiltration. A 34-year-old lady presented with an ulcer in the right retromolar trigone (RMT), which developed following an extraction of a mobile right lower molar 2 months prior and multiple lymph nodal swellings on the right side of her neck. Physical examination confirmed the ulcer overlying the vertical ramus of mandible and also the multiple significant cervical lymphadenopathy along neck node levels I-III. Her hemogram, chest skiagram and serum biochemistry including alkaline phosphatase levels were normal. Computerized tomography of the head and neck identified the primary 2 × 1.5 cm ulcer in the right RMT with multiple enlarged lymph nodes in the right submandibular, upper and midjugular regions, with the largest right upper jugular node measuring 3.6 × 2.7 × 2.6 cm [Figure - 1]a-c. There was no evidence of involvement of the mandible. A punch biopsy from the tumor was suggestive of a poorly differentiated carcinoma. FNAC from the node demonstrated metastatic deposits from a poorly differentiated carcinoma. She underwent right RMT composite resection and reconstruction with a pectoralis major flap [Figure - 2]a and b. Postoperative microscopy of the specimen revealed ulcerated squamous epithelium with an underlying tumor composed of solid groups of large nest of atypical polygonal cells divided by fibrous septae, with pleomorphic vesicular nuclei, prominent nucleoli and moderate amounts of eosinophilic to clear cytoplasm [Figure - 3]. Scattered tumor giant cells were seen. Mitosis was observed in 1-3/high-power field, some of the atypical cells showed droplet positivity to mucin. Three out of 16 nodes were positive for tumor with extra capsular spread. Immunohistochemical staining was strongly positive for epithelial membrane antigen, keratin, chromogranin, S100P CD56 and CD57 [Figure - 4]a. The tumor cells displayed a negative reaction whereas the lymphoid tissue displayed a positive reaction to leukocyte common antigen, CD43 and CD68. The Ki67-labeling index was 50%. Taking histology and immunohistochemistry into consideration, the diagnosis was in favor of LCNEC-high grade. She was planned for adjuvant chemotherapy and radiation which was started a month after surgery. While on radiotherapy, she developed generalized weakness and bone pains. A bone marrow biopsy revealed atypical cells suggestive of metastatic deposits [Figure - 4]b. A bone scan revealed lesions suspicious for metastatic deposits in the ribs, dorsal and lumbar vertebrae [Figure - 5]. The patient offered to be on supportive care after one cycle of cisplatin and etoposide chemotherapy. At 9 months follow-up, she continues to live with disease. Neuroendocrine tumors are a heterogeneous family of neoplasms with differences in histomorphology, tissue origin, clinical behavior and therapeutic implications. Yao identified 35,618 patients with NECs from The Surveillance Epidemiology and End Results database. They document a significant increase in reported annual age-adjusted incidence from 1973 (1.09/100,000) to 2004 (5.25/100,000). As a result of increased incidence, these tumors represent a substantial clinical problem as they are known to be clinically aggressive and largely resistant to therapy. [8] A recent classification produced by the World Health Organization (2005) comprises of four subtypes of tumors: the low-grade typical carcinoid, the intermediate-grade atypical carcinoid and the two high-grade i.e., LCNEC and small-cell lung carcinoma. [9] It is a characteristic feature that these tumors at their primary site are small and often go unnoticed and are devoid of clinical symptoms till the tumor has metastasized. Our patient presented with a small 2 × 1.5 cm ulceroproliferative lesion at the retromolar trigone and massive metastases to the neck. Iyoda [2] discusses that the final diagnosis of most cases of LCNEC have been accomplished on resected post operative specimens, thereby enabling only retrospective studies on initial presentation and clinical behavior. Similarly, in our case, while FNAC and incisional biopsy were helpful in acquiring a pre operative diagnosis of a poorly differentiated malignancy, both modalities failed to recognize its epithelial neuroendocrine character. While the various subtypes of neuroendocrine neoplasms are marked by different light microscopic appearances, the use of a range of immunohistochemical stains is essential to determine if a neuroendocrine phenotype exists. Neuroendocrine markers such as chromogranin, synaptophysin, S100 and neural cell adhesion molecule (CD56, CD57) are reliable markers and are considered essential to its diagnosis and to distinguish NEC from other tumors [Table - 1]. Aggressive behavior with early dissemination to neighboring organs and lymph nodes is usually expected in such tumors. [1],[10] The occurrence of marrow infiltrates appears to be a rare complication of certain types of NECs. [11] Tritz in their review of 129 patients with SCC of the lung document an incidence of 30% with bone marrow involvement. [11] Thus, while SCC possesses the capacity to metastasize to bone marrow- numerous studies on its counterpart large cell carcinoma variant do not document bone marrow infiltration. [1],[2] Management for oral cavity sub sites of large cell NEC still remains a controversial subject. Surgery is accepted as the primary treatment modality and can be supplemented with postoperative radiotherapy and chemotherapy. To the best of our knowledge, within the category of NECs as primary oral cavity tumors, there exist only one case of LCNEC and three cases of SCCs in the English language literature. [4],[5],[6],[7] Unfortunately due to the rarity of this neoplasm, there is no specific recommendation on management guidelines, treatment options are generally extrapolated from similar tumors of pulmonary origin. It is the author′s opinion that it is important to report single institution experiences of poorly differentiated NECs of the oral cavity, to perhaps aid in forming a consensus on the treatment and its outcomes. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11084f2.jpg] [cr11084t1.jpg] [cr11084f4.jpg] [cr11084f1.jpg] [cr11084f5.jpg] [cr11084f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}