 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
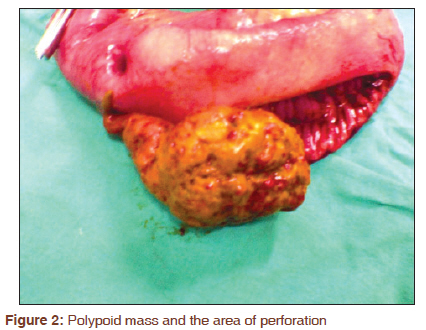
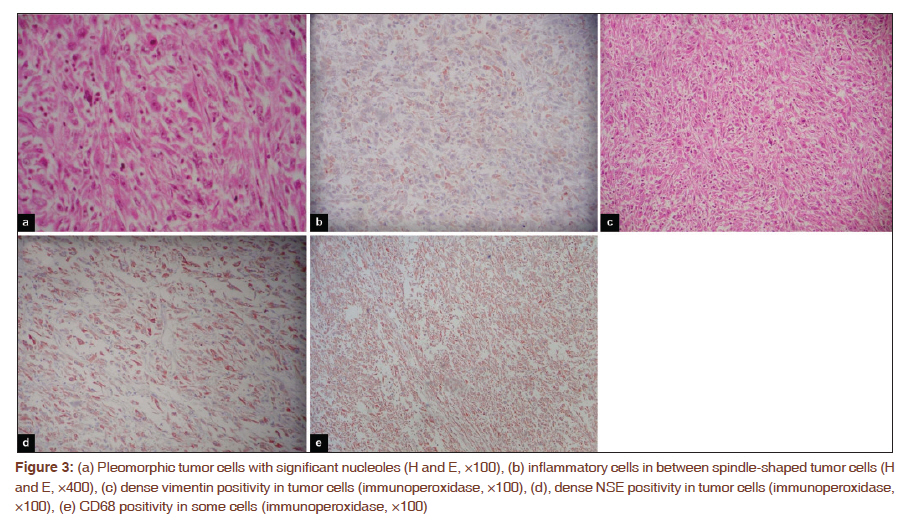
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 348-350 Letter to the Editor - Documenting a Case A rare cause of acute abdomen: Perforated primary sarcomatoid carcinoma of the small intestine - Report of a case, with a brief review of the literature Ahmet Fikret Yucel1, Ahmet Kocakusak2, Soykan Arikan3, Nilgun Demirbag4, Ahmet Tarlaci4, Sebnem Batur4 1 Department of Surgery, Rize University School of Medicine, Rize, Turkey Sir, Sarcomatoid carcinomas (SCA) are primary malignant tumors that basically originate in the lungs. [1] These tumors have also been reported in the thyroid, pancreas, and gallbladder. [2] Primary carcinoma of the small bowel is an uncommon tumor, with an incidence of only 0.5-0.8 per 100000 population per year. [3] Although most of these cases are adenocarcinomas, rare cases of SCA have also been reported. [2],[4] SCAs are more malignant than the more usual adenocarcinoma of the small bowel. Typically, when discovered, primary carcinoma of the small intestine is already in the late stage of disease and follows a rapidly pogressive course. [3] We present the case of a patient, who presented with acute abdomen due to a perforation caused by SCA of the small bowel. A 51-year-old female patient was being followed up by the department of internal medicine because of anemia and abdominal pain, but was referred to the department of general surgery when she developed an acute abdomen. Her examination revealed widespread defence and sensitivity to palpation. Her blood tests were as follows: Hemoglobin 7.2 g/ dl, hematocrit 24.7%, calcium 6.5 mEq/l, amylase 122 U/l, total protein 5.2 g/dl, and albumin 2.7 g/ dl. Other blood tests were normal. X-ray showed free gas under the right diaphragm. As this suggested intestinal perforation, she underwent emergency surgery. Intraoperative exploration revealed acidic fluid contaminated with bile in the peritoneal cavity. Eighty centimeters distal to the Treitz ligament, there was an 8-cm polypoidal mass partially obliterating the lumen of the jejunum and causing mild expansion of the proximal region. There was also conglomerated lymphadenopathies in the meso of the jejunum where the mass was located [Figure - 1]. At the junction of the mass and the jejunal wall there was a 0.5-cm focus of perforation [Figure - 2]. No macroscopic metastatic foci were found. The mass was resected widely, including the meso, and a jejunostomy was performed before closure. The postoperative course was normal and the patient was discharged on the 4 th postoperative day. Histopathological examination of the resected material revealed inflammatory cells between spindle-shaped tumor cells [Figure - 3]a; there were pleomorphic tumor cells with significant nucleoles [Figure - 3]b. Immunohistochemical examination with immunoperoxidase revealed high vimentin [Figure - 3]c and NSE positivity [Figure - 3]d in tumor cells. Some cells had CD68 [Figure - 3]e and cytokeratin positivity. The cells were negative for mucin, CD34, C-kit, chromogranin, synaptophysin, desmin, and HMB-45. As there were no lesions in the lungs, the patient was diagnosed as primary small intestinal sarcomatoid carcinoma. There were metastases in 7 of the 12 lymph nodes resected. The jejunostomy was closed at 3 weeks post surgery and the patient was sent to the medical oncology department for further treatment and follow-up. She, however, died of widespread metastases in the 8 th postoperative week. Primary SCA of the small intestine is generally seen in elderly patients, with the female/male ratio being 1/1.5. [2],[5] These tumors are hard to diagnose as they are rare and have nonspecific symptoms, and also because there are limited diagnostic modalities available. [6],[7] Abdominal pain is the most common symptom, followed by melena, nausea, and vomiting. The presence of these symptoms in a patient is suggestive of small intestinal malignancies. [6] Our patient had complaints of exhaustion and abdominal pain and distension, which had been present for 4 months. Diagnosis was not made till perforation of the intestine had occurred, which resulted in a complicated clinical course and the eventual death of the patient. If diagnostic studies focusing on the small intestine had been done at presentaion 4 months ago, she could have been diagnosed earlier. Abdominal tomography, x-rays with barium, and enteroclysis have been reported to be useful diagnostic tools in these cases. [6] Only abdominal tomography was done for our patient at presentation, and this failed to show any abnormalities. The most effective treatment of malignancy of the small intestine is surgical resection. Intestine 10 cm proximal and distal to the site of the tumor should be removed along with the lymph nodes and the mesentery; this was the treatment we chose for our patient. [8] SCAs have been given different names, depending on the type of cells, cell cultures, and immunohistochemical properties: For example, sarcomatoid carcinoma, carcinosarcoma, pleomorphic carcinoma, undifferentiated carcinoma, pleomorphic giant cell carcinoma, giant cell anaplastic carcinoma, and giant cell carcinoma. [2] Lately, the term ′sarcomatoid carcinoma′ has come to be well accepted and is recommended for routine use in surgical reports. As reported in some cases in the literature, our patient had NSE and chromogranin positivity. Although cytokeratin positivity was suggestive of metastatic carcinoma, we could not detect any other focus of malignancy and so we diagnosed this case as a primary small intestinal malignancy. Small intestinal malignancies have poor prognosis. SCAs have a particularly bad prognosis and when patients are diagnosed at an advanced stage the duration of survival is generally only a few months. [6] Our patient died of widespread lung metastases during her oncology follow-up, 8 weeks after the second operation. In conclusion, primary SCA of the small intestine has a much worse prognosis than other malignant tumors of the small intestine. Early diagnosis has a direct effect on patient survival. In any patient with long-standing abdominal pain with an inapparent cause, anemia, and weight loss, it is mandatory to do diagnostic tests focusing on the small intestine. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11086f1.jpg] [cr11086f2.jpg] [cr11086f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}